What are the thing that should include I exam if TB as topic came
🫁 Tuberculosis (TB) - Complete Exam Guide
1. Etiology & Microbiology
- Causative organism: Mycobacterium tuberculosis (most common) - part of the M. tuberculosis Complex (MTBC)
- Other MTBC members: M. bovis, M. africanum, M. microti, M. canettii
- Key properties:
- Acid-fast bacillus (AFB) - Ziehl-Neelsen stain (red rods on blue background)
- Obligate aerobe - explains predilection for upper lobes
- Slow dividing (18-24 hour generation time)
- Non-motile, non-spore forming
- Waxy, lipid-rich cell wall (mycolic acids) - responsible for acid-fastness, resistance to killing, and granuloma formation
- ESX-1 Type VII secretion system secretes ESAT-6 and CFP-10 (virulence factors, also used in IGRA tests)
- Genome: 4 Mb circular genome, encoding ~4006 proteins; phylogenetically 7 major branches with geographic distribution
2. Epidemiology
- Leading infectious disease killer worldwide (surpassing HIV)
- High burden countries: India, China, Indonesia, Philippines, Pakistan, Nigeria, South Africa
- Risk factors for infection:
- Close household contact with active TB case
- Overcrowding, poor ventilation
- HIV/AIDS (greatest single risk factor)
- Poverty, malnutrition, homelessness
- Healthcare workers
- Prisoners/institutional settings
- Risk factors for reactivation (LTBI to active TB):
- HIV (highest risk - 5-10% per year vs 5-10% lifetime in immunocompetent)
- TNF-alpha antagonists (infliximab, etanercept) - major risk, screen before starting
- DM, CKD, malnutrition, silicosis
- Corticosteroids, immunosuppressants
- Young age (<5 years), old age
3. Transmission
- Route: Airborne droplet nuclei (1-5 microns diameter)
- Source: Pulmonary/laryngeal TB patients (especially smear-positive, cavitary disease)
- Droplet nuclei survive 3-9 hours in air under standard conditions
- Environmental factors affect risk: ventilation, UV light exposure, air exchanges
- Close household contacts: ~50% become infected; ~15% non-close contacts
- Rate of TB ~15 per 1000 close contacts vs ~3 per 1000 non-close contacts
4. Pathogenesis
4a. Primary Infection
- Inhaled droplet nuclei reach alveoli
- Engulfed by alveolar macrophages (primary host cell)
- M. tb survives intracellularly - blocks phagosome-lysosome fusion (ESX-3 via EsxH)
- Bacilli replicate, macrophages spread to regional lymph nodes
- Ghon focus (parenchymal lesion) + hilar lymphadenopathy = Ghon complex (Ranke complex)
- Bacilli may enter bloodstream (occult bacteremia) - seeding multiple sites
4b. Granuloma Formation (Key)
- Hallmark: caseating granuloma (caseous necrosis in center)
- Structure: Central caseous necrosis → Epithelioid macrophages → Multinucleated Langhans giant cells → Rim of lymphocytes → Fibroblasts
- Cell-mediated immunity (CD4+ T cells, IFN-gamma, TNF-alpha) critical for containment
- TST/IGRA positivity develops 2-8 weeks after infection
4c. Latent TB Infection (LTBI)
- Bacilli remain dormant within granulomas
- No symptoms, not infectious, positive TST/IGRA
- Reactivation risk when immunity wanes
4d. Post-primary (Reactivation) TB
- Apical and posterior segments of upper lobes (high O2 tension)
- Cavitation occurs - enormously infectious
- Fibrocaseous disease, bronchogenic spread
5. Clinical Features
Pulmonary TB (most common, ~80%)
| Symptom | Detail |
|---|---|
| Cough | Persistent >2-3 weeks, initially dry then productive |
| Hemoptysis | Blood-streaked or frank hemoptysis |
| Fever | Low-grade, afternoon/evening |
| Night sweats | Drenching |
| Weight loss | Significant, with anorexia |
| Fatigue/malaise | Chronic |
| Chest pain | Pleuritic if pleural involvement |
| Dyspnea | With extensive disease |
- Constitutional symptoms (B symptoms): fever, night sweats, weight loss - classic triad
- Examination: Dullness/bronchial breathing at apex, post-tussive crepitations
- CXR findings: Apical infiltrates, cavities, fibrosis, calcification, pleural effusion, miliary nodules
6. Extrapulmonary TB (EPTB)
| Site | Key Features |
|---|---|
| Lymph node TB | Most common EPTB; cervical > mediastinal; painless, matted nodes; may form collar-stud abscess (sinus tract) |
| Pleural TB | Exudative effusion, lymphocytic, high ADA (>40 U/L); protein >3 g/dL |
| TB Meningitis | Most severe; subacute onset; basal meningeal enhancement on MRI; CSF: lymphocytosis 10-500/μL, high protein >1 g/L, low glucose; cranial nerve palsies (III, IV, VI, VII); hydrocephalus |
| Miliary TB | Hematogenous dissemination; "millet seed" nodules on CXR (2-3 mm); involves lung, liver, spleen, bone marrow; choroid tubercles in eye |
| Skeletal TB | Spine (Pott's disease) most common; L1 affects lower thoracic/upper lumbar; gibbus deformity; cold abscess; paraplegia |
| Renal/Urogenital | Sterile pyuria, hematuria, "putty kidney" calcification; epididymo-orchitis in males |
| Pericardial TB | Pericardial effusion → constrictive pericarditis; raised JVP, Kussmaul's sign |
| GI TB | Ileocecal most common; mimics Crohn's; "pipe stem" appearance; abdominal TB with ascites |
| Adrenal TB | Can cause Addison's disease (adrenal insufficiency) |
7. Diagnosis
7a. Tuberculin Skin Test (TST / Mantoux)
- 0.1 mL of 5 TU PPD injected intradermally; read at 48-72 hours
- Interpretation of induration (not erythema):
| Cutoff | Population |
|---|---|
| ≥5 mm | HIV+, recent contact, immunosuppressed, CXR with old TB, transplant |
| ≥10 mm | Recent immigrants from endemic areas, IV drug users, health care workers, children <4 years |
| ≥15 mm | Low-risk individuals |
- False negative: HIV/immunosuppression, miliary TB, recent viral illness, malnutrition, improper technique
- False positive: BCG vaccination, NTM infection (Mantoux <15mm usually from BCG)
- Booster effect (two-step testing): for healthcare workers
7b. Interferon-Gamma Release Assays (IGRAs)
- QuantiFERON-TB Gold Plus (QFT-Plus), T-SPOT.TB
- Blood test; measures IFN-gamma response to ESAT-6 and CFP-10 antigens
- Advantages over TST: Not affected by BCG vaccination; more specific; single visit
- Preferred in BCG-vaccinated populations
- Same uses as TST - diagnoses LTBI, NOT active disease
7c. Sputum Microscopy (AFB Smear)
- 3 sputum specimens (at least 2): early morning preferred
- Ziehl-Neelsen (ZN) stain or fluorescent auramine-rhodamine stain
- Sensitivity 60-80% in smear-positive; lower for smear-negative, extrapulmonary
- Grade smear: 1+ to 4+ or scanty
- Requires 5000-10,000 bacilli/mL to be smear positive
- Cannot distinguish M. tuberculosis from NTM
7d. Mycobacterial Culture (Gold Standard)
- Lowenstein-Jensen (LJ) medium: solid, buff-colored, rough, raised colonies; 6-8 weeks
- Middlebrook 7H9/7H10/7H11: liquid and solid
- BACTEC MGIT (automated liquid): faster, 1-3 weeks
- Can distinguish species and perform Drug Susceptibility Testing (DST)
7e. Nucleic Acid Amplification Tests (NAATs)
- Xpert MTB/RIF (CBNAAT/GeneXpert): WHO-recommended first-line rapid test
- 2-hour turnaround; detects M. tb AND rifampicin resistance (rpoB gene) simultaneously
- Sensitivity: ~90% smear+, ~70% smear- cases
- Point-of-care available
- Xpert MTB/RIF Ultra: more sensitive than original (especially smear-negative, TBM)
- Line Probe Assays (LPA): GenoType MTBDRplus - rapid DST for isoniazid and rifampicin resistance; GenoType MTBDRsl for fluoroquinolone/second-line resistance
7f. Additional Investigations
| Test | Role |
|---|---|
| CXR | Screening and follow-up |
| HRCT Chest | Better than CXR; "tree-in-bud" pattern, cavities, miliary nodules |
| Bronchoscopy + BAL | Smear-negative cases |
| ADA (Adenosine Deaminase) | Pleural fluid/CSF/ascites (>40 U/L in pleural TB) |
| Pleural biopsy | Granulomas on histology |
| LFTs, CBC, renal function | Pre-treatment baseline |
| HIV testing | Mandatory in all TB patients |
| Blood sugar | Screen for DM |
8. Treatment
First-Line Anti-TB Drugs (RIPE / HRZE)
| Drug | Abbreviation | Mechanism | Key Side Effect |
|---|---|---|---|
| Rifampicin | R | Inhibits RNA polymerase (β-subunit, rpoB gene) | Hepatotoxicity, orange-red discoloration of secretions, drug interactions (CYP450 inducer) |
| Isoniazid | H | Inhibits mycolic acid synthesis (InhA/KatG) | Peripheral neuropathy (give pyridoxine B6), hepatotoxicity, lupus-like syndrome |
| Pyrazinamide | Z | Unknown (disrupts membrane energy) | Hepatotoxicity, hyperuricemia/gout, arthralgia |
| Ethambutol | E | Inhibits arabinosyl transferase (embB - arabinogalactan synthesis) | Optic neuritis (red-green color blindness, visual acuity) - dose-dependent |
| Streptomycin | S | Inhibits 30S ribosome (aminoglycoside) | Ototoxicity (VIII nerve), nephrotoxicity |
Standard Treatment Regimen
- 2 HRZE / 4 HR (6 months total)
- Intensive phase: 2 months - HRZE (Isoniazid + Rifampicin + Pyrazinamide + Ethambutol)
- Continuation phase: 4 months - HR (Isoniazid + Rifampicin)
- TB Meningitis/Bone/Pericardial: 2 HRZE / 10 HR (12 months total)
- Directly Observed Therapy (DOT) - mandatory to prevent resistance
LTBI Treatment Options
| Regimen | Duration | Notes |
|---|---|---|
| 6H (INH) | 6 months | Classic, widely used |
| 9H (INH) | 9 months | Preferred in US guidelines |
| 3HP (INH + Rifapentine weekly) | 3 months | Newer, preferred in some settings |
| 4R (Rifampicin alone) | 4 months | If INH not tolerated |
9. Drug Resistance
| Type | Definition |
|---|---|
| MDR-TB | Resistant to at least Rifampicin + Isoniazid |
| Pre-XDR-TB | MDR-TB + resistant to any fluoroquinolone |
| XDR-TB | MDR-TB + resistant to any fluoroquinolone + at least one of bedaquiline or linezolid |
| RR-TB | Rifampicin-resistant (treated same as MDR) |
- BPaL (Bedaquiline + Pretomanid + Linezolid) - approved for XDR-TB and treatment-intolerant MDR-TB (TB-PRACTECAL/ZeNix trials)
- BPaLM - adds Moxifloxacin (6-month regimen)
- Second-line drugs: Fluoroquinolones (levofloxacin, moxifloxacin), bedaquiline, linezolid, clofazimine, cycloserine, delamanid
- Duration: typically 18-24 months for MDR-TB
10. TB & HIV Co-infection
- HIV is the biggest risk factor for TB - 20-30x increased risk
- CD4 <200: more atypical presentations (lower lobe, no cavities, miliary)
- IRIS (Immune Reconstitution Inflammatory Syndrome): worsening of TB symptoms after starting ART
- Start ART 2 weeks after anti-TB therapy if CD4 <50; 8 weeks if CD4 >50
- Rifampicin interacts with many ARVs (CYP450 inducer) - substitute rifabutin if on protease inhibitors
- HIV testing is mandatory in all TB patients
11. TB Meningitis (High-Yield)
- Clinical criteria (max 6 pts): symptom duration >5 days (4 pts), systemic TB symptoms (2 pts), focal deficits (1 pt), CN palsy (1 pt), altered consciousness (1 pt)
- Imaging criteria (max 6 pts): basal meningeal enhancement (2 pts), tuberculoma (2 pts), precontrast basal hyperdensity (2 pts), hydrocephalus (1 pt), infarct (1 pt)
- CSF criteria (max 4 pts): lymphocytosis 10-500/μL, protein >1 g/L, glucose <2.2 mmol/L
- Score: ≥12 = definite; 10-11 = probable; 6-9 = possible; <6 = non-TB
- NAAT for TBM: sensitivity 56%, specificity 98% (meta-analysis)
- Treatment: 2 HRZE + 10 HR + dexamethasone (adjunct, reduces mortality)
12. Prevention & Control
- BCG vaccine: given at birth; protects against miliary TB and TBM in children (60-80%); does NOT reliably prevent pulmonary TB in adults
- Infection control (4 categories):
- Clinician awareness - rapid diagnosis
- Administrative controls - respiratory isolation, surgical masks for patients
- Environmental controls - ventilation (negative pressure rooms), UV germicidal irradiation, air exchanges
- Personal protective equipment (PPE) - N95 respirator for HCWs entering isolation rooms
- Contact tracing: screen all household contacts (TST/IGRA, symptom screen, CXR)
- DOTS strategy (WHO): Directly Observed Therapy, Short-course - cornerstone of national programs
- END TB Strategy (WHO): target <10 cases/100,000 by 2035
13. Special Scenarios (High Yield for Exams)
| Scenario | Key Point |
|---|---|
| TNF-alpha inhibitors (infliximab) | Screen with TST/IGRA + CXR before starting; treat LTBI first |
| Steroids in TB | Only for TBM and pericardial TB (reduces constrictive pericarditis) |
| Pregnancy | Rifampicin, INH, Ethambutol safe; avoid Streptomycin (ototoxic to fetus) and Pyrazinamide (caution) |
| Renal failure | Reduce dose of Ethambutol and Streptomycin (renally cleared) |
| Hepatotoxicity monitoring | Stop all drugs if ALT >3x ULN with symptoms or >5x ULN without symptoms |
| Pott's disease | Collapse L1 vertebrae → "gibbus"; cold abscess tracking down psoas muscle |
| Cold abscess | TB lymph node/spine abscess - NOT warm, NOT tender (unlike pyogenic) |
| Choroid tubercles | Pathognomonic of miliary TB on fundoscopy |
14. Summary: Exam Quick Points
- AFB stain = Ziehl-Neelsen; Culture = LJ medium (gold standard)
- Ghon focus = parenchymal lesion; Ghon complex = focus + hilar lymph node
- CBNAAT (Xpert MTB/RIF) = detects TB + rifampicin resistance simultaneously
- ADA elevated in pleural, peritoneal, and CSF TB
- Ethambutol - optic neuritis; INH - peripheral neuropathy (give B6/pyridoxine); Rifampicin - orange urine
- MDR-TB = resistant to R + H; XDR-TB adds fluoroquinolone + bedaquiline/linezolid resistance
- BCG protects children from miliary/meningeal TB, NOT adult pulmonary TB
- IGRA preferred in BCG-vaccinated populations (not affected by BCG)
- HIV = start ART after 2 weeks if CD4 <50, 8 weeks if CD4 >50
- DOT (Directly Observed Therapy) = mandatory to prevent resistance
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 1164-1253
- Tintinalli's Emergency Medicine, Ch. 6
I don't understand the diagnosis do providing insimple way
🔬 TB Diagnosis - Made Simple
STEP 1 - Suspect TB (Clinical)
- Cough for >2 weeks?
- Night sweats + weight loss + fever?
- Contact with a TB patient?
- HIV positive?
STEP 2 - Take an X-Ray
- White patches at the top of the lungs (upper lobe infiltrates)
- Holes (cavities) - very suspicious
- Miliary TB = "millet seeds" scattered all over
STEP 3 - Test the Sputum
🔴 Test A - AFB Smear (Fast, Cheap)
- Patient spits sputum (3 samples, early morning best)
- Stain it with Ziehl-Neelsen (ZN) stain
- Seen under microscope as red rods on blue background
- Result in: same day
- Problem: doesn't confirm M. tuberculosis (could be other mycobacteria)
🟡 Test B - CBNAAT / GeneXpert (Fast + Smart)
- Same sputum sample
- Machine detects TB's DNA in 2 hours
- Also tells you if TB is resistant to Rifampicin (MDR-TB)
- WHO recommends this as first test
- Think of it as: "Google search for TB DNA"
🟢 Test C - Culture (Gold Standard but Slow)
- Grow the bacteria on LJ medium in a lab
- Takes 6-8 weeks (bacteria grow very slowly)
- Confirms exact species + which drugs it's sensitive to
- Best test, but too slow for starting treatment
STEP 4 - Test for Past Exposure / Latent TB
🩺 Mantoux Test (TST)
- Inject a small amount (PPD) under the skin of the forearm
- Come back after 48-72 hours
- Measure the bump (induration) - NOT the redness
- If bump ≥ 10 mm → positive (likely been infected)
- Problem: BCG vaccination can give a false positive
🩸 IGRA / QuantiFERON (Blood Test)
- A blood test - measures immune response to TB proteins
- Not affected by BCG vaccine → more accurate in India
- Same idea as Mantoux but done in a lab
⚠️ Both Mantoux and IGRA only tell you "infected before" - they CANNOT tell if TB is active right now
ADA Test (Special Situation)
- Check ADA (Adenosine Deaminase) level in that fluid
- If ADA > 40 U/L → strongly suggests TB
- Simple blood-like test done on the fluid sample
🧠 Simple Memory Table
| Test | What it finds | Time | Used when |
|---|---|---|---|
| AFB Smear (ZN) | Bacteria under microscope | Hours | First quick check |
| GeneXpert/CBNAAT | TB DNA + drug resistance | 2 hours | Best first-line test |
| Culture (LJ) | Grows actual bacteria | 6-8 weeks | Gold standard |
| Mantoux/TST | Past exposure (skin bump) | 48-72 hrs | Latent TB screening |
| IGRA (blood) | Past exposure (blood test) | 1 day | Better than Mantoux in BCG-vaccinated |
| ADA | TB inflammation marker | Hours | Pleural/CSF/ascites TB |
🎯 One-Line Rule for Exams
Smear = quick screen → GeneXpert = confirm + resistance → Culture = gold standard → Mantoux/IGRA = latent TB only
Ok then classification offirst line anti tubercular drugs it's common adverse effect ,drugs interaction , nursing implications in simple way for exam
💊 First-Line Anti-TB Drugs - Simple Exam Guide
Memory Trick: "RIPE" or "HRZE"
Rifampicin + Isoniazid + Pyrazinamide + Ethambutol
🔴 Drug 1 - RIFAMPICIN (R)
Classification
- Rifamycin antibiotic - bactericidal (kills bacteria)
- Most powerful sterilizing drug in the regimen
Mechanism (simple)
Blocks the bacteria's ability to make RNA
- Inhibits DNA-dependent RNA polymerase (β-subunit / rpoB gene)
- Without RNA → bacteria cannot make proteins → bacteria die
Common Adverse Effects
| Effect | What Patient Feels |
|---|---|
| 🟠 Orange-red discoloration | Urine, sweat, tears, saliva all turn orange - HARMLESS |
| 🤢 GI upset | Nausea, vomiting, abdominal pain |
| 🫁 Hepatotoxicity | Liver damage - monitor LFTs |
| 🤧 Flu-like syndrome | Fever, chills, muscle ache (especially with intermittent dosing) |
| 🔴 Thrombocytopenia | Low platelets → bleeding risk |
| 🌡️ Hypersensitivity | Rash, fever |
Drug Interactions ⚠️
- Rifampicin is a STRONG CYP450 enzyme INDUCER
- It SPEEDS UP the breakdown of many drugs → their levels fall
| Drug affected | Result |
|---|---|
| Oral contraceptive pills (OCP) | OCP fails → unwanted pregnancy |
| Warfarin | Anticoagulation reduced → clot risk |
| HIV drugs (protease inhibitors) | ARV levels drop → treatment failure |
| Antifungals (fluconazole) | Reduced effect |
| Digoxin, steroids, methadone | All reduced |
💡 Exam Tip: "Rifampicin reduces the effect of OCP" is a classic MCQ
Nursing Implications
- ✅ Warn patient urine/tears/sweat will turn orange - this is NORMAL, not blood
- ✅ Warn patients using contact lenses - lenses will stain orange permanently
- ✅ Tell female patients on OCP to use barrier contraception
- ✅ Take on empty stomach (1 hour before or 2 hours after food) for best absorption
- ✅ Monitor liver function tests (LFTs) regularly
- ✅ Do NOT give in severe liver disease
🟡 Drug 2 - ISONIAZID (H / INH)
Classification
- Isonicotinic acid hydrazide - bactericidal (strongest early-killing drug)
- Prodrug - activated by the bacterial enzyme KatG
Mechanism (simple)
Stops the bacteria from building its protective waxy coat (cell wall)
- Inhibits mycolic acid synthesis (InhA enzyme)
- Without mycolic acid → bacteria's cell wall breaks → bacteria die
Common Adverse Effects
| Effect | What Patient Feels |
|---|---|
| 🦶 Peripheral neuropathy | Tingling/numbness/burning in hands and feet (MOST COMMON) |
| 🫁 Hepatotoxicity | Liver damage (common, especially in elderly, alcoholics) |
| 🧠 CNS effects | Dizziness, memory problems, rarely seizures |
| 💊 Drug-induced lupus | Joint pain, rash, ANA positive |
| 😴 Pyridoxine (B6) deficiency | Leads to the neuropathy above |
Drug Interactions
| Drug | Result |
|---|---|
| Phenytoin | INH inhibits phenytoin metabolism → phenytoin toxicity (ataxia, nystagmus) |
| Alcohol | Increases hepatotoxicity risk dramatically |
| Antacids (aluminium) | Reduce INH absorption - give 1 hour apart |
| Warfarin | INH increases warfarin effect → bleeding risk |
Nursing Implications
- ✅ Always give Pyridoxine (Vitamin B6) 25-50 mg/day with INH to prevent peripheral neuropathy
- Especially important in: diabetics, alcoholics, malnourished, pregnant women, elderly
- ✅ Monitor for tingling/numbness in hands and feet (early neuropathy sign)
- ✅ Monitor liver function tests - warn about signs of hepatitis (yellow eyes, dark urine)
- ✅ Take on empty stomach (food reduces absorption)
- ✅ Avoid alcohol completely
- ✅ Monitor phenytoin levels if patient is on anti-epileptics
🟢 Drug 3 - PYRAZINAMIDE (Z / PZA)
Classification
- Nicotinamide analogue - bactericidal in acidic environments
- Prodrug - activated by pyrazinamidase to pyrazinoic acid (POA)
- Only drug that works inside acidic macrophages (where TB hides)
Mechanism (simple)
Works inside the acidic environment of macrophages to kill hidden bacteria
- Disrupts mycobacterial membrane energy + inhibits fatty acid synthesis
- Uniquely active at acidic pH (inside phagolysosomes)
- Allows treatment to be shortened from 9 months to 6 months
Common Adverse Effects
| Effect | What Patient Feels |
|---|---|
| 🫁 Hepatotoxicity | MOST HEPATOTOXIC of all first-line drugs |
| 🦴 Hyperuricemia | High uric acid → gout (joint pain, especially big toe) |
| 🦵 Arthralgia | Joint pain, muscle aches (very common) |
| 🤢 GI upset | Nausea, vomiting |
| 🌡️ Photosensitivity | Skin burns easily in sunlight |
Drug Interactions
| Drug | Result |
|---|---|
| Allopurinol | Reduced effect (PZA blocks uric acid excretion) |
| Other hepatotoxic drugs | Additive liver damage |
| Probenecid | Reduced effect |
Nursing Implications
- ✅ Monitor uric acid levels and LFTs regularly
- ✅ Advise patient to report joint pain (gout-like symptoms)
- ✅ Adequate hydration - drink plenty of water (helps uric acid excretion)
- ✅ Avoid sunlight/use sunscreen (photosensitivity)
- ✅ Monitor for jaundice (most hepatotoxic first-line drug)
- ✅ Used only in intensive phase (first 2 months) - not continued phase
🔵 Drug 4 - ETHAMBUTOL (E / EMB)
Classification
- Synthetic bacteriostatic drug (slows bacteria, doesn't kill - at standard doses)
- Protects against development of rifampicin resistance
Mechanism (simple)
Breaks down the bacteria's cell wall scaffold
- Inhibits arabinosyl transferase (embB gene)
- Blocks synthesis of arabinogalactan (a key cell wall component)
- Without cell wall → bacteria become vulnerable
Common Adverse Effects
| Effect | What Patient Feels |
|---|---|
| 👁️ Optic neuritis | Blurred vision, loss of red-green color vision (MOST IMPORTANT - dose-dependent) |
| 🤢 GI upset | Nausea, stomach pain |
| 🦴 Hyperuricemia | Joint pain (mild, less than PZA) |
| 🌡️ Peripheral neuropathy | Rare |
🚨 Optic neuritis is the KEY adverse effect of Ethambutol - test red-green color vision before starting!
Drug Interactions
| Drug | Result |
|---|---|
| Antacids (aluminium hydroxide) | Reduces ethambutol absorption |
| Other nephrotoxic drugs | Increased renal toxicity risk (EMB excreted by kidneys) |
Nursing Implications
- ✅ Baseline visual acuity test + red-green color vision test before starting
- ✅ Ask about vision changes at every visit - blurred vision, difficulty distinguishing red from green
- ✅ If patient reports any visual changes → STOP DRUG IMMEDIATELY and refer ophthalmology
- ✅ Avoid in children <5 years (cannot report visual symptoms reliably)
- ✅ Reduce dose in renal failure (drug accumulates → more eye toxicity)
- ✅ Do NOT give with antacids at the same time
⚡ QUICK COMPARISON TABLE (Most Important for Exam)
| Drug | Nickname | Kills or Slows? | #1 Side Effect | Antidote / Prevention |
|---|---|---|---|---|
| Rifampicin | R | Kills | Orange urine + Liver toxicity | Monitor LFTs |
| Isoniazid | H | Kills | Peripheral neuropathy | Pyridoxine (B6) |
| Pyrazinamide | Z | Kills (in macrophages) | Hepatotoxicity + Gout | Monitor uric acid |
| Ethambutol | E | Slows | Optic neuritis (eye) | Baseline eye test |
🎯 HEPATOTOXICITY - All 3 Can Cause It!
Rifampicin + Isoniazid + Pyrazinamide ALL cause liver damage
- ALT/AST > 3x normal WITH symptoms (nausea, jaundice, abdominal pain)
- ALT/AST > 5x normal even WITHOUT symptoms
- Yellow eyes/skin (jaundice)
- Dark urine (like tea)
- Pale/clay-coloured stools
- Right upper abdomen pain
🧠 NURSING IMPLICATIONS - COMMON TO ALL DRUGS
- DOT (Directly Observed Therapy) - watch patient swallow every dose
- Never miss a dose - skipping doses causes drug resistance
- Take medicines at the same time daily
- Monitor LFTs, CBC, renal function regularly
- Report side effects immediately - especially vision, numbness, yellow eyes
- HIV test for all TB patients
- Complete the full course even if feeling better
- Sputum tests at 2 months, 5 months, end of treatment
🔑 Classic Exam MCQ Clues
| If exam says... | Think... |
|---|---|
| "Tingling in hands and feet" with TB treatment | INH → Peripheral neuropathy → give B6 |
| "Red-green color blindness" with TB treatment | Ethambutol → Optic neuritis → STOP drug |
| "Orange urine" with TB treatment | Rifampicin → Normal, reassure patient |
| "Gout/joint pain" with TB treatment | Pyrazinamide → Hyperuricemia |
| "OCP failure" with TB treatment | Rifampicin → CYP450 inducer |
| "Phenytoin toxicity" with TB treatment | INH → inhibits phenytoin metabolism |
| "Avoid in pregnancy" (one drug) | Streptomycin (causes fetal deafness - but this is 2nd line) |
- Lippincott Illustrated Reviews: Pharmacology, Ch. 32
- Murray & Nadel's Textbook of Respiratory Medicine, p. 2106-2122
Search for recent MDR-TB treatment guidelines 2024-2025
"multidrug-resistant tuberculosis"[MeSH Terms] AND "treatment"[MeSH Terms]
WHO MDR-TB treatment guidelines 2024 2025 BPaLM bedaquiline pretomanid
"MDR-TB" AND "BPaLM" AND "treatment"
https://www.who.int/teams/global-programme-on-tuberculosis-a…
PMID: 40657634
PMID: 40953688
WHO Module 4 TB treatment 2025 update MDR XDR BPaLM BDLLfxC new regimen
🆕 MDR-TB Treatment Guidelines - 2024-2025 Update
🔑 The Big Picture - What Changed?
Old approach: Long 18-24 month regimens with painful injectable drugs (kanamycin, amikacin) New approach: Short 6-month all-oral regimens - simpler, safer, more effective
📋 Three Categories of MDR-TB Regimens (WHO 2025)
🥇 TIER 1 - PREFERRED: 6-Month All-Oral Regimens
🟢 Regimen 1: BPaLM
| Drug | Full Name | Role |
|---|---|---|
| B | Bedaquiline | Inhibits ATP synthase (bacterial energy) |
| Pa | Pretomanid | Disrupts cell wall + kills anaerobic bacteria |
| L | Linezolid | Inhibits protein synthesis (50S ribosome) |
| M | Moxifloxacin | Inhibits DNA gyrase (fluoroquinolone) |
- Who gets BPaLM: MDR-TB/RR-TB patients sensitive to fluoroquinolones
- Duration: 6 months
- Moxifloxacin dropped if fluoroquinolone-resistant → becomes just BPaL (also 6-9 months)
- Success rate: ~76% (TB-PRACTECAL trial, Lancet 2024) vs 51% with old injectable regimen
- Bedaquiline: 400 mg daily x 2 weeks → 200 mg 3x/week x 24 weeks
- Pretomanid: 200 mg daily x 26 weeks
- Linezolid: 600 mg daily x 26 weeks (600 mg better tolerated than 1200 mg - ZeNix trial)
🟡 Regimen 2: BDLLfxC
| Drug | Full Name |
|---|---|
| B | Bedaquiline |
| D | Delamanid (replaces Pretomanid) |
| L | Linezolid |
| Lfx | Levofloxacin |
| C | Clofazimine |
- Key advantage: Suitable for groups excluded from BPaLM:
- ✅ Children of any age
- ✅ Adolescents
- ✅ Pregnant women
- ✅ Breastfeeding women
- Duration: 6 months
- Delamanid replaces pretomanid (better safety profile in these populations)
🥈 TIER 2: 9-Month All-Oral Regimen
- For MDR-TB without fluoroquinolone resistance
- All-oral, shorter than old regimens
- Still widely used - 99 countries using it by end of 2024
- Includes: bedaquiline, fluoroquinolone, ethionamide/prothionamide, ethambutol, pyrazinamide, clofazimine
🥉 TIER 3 - LAST RESORT: 18-20 Month Regimens
- Only when shorter regimens fail or are not feasible
- May include amikacin (injectable) as a last option
- Still used in 54% of MDR-TB patients globally in 2024 (due to limited access to new drugs)
📊 Global Uptake (WHO 2025 Report)
| Year | Patients on 6-month regimens | Countries using it |
|---|---|---|
| 2022 | 1,744 | 41 |
| 2023 | 5,653 | 60 |
| 2024 | 34,256 | 97 |
- A 6x increase in one year - the fastest scale-up in TB history
- By 2024, African Region (45%) and Eastern Mediterranean (57%) had highest 6-month regimen use
⚠️ Where 6-Month Regimens Are NOT Recommended (2025)
Both BPaLM and BDLLfxC have limitations in certain complex TB forms:
| Situation | Issue |
|---|---|
| TB Meningitis (TBM) | Poor CNS drug penetration - neither BPaLM nor BDLLfxC recommended |
| Bone/Osteoarticular TB | Insufficient drug levels at bone |
| Disseminated/Miliary TB | Limited clinical experience |
| Children <14 years | Longer regimens still recommended (BDLLfxC is an option for MDR-TB in children) |
| HIV with CD4 <100 | Use with caution, requires specialist input |
💊 New Drug Side Effects to Know
| Drug | Key Side Effect | Monitor |
|---|---|---|
| Bedaquiline | QTc prolongation (heart rhythm) | ECG at baseline + regularly |
| Linezolid | Peripheral neuropathy, thrombocytopenia, anaemia | CBC, neuropathy symptoms |
| Pretomanid | Peripheral neuropathy, hepatotoxicity, QTc | LFTs, ECG |
| Moxifloxacin | QTc prolongation | ECG (additive with Bedaquiline!) |
| Clofazimine | Skin discolouration (pink to brown-black), GI upset | Warn patient - harmless |
| Delamanid | QTc prolongation | ECG |
🚨 QTc prolongation is the most critical monitoring concern in BPaLM - multiple drugs in the regimen all prolong QTc (bedaquiline + moxifloxacin + clofazimine). ECG monitoring is mandatory.
🆕 What's New in Drug-Susceptible TB (2025)
- Isoniazid (H) + Rifapentine (P) + Moxifloxacin (M) + Pyrazinamide (Z) x 2 months
- Then: Isoniazid + Rifapentine + Moxifloxacin x 2 months
- Rifapentine dose: 1200 mg, Moxifloxacin: 400 mg - daily dosing
- NOT recommended yet for extrapulmonary TB, children <12 years, HIV with CD4 <100, or pregnancy
🆕 WHO 2025 New Guidelines on TB & Undernutrition
- Released October 2025 as Module 6 of consolidated TB guidelines
- Addresses undernutrition as a major driver of TB epidemic
- Recommends integrating nutritional support and food assistance into TB care
🧠 Exam Summary Table
| Regimen | Duration | For Who | Key Drugs |
|---|---|---|---|
| BPaLM | 6 months | MDR-TB, FQ-sensitive | Bedaquiline + Pretomanid + Linezolid + Moxifloxacin |
| BPaL | 6-9 months | XDR-TB, FQ-resistant | Bedaquiline + Pretomanid + Linezolid |
| BDLLfxC | 6 months | Children, pregnant, breastfeeding | Bedaquiline + Delamanid + Linezolid + Levofloxacin + Clofazimine |
| 9-month regimen | 9 months | MDR, no FQ resistance | All-oral, older second-line drugs |
| 18-20 month | Long | Last resort only | May include injectable (amikacin) |
| 2HPMZ/2HPM | 4 months | Drug-susceptible TB (new) | H + Rifapentine + Moxifloxacin + Z |
📌 Key Facts for Exam MCQs
- MDR-TB = resistant to Rifampicin + Isoniazid
- Pre-XDR-TB = MDR + resistant to any fluoroquinolone
- XDR-TB = MDR + fluoroquinolone + bedaquiline OR linezolid resistant
- BPaLM = first-line preferred 6-month regimen since WHO 2022
- BDLLfxC = second 6-month option added in 2024, safe in children/pregnancy
- Linezolid 600 mg (not 1200 mg) - current recommendation (ZeNix trial)
- ECG monitoring mandatory with BPaLM (QTc)
- Clofazimine causes harmless skin discolouration (pink-brown)
- Only 2 in 5 MDR-TB patients accessed treatment globally in 2024 (treatment gap remains huge)
- DOT remains mandatory for all MDR-TB regimens
- Davoli et al., 2025 - 6-month MDR-TB regimens review (PMID: 40953688)
- Michalik et al., 2025 - DR-TB treatment advances (PMID: 40657634)
- WHO Global TB Report 2025
Make a quick reference card on TBM treatment in 2025
"tuberculous meningitis" AND "treatment" AND "dexamethasone"
tuberculous meningitis TBM treatment guidelines 2024 2025 WHO regimen dexamethasone
PMID: 41540106
A clean, professional medical quick reference card titled "Tuberculous Meningitis (TBM) Treatment 2025" with the following sections clearly laid out on a white background with colored section headers: SECTION 1 - "ANTI-TB REGIMEN" (blue header): - WHO 2025: 2HRZE / 10HR = 12 months total - Intensive phase (2 months): Isoniazid 5mg/kg/day (max 300mg) + Rifampicin 10mg/kg/day (max 600mg) + Pyrazinamide (weight-based) + Ethambutol (weight-based) - Continuation phase (10 months): Isoniazid + Rifampicin - ⚠ Children: Same 12-month regimen SECTION 2 - "ADJUNCTIVE DEXAMETHASONE" (red header): - ALWAYS add dexamethasone (reduces mortality and disability) - Standard: 0.3-0.4 mg/kg/day IV, taper over 6-8 weeks - NEW 2026 (Nat Med RCT): Dexamethasone benefit confirmed for LTA4H TT genotype; CC/CT genotype benefit uncertain - ⚠ Do NOT omit steroids - still standard of care pending further data SECTION 3 - "CSF FINDINGS" (green header): - Lymphocytic pleocytosis 10-500 cells/uL - Protein >1 g/L (high) - Glucose low (<2.2 mmol/L or CSF:plasma ratio <50%) - Opening pressure raised - ADA elevated SECTION 4 - "COMPLICATIONS TO MONITOR" (orange header): - Hydrocephalus → VP shunt if needed - Cranial nerve palsies (CN III, IV, VI, VII) - Cerebral infarction - SIADH (hyponatremia) - Raised ICP SECTION 5 - "KEY POINTS" (purple header, small yellow boxes): - ⚠ BPaLM / BDLLfxC NOT recommended for TBM (poor CNS penetration) - Rifampicin has good CSF penetration - Isoniazid has excellent CSF penetration - Start treatment IMMEDIATELY on clinical suspicion - don't wait for culture - 12-month regimen for TBM (not 6-month standard) Include a small "GRADE" scale showing evidence level. Use a clean clinical card layout with colored boxes, medical font, and organized grid layout. Make it suitable for printing as a pocket reference card.
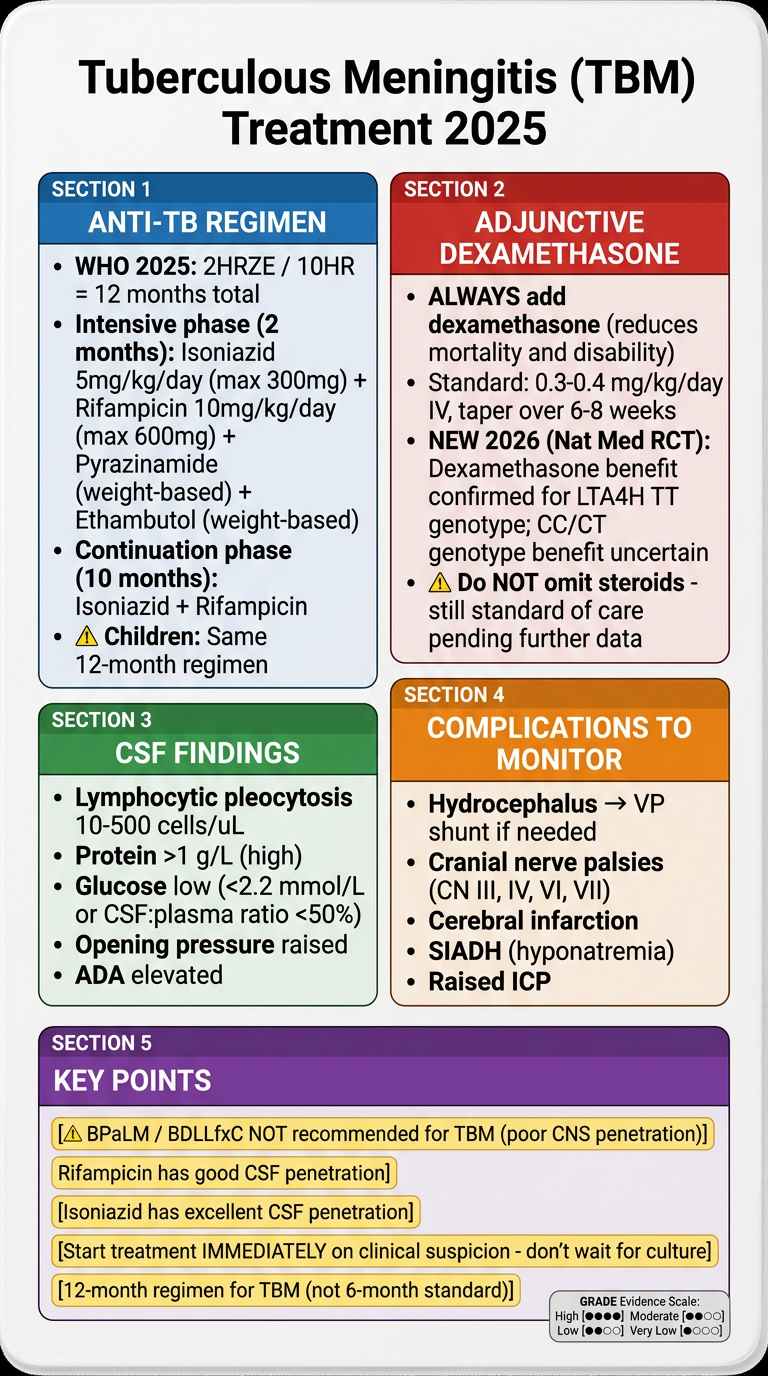
🧠 TBM Treatment 2025 - Quick Reference
💊 Anti-TB Regimen (WHO 2025)
| Phase | Duration | Drugs | Doses |
|---|---|---|---|
| Intensive | 2 months | H + R + Z + E | H: 5 mg/kg/day (max 300 mg); R: 10 mg/kg/day (max 600 mg); Z + E: weight-based |
| Continuation | 10 months | H + R | Same doses |
Children: Same 12-month regimen, weight-adjusted doses ⚠️ BPaLM and BDLLfxC are NOT recommended for TBM - poor CNS drug penetration
🔴 Adjunctive Dexamethasone (Always Add)
- Dose: 0.3-0.4 mg/kg/day IV → taper over 6-8 weeks
- Reduces mortality and neurological disability
- 🆕 2026 Landmark RCT (Donovan et al., Nature Medicine): Dexamethasone benefit is genotype-dependent (LTA4H gene):
- TT genotype → clear survival benefit from dexamethasone
- CC/CT genotype → benefit uncertain (trial did not establish noninferiority of placebo)
- Clinical implication: Dexamethasone remains standard of care for ALL patients until genotyping becomes routine - do NOT omit
🧪 CSF Findings in TBM
| Parameter | Finding |
|---|---|
| Appearance | Clear / straw-coloured |
| Cells | 10-500/μL, lymphocytic |
| Protein | >1 g/L (elevated) |
| Glucose | <2.2 mmol/L or CSF:plasma <50% |
| Opening pressure | Raised |
| ADA | Elevated (>10 U/L in CSF) |
| NAAT (Xpert Ultra) | Sensitivity ~70%, specificity 98% |
⚠️ Complications to Monitor
- Hydrocephalus - most common; needs VP shunt if severe
- Cranial nerve palsies - CN III, IV, VI (eye movement), VII (facial)
- Cerebral infarction - vasculitis of basal vessels
- SIADH - hyponatremia, fluid restriction needed
- Raised ICP - manage with head elevation, mannitol if severe
🔑 5 Must-Know Points
- Start treatment immediately on clinical suspicion - never wait for culture (takes weeks)
- 12 months, not 6 - TBM needs longer treatment than pulmonary TB
- Rifampicin + Isoniazid have the best CSF penetration of first-line drugs
- Dexamethasone is mandatory - reduces death and disability (still standard of care 2025)
- BPaLM/BDLLfxC = NOT for TBM - new short MDR regimens do not reach the CNS adequately
- Donovan et al., Nature Medicine 2026 - landmark Phase 3 RCT on dexamethasone genotyping (PMID: 41540106)
- Rosen's Emergency Medicine, p. 4418
- WHO Consolidated Guidelines Module 4: Treatment and Care, 2025
Build simple chart of all First line drugs
A clean, professional medical reference chart titled "First-Line Anti-TB Drugs - Quick Reference" on a white background. The chart is a wide comparison table with 5 columns, one for each drug. Each drug column has a distinct color header: Column 1 - RIFAMPICIN (R) - RED header Column 2 - ISONIAZID (H) - BLUE header Column 3 - PYRAZINAMIDE (Z) - GREEN header Column 4 - ETHAMBUTOL (E) - ORANGE header Column 5 - STREPTOMYCIN (S) - PURPLE header Each column contains these rows: Row 1 - DRUG CLASS: R: Rifamycin antibiotic H: Isonicotinic acid hydrazide Z: Nicotinamide analogue E: Synthetic bacteriostatic S: Aminoglycoside antibiotic Row 2 - ACTION (Kills or Slows?): R: BACTERICIDAL (kills) H: BACTERICIDAL (kills) Z: BACTERICIDAL (acidic env.) E: BACTERIOSTATIC (slows) S: BACTERICIDAL (kills) Row 3 - MECHANISM: R: Inhibits RNA polymerase (rpoB) H: Inhibits mycolic acid synthesis (InhA/KatG) Z: Disrupts membrane energy; active in acidic pH E: Inhibits arabinogalactan synthesis (embB) S: Inhibits 30S ribosome protein synthesis Row 4 - DOSE (Adult): R: 10 mg/kg/day (max 600 mg) H: 5 mg/kg/day (max 300 mg) Z: 25 mg/kg/day (weight-based) E: 15-25 mg/kg/day (weight-based) S: 15 mg/kg/day IM (max 1g) Row 5 - #1 SIDE EFFECT (bold, colored): R: Orange-red urine/secretions + Hepatotoxicity H: Peripheral neuropathy (B6 deficiency) Z: Hepatotoxicity (most hepatotoxic) + Gout/Hyperuricemia E: OPTIC NEURITIS - red/green color blindness S: Ototoxicity (VIII nerve deafness) + Nephrotoxicity Row 6 - ANTIDOTE / PREVENTION: R: Monitor LFTs; warn about orange urine H: Give Pyridoxine (Vitamin B6) 25-50 mg/day Z: Monitor uric acid; hydration E: Baseline eye test; stop if vision changes S: Avoid in pregnancy; monitor renal function Row 7 - KEY DRUG INTERACTION: R: CYP450 INDUCER - reduces OCP, warfarin, ARVs, steroids H: Increases phenytoin toxicity; avoid alcohol Z: Blocks uric acid excretion (antagonizes allopurinol) E: Antacids reduce absorption (give 1hr apart) S: Additive nephrotoxicity with aminoglycosides Row 8 - AVOID IN: R: Severe liver disease H: Liver disease; monitor in alcoholics Z: Severe liver disease; gout E: Children under 5 yrs; renal failure (reduce dose) S: PREGNANCY (fetal deafness); renal failure Row 9 - PHASE USED: R: Both phases (I + C) H: Both phases (I + C) Z: Intensive phase only (2 months) E: Intensive phase (protective role) S: Intensive phase (2nd line replacement) At the bottom, add a colored note box: "MEMORY: R-I-P-E = Rifampicin + Isoniazid + Pyrazinamide + Ethambutol | All 3 (R, H, Z) can cause HEPATOTOXICITY - Stop if ALT >3x ULN with symptoms or >5x ULN without symptoms" Use clean grid lines, small readable font, colored row labels on the left. Make it look like a professional hospital drug reference chart suitable for printing on A4 paper.
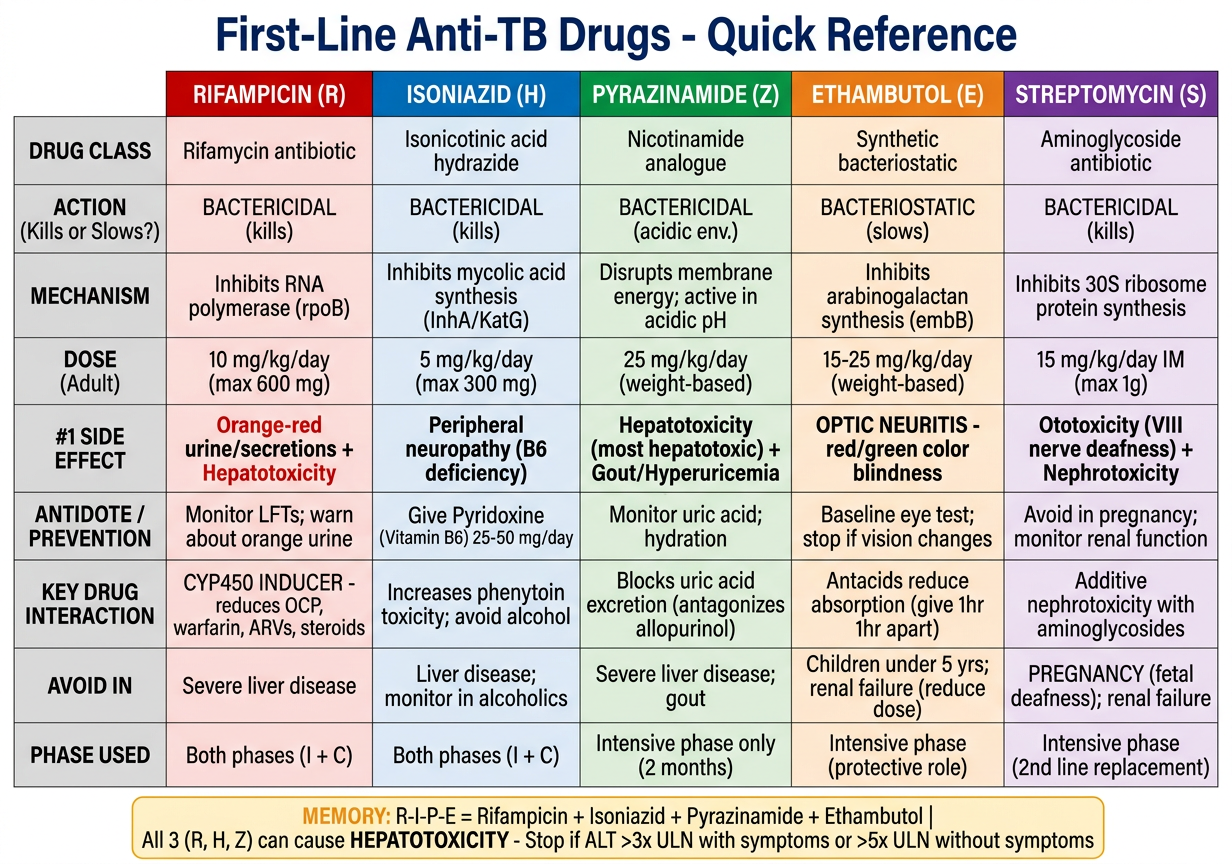
| 🔴 RIFAMPICIN (R) | 🔵 ISONIAZID (H) | 🟢 PYRAZINAMIDE (Z) | 🟠 ETHAMBUTOL (E) | 🟣 STREPTOMYCIN (S) | |
|---|---|---|---|---|---|
| Class | Rifamycin antibiotic | Isonicotinic acid hydrazide | Nicotinamide analogue | Synthetic agent | Aminoglycoside |
| Action | Bactericidal | Bactericidal | Bactericidal (acidic) | Bacteriostatic | Bactericidal |
| Mechanism | Inhibits RNA polymerase (rpoB) | Inhibits mycolic acid synthesis (InhA/KatG) | Disrupts membrane energy at acidic pH | Inhibits arabinogalactan (embB) | Inhibits 30S ribosome |
| Adult Dose | 10 mg/kg/day (max 600 mg) | 5 mg/kg/day (max 300 mg) | 25 mg/kg/day (weight-based) | 15-25 mg/kg/day | 15 mg/kg/day IM (max 1g) |
| #1 Side Effect | 🟠 Orange urine + Hepatotoxicity | 🦶 Peripheral neuropathy | 🫁 Hepatotoxicity + 🦴 Gout | 👁️ Optic neuritis | 👂 Ototoxicity + Nephrotoxicity |
| Prevention | Warn about orange urine; monitor LFTs | Give Pyridoxine (B6) 25-50 mg/day | Monitor uric acid; hydrate well | Baseline eye test; stop if vision changes | Avoid in pregnancy; monitor renal function |
| Drug Interaction | CYP450 inducer - reduces OCP, warfarin, ARVs | Increases phenytoin toxicity; avoid alcohol | Antagonizes allopurinol | Antacids reduce absorption | Additive nephrotoxicity with other nephrotoxics |
| Avoid in | Severe liver disease | Liver disease; alcoholics (caution) | Severe liver disease; gout | Children <5 yrs; renal failure | Pregnancy (fetal deafness); renal failure |
| Phase used | Both (Intensive + Continuation) | Both (Intensive + Continuation) | Intensive phase only (2 months) | Intensive phase | Intensive phase (2nd line substitute) |
🧠 Bottom-Line Memory Points
| Clue in Exam | Drug |
|---|---|
| Orange urine | Rifampicin - reassure, it's harmless |
| Tingling hands & feet | Isoniazid - give Vitamin B6 |
| Joint pain / gout | Pyrazinamide - check uric acid |
| Blurred vision / can't see red | Ethambutol - stop immediately |
| Deaf after treatment / pregnancy | Streptomycin - most dangerous in pregnancy |
| OCP failure | Rifampicin - CYP450 inducer |
| Phenytoin toxicity | Isoniazid - inhibits phenytoin metabolism |
⚠️ Hepatotoxicity Alert: Rifampicin + Isoniazid + Pyrazinamide ALL three can damage the liver. Check LFTs before starting and regularly during treatment. Stop ALL drugs if ALT >3x ULN with symptoms, or >5x ULN even without symptoms.