Management of benign ureteric stricture
Reading File
Finding Sources
Searching PubMed
"ureteral stricture" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a structured, comprehensive account of the management of benign ureteric strictures, drawn from Campbell-Walsh-Wein Urology and Grainger & Allison's Diagnostic Radiology, with recent evidence noted.
Management of Benign Ureteric Stricture
1. Aetiology
Common causes include:
- Ischaemia / surgical dissection trauma
- Endoscopic instrumentation (ureteroscopy, PCNL)
- Impacted ureteric calculus (>2 months impaction: ~24% stricture rate)
- Radiation
- Infection (tuberculosis, schistosomiasis)
- Periureteral fibrosis (AAA, endometriosis, retroperitoneal fibrosis)
- Post-renal transplant (ischaemic, BK virus, CMV)
- Idiopathic
Always rule out malignancy before treating as benign. TCC can mimic a benign stricture, and extrinsic lesions (cervical, prostate, ovarian, colon, breast cancers) may present identically.
(Campbell-Walsh-Wein Urology, p. 2618)
2. Diagnostic Evaluation
| Investigation | Purpose |
|---|---|
| CT scan | Initial detection of obstruction; rule out malignancy or extrinsic mass |
| CT urography / retrograde or antegrade pyelogram | Define stricture location and length |
| Ureteroscopy with biopsy / barbotage | Mandatory when cause is uncertain |
| Diuretic renography (MAG-3 or DTPA) | Quantify differential renal function; determine if obstruction is functionally significant |
Indications for intervention: suspected malignancy, ongoing renal obstruction, recurrent pyelonephritis, pain from functional obstruction.
3. Management Algorithm
The key determinants are stricture length, renal function (ipsilateral moiety), and stricture location:
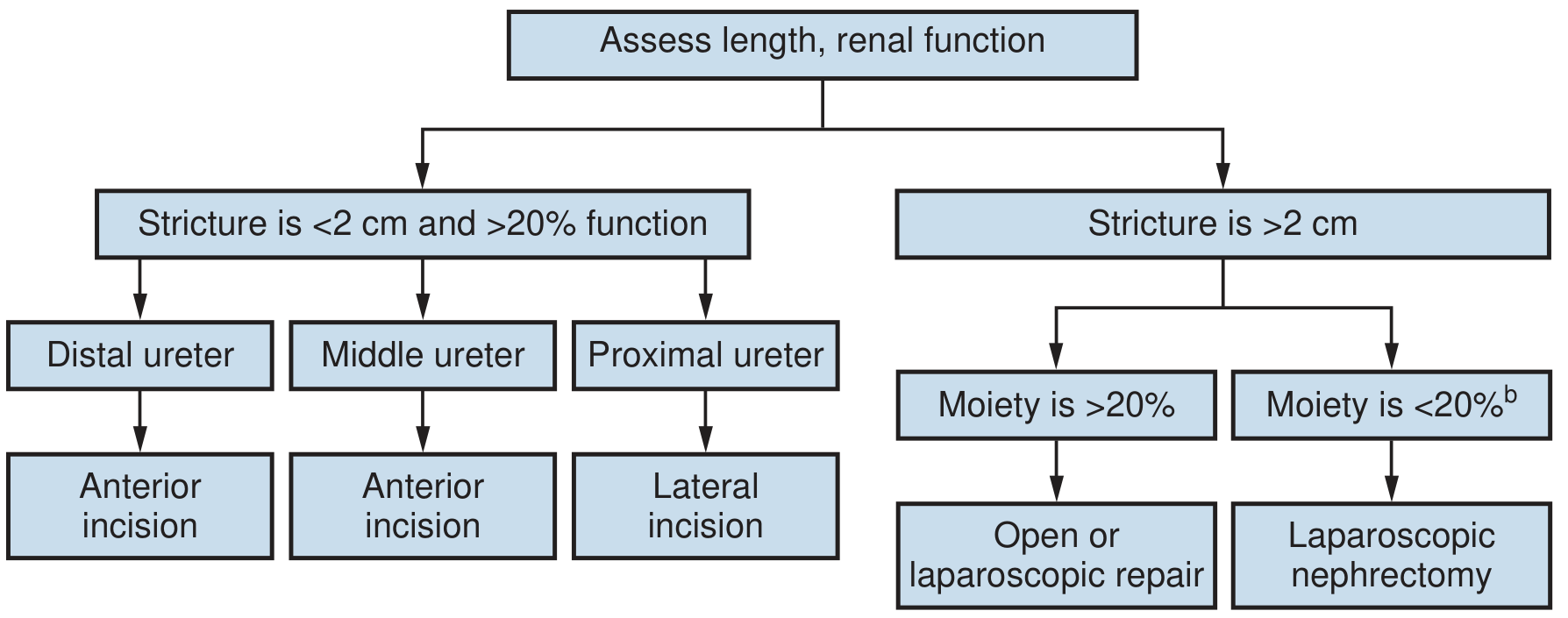
- Stricture <2 cm AND >20% ipsilateral function → Endourological (endoureterotomy, direction of incision varies by location)
- Stricture >2 cm AND >20% function → Open or laparoscopic surgical repair
- Stricture >2 cm AND <20% function → Consider nephrectomy (laparoscopic); select paediatric patients and those with renal insufficiency may still warrant repair
- Transplant patients on immunosuppression → Prefer balloon dilation first
4. Endourological Options
A. Ureteral Stent Placement
- Effective for acute decompression of intrinsic strictures (88% success at 26 months for intrinsic obstruction)
- Extrinsic compression eventually requires percutaneous drainage or surgery
- Stents alone rarely produce long-term cure but are useful in:
- Patients unfit for surgery or with poor prognosis
- Temporisation while awaiting definitive repair
- Patients on systemic therapy for malignancy
- Tandem stenting (two parallel stents): useful when single stent fails; 0% failure in one series for benign extrinsic obstruction
- Metal stents (thermoexpandable or full metallic): for long-term palliation in select patients; complications include encrustation, migration, and infection; exchange at 12-month intervals
(Campbell-Walsh-Wein, p. 2619-2620)
B. Balloon Dilatation
- Overall success rate 16-83%; highest for early post-transplant strictures, early post-PCNL/ureterolithotomy strictures, and proximal well-circumscribed strictures
- Lower success at the vesicoureteric junction (VUJ) and in ischaemic strictures
- Long strictures (≥3 cm) respond poorly
- Technique: access via interpolar calyx, use hydrophilic wire to cross stricture, exchange for stiff wire, dilate with 6-8 mm balloon at high pressure until waist disappears; leave ureteric stent as splint for 4-6 weeks
- Failure of balloon dilatation does not preclude subsequent surgery - it is therefore the procedure of choice for transplant ureteric strictures
- Cutting balloon angioplasty: for resistant strictures; primary patency 55%, secondary patency 78% in post-transplant ureter
(Grainger & Allison's Diagnostic Radiology, p. [balloon dilatation section])
C. Endoureterotomy (Incision of stricture)
The dominant approach is retrograde holmium laser endoureterotomy.
- Incision direction:
- Distal and middle ureter: anterolateral incision
- Proximal ureter: lateral incision (avoids iliac vessels and gonadal vessels medially)
- Incision is full-thickness to periureteral fat, encompassing 2-3 mm of normal tissue proximally and distally
- Post-incision stenting with large-diameter stents (8-12 Fr) improves results
- Triamcinolone injection after endoureterotomy may improve outcomes
- Success rates: 66-83% at >12 months follow-up for strictures <2 cm
- Poor results with retrograde approach for strictures >2 cm
- Stone-related strictures may have lower success (~56%)
Antegrade approach is used when retrograde ureteroscopic access fails:
- Percutaneous nephrostomy is established first, infection/compromised function is allowed to resolve, then percutaneous tract is dilated to allow a flexible ureteroscope
Combined retrograde + antegrade approach: for areas of complete ureteral obliteration (rare).
5. Open / Laparoscopic / Robotic Surgical Repair
The approach is dictated by the location and length of the stricture:
Distal Ureteral Strictures
| Technique | Indication |
|---|---|
| Ureteroneocystostomy (direct reimplantation) | Short distal stricture, adequate bladder capacity |
| Psoas hitch | Adds 4-5 cm; bridges defects of lower/mid ureter |
| Boari flap | Bridges longer mid-ureteric defects (up to 15 cm with psoas hitch combined) |
Mid-Ureteral Strictures
- Uretero-ureterostomy (end-to-end anastomosis): for short gaps after adequate mobilisation, spatulated anastomosis over a stent
- Transureteroureterostomy (TUU): when ureteral length is insufficient to reach the bladder; donor ureter tunnelled under sigmoid mesentery to recipient ureter; contraindicated if recipient ureter is diseased or donor ureter is too short; relative contraindications include nephrolithiasis, RPF, urothelial malignancy, prior pelvic radiation
Proximal Ureteral Strictures / Long/Panureteral Strictures
- Ileal ureter substitution: entire ureter replaced with an isoperistaltic segment of ileum; used for long or panureteral strictures (e.g., post-TB multiple strictures); contraindicated in renal insufficiency (metabolic acidosis risk), bowel disease, prior pelvic radiation
- Renal mobilisation (renal decensus): frees up to 8 cm of length; kidney mobilised and fixed inferiorly on its vascular pedicle; can be combined with Boari flap for panureteral strictures
- Appendix ureteroplasty / buccal mucosa graft ureteroplasty: augmentation techniques for long strictures not amenable to resection; robotic-assisted buccal mucosa graft ureteroplasty is gaining traction (recent systematic review PMID: 41408485)
Laparoscopic / Robotic Approach
All the above procedures can be performed laparoscopically or robotically with equivalent success rates and less morbidity than open surgery. Laparoscopic approaches are now standard for most centres with appropriate expertise.
6. Special Situations
Post-Transplant Ureteric Stricture
- Affect 1-9% of transplants; most strictures >3 months post-transplant are ischaemic
- Priority: decompress with nephrostomy/stent first
- Retrograde stenting can be technically difficult due to location of neoureteral orifice
- Antegrade nephrostomy provides best access
- Endourological: holmium laser endoureterotomy 67-83% success at 44-58 months
- Balloon dilatation: success 16-81% (best with early-onset short strictures)
- Surgical: open ureteric reimplantation for failed endoscopic treatment
Retroperitoneal Fibrosis
- Ureteral stents, balloon dilation, or steroids (corticosteroids reduce fibrous tissue) as initial treatment
- Ureterolysis (surgical) for definitive treatment in non-responders
Radiation-induced strictures
- Tend to be ischaemic and respond poorly to balloon dilation
- Ileal replacement is often required for definitive repair
7. Summary of Success Rates
| Intervention | Success Rate |
|---|---|
| Balloon dilation (general) | 16-83% |
| Balloon dilation (post-transplant) | 16-81% (up to 81% in best series) |
| Holmium laser endoureterotomy (<2 cm) | 66-83% |
| Open/laparoscopic repair | >85-90% (most series) |
Recent evidence:
- A 2025 meta-analysis (PMID: 41408485) comparing robotic vs. laparoscopic/open buccal mucosa graft ureteroplasty shows robotic approaches are safe and effective for complex strictures.
- A 2025 systematic review/meta-analysis (PMID: 40465801) on segmental metal ureteral stents for long-term maintenance therapy found no significant difference between stent types across years, supporting their role in patients unfit for surgery.
- A 2024 systematic review (PMID: 38185833) confirmed endourological management as the first-line approach for transplant ureteric strictures, with surgical revision reserved for failures.
Sources: Campbell-Walsh-Wein Urology (9780323546423), pp. 2618-2630; Grainger & Allison's Diagnostic Radiology (9780323760751), balloon dilatation section
This is a shared conversation. Sign in to Orris to start your own chat.