COPD X-ray
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the information and images needed for a comprehensive answer. Let me compile the full response.
COPD on Chest X-Ray
The chest X-ray (CXR) is NOT required to diagnose COPD - that requires spirometry (FEV₁/FVC < 0.7). However, CXR findings are important for assessing disease severity, detecting complications, and ruling out differentials like pneumonia, heart failure, or malignancy.
Key Radiographic Features
1. Hyperinflation (Most Reliable Sign)
The classic radiographic appearance of hyperinflation includes:
- Increased radiolucency of the lung fields
- Low, flat diaphragms - right hemidiaphragm at or below the anterior aspect of the 7th rib; this is probably the most reliable sign of severe emphysema
- Exaggerated verticality of the heart (small, narrow, vertical-appearing heart on PA view)
- Increased AP diameter of the chest ("barrel chest")
- Widened retrosternal lucent space >2 cm on lateral view
- Widening of the sternodiaphragmatic angle
2. Emphysema-Predominant Pattern
- Paucity of parenchymal markings (vascular attenuation / oligaemia)
- Bullae - avascular transradiant areas with thin curvilinear walls, especially upper lobes
- Upper lobe hyperlucency in centriacinar (smoking-related) emphysema
- Lower lobe predominant lucency in panacinar emphysema (e.g., alpha-1 antitrypsin deficiency)
3. Chronic Bronchitis-Predominant Pattern ("Dirty Chest")
- Increased bronchovascular markings throughout the central lung fields
- Bronchial wall thickening producing tubular shadows (end-on = ring shadows, en face = parallel line/"tram-track" shadows)
- "Dirty chest" appearance - loss of clarity of lung vessels due to increased linear markings
- Hyperaeration is usually minimal in pure chronic bronchitis
4. Complications to Look For
| Finding | Significance |
|---|---|
| Enlarged central pulmonary arteries | Pulmonary hypertension |
| Enlarged right heart silhouette | Cor pulmonale |
| New infiltrate/consolidation | Pneumonia (common COPD exacerbation trigger) |
| Avascular hyperlucent area | Pneumothorax (esp. if bullae present) |
| Air-fluid level in a bulla | Infected or haemorrhagic bulla |
| Sabre-sheath trachea | Coronal narrowing of the intrathoracic trachea, associated with COPD |
Radiographic Images
Figure 1 - Chronic Bronchitis-Predominant COPD (PA detail view)

Dense, mottled bronchovascular markings particularly prominent in the central lung fields. Hyperaeration is minimal. This pattern is typical of COPD with predominant chronic bronchitis. - Fishman's Pulmonary Diseases and Disorders
Figure 2 - Severe Emphysema-Predominant COPD (PA view)
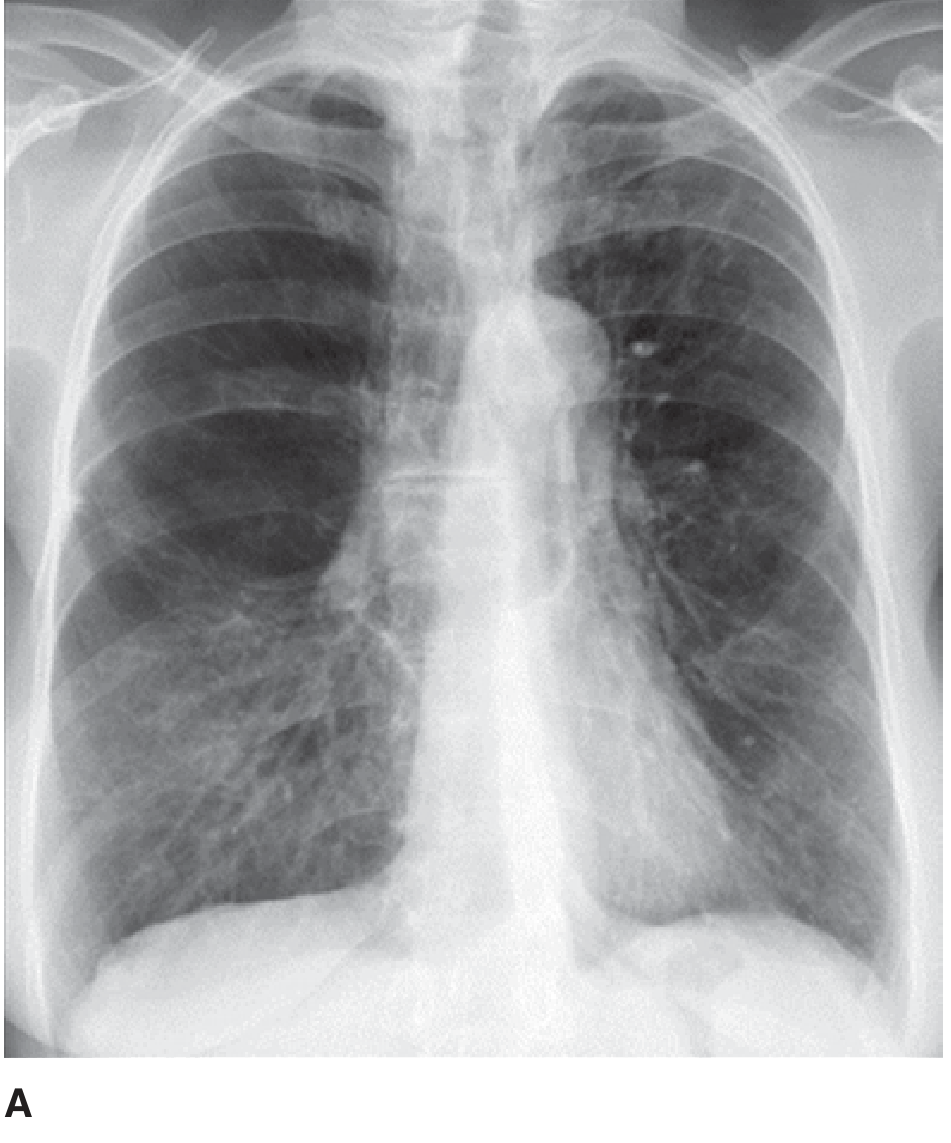
PA radiograph showing overinflated, hyperlucent lung fields, flattened diaphragms, and a narrow vertical heart - classic features of advanced emphysema. - Fishman's Pulmonary Diseases and Disorders
Figure 3 - Chronic Bronchitis / Obstructive Lung Disease with Ring Shadow (PA view)
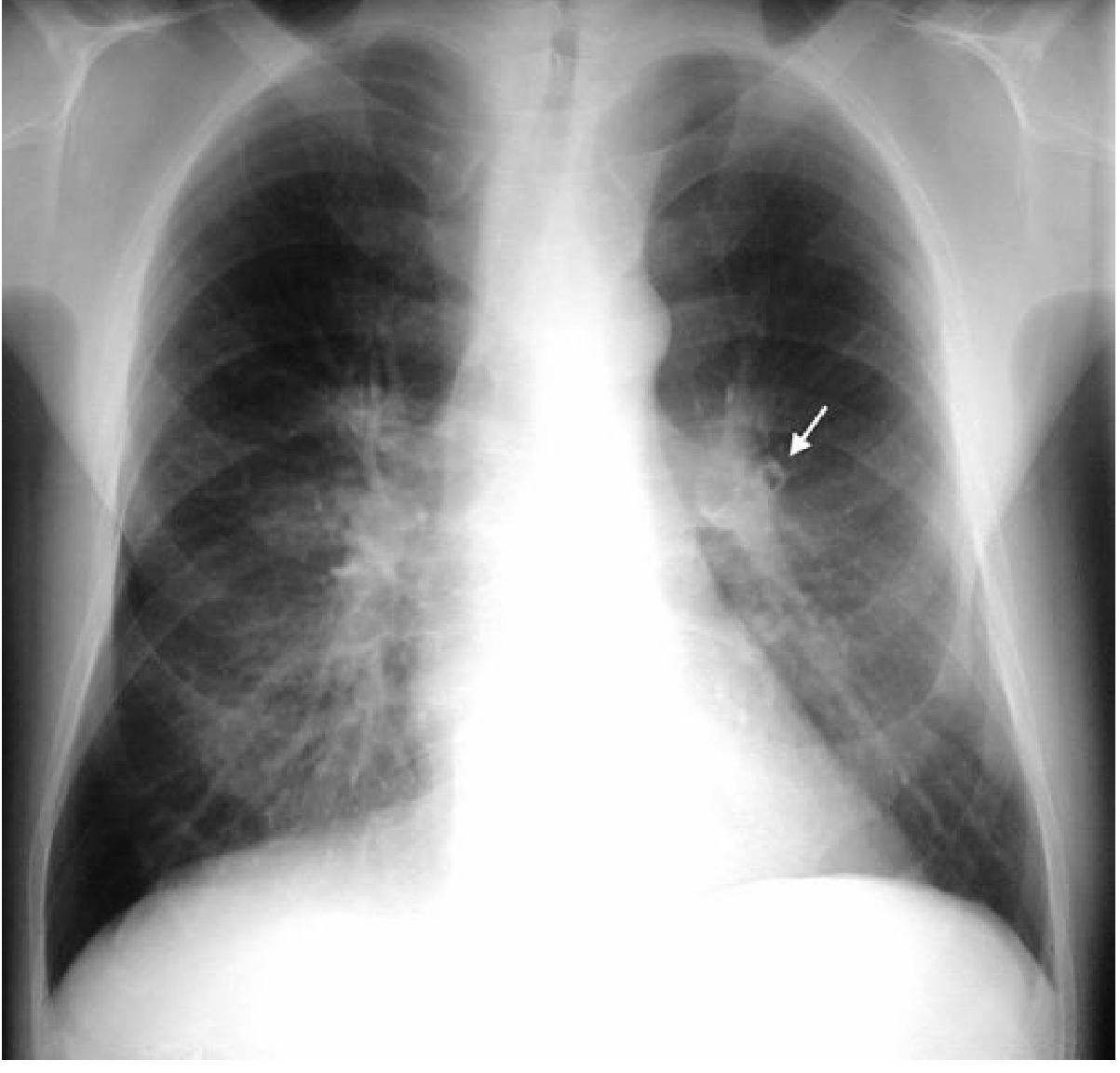
PA CXR showing mild overinflation. The arrow points to a ring shadow above the left hilum reflecting bronchial wall thickening. Accentuation of linear markings in the right lung base. - Grainger & Allison's Diagnostic Radiology
Figure 4 - Centriacinar Emphysema: PA + Lateral (Classic Teaching Case)
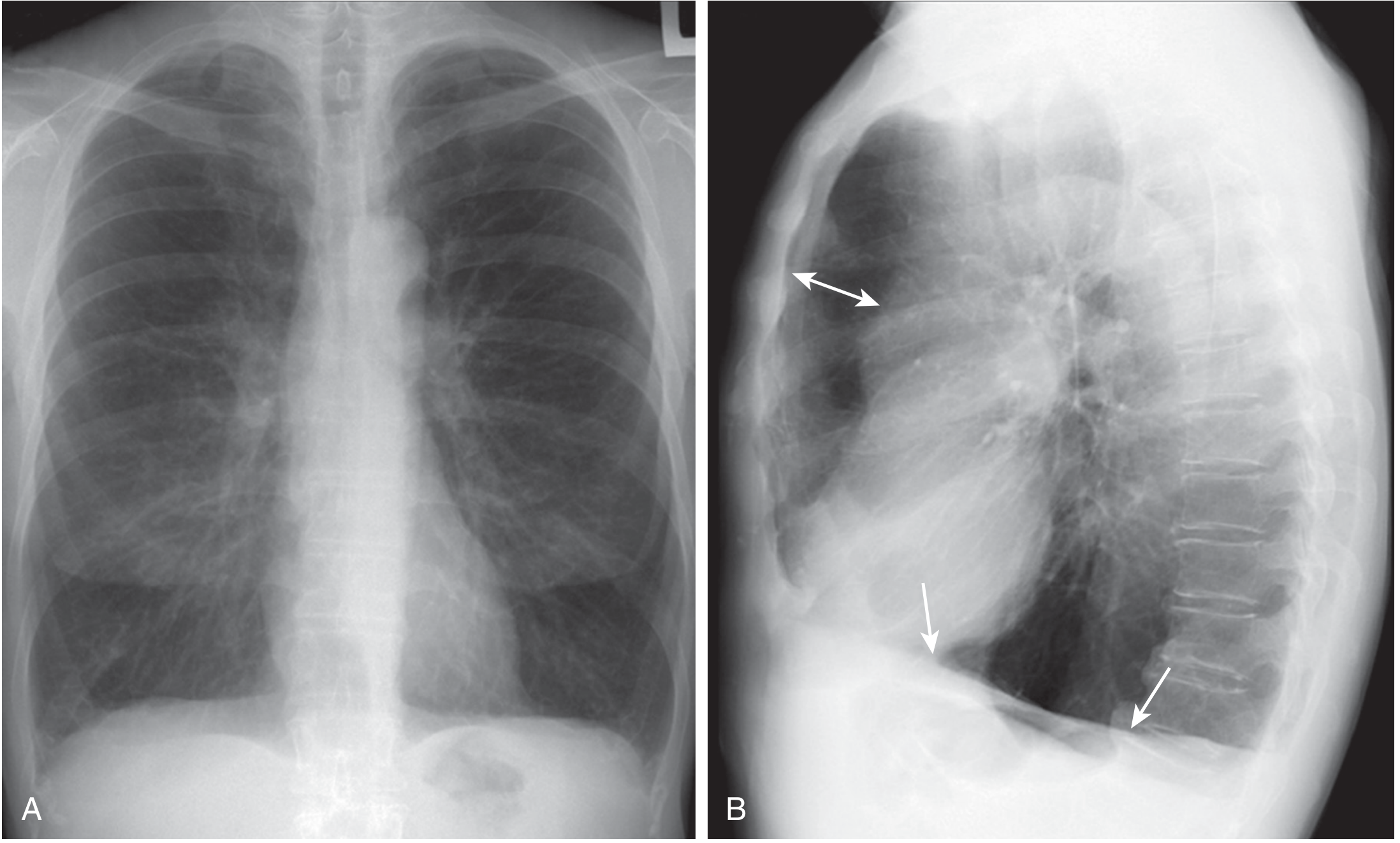
54-year-old female smoker with centriacinar emphysema. (A) PA: large lung volumes, upper lobe hyperlucency, small vertical heart. (B) Lateral: the double arrow marks the prominent retrosternal clear space; single arrows mark flattened diaphragms. These are the hallmark findings of advanced emphysema. - Murray & Nadel's Textbook of Respiratory Medicine
Specific Overinflation Criteria (Grainger & Allison)
- Height of right lung > 29.9 cm
- Right hemidiaphragm at or below the anterior aspect of the 7th rib
- Flattening of the hemidiaphragm (most reliable)
- Widening of sternodiaphragmatic angle
- Narrowing of transverse cardiac diameter
- Enlarged retrosternal space on lateral
Important Limitations
As Harrison's notes: "Chest x-ray findings may be consistent with COPD but cannot be used reliably to make the diagnosis." Early COPD is radiographically normal. CT scan (especially HRCT) is the definitive imaging modality for characterizing emphysema type and extent, detecting early bullae, and planning surgery (e.g., lung volume reduction surgery).
Sources:
- Fishman's Pulmonary Diseases and Disorders - Chapter 28 (Obstructive Lung Diseases)
- Murray & Nadel's Textbook of Respiratory Medicine - Chapter 64 (COPD Imaging)
- Grainger & Allison's Diagnostic Radiology - Chapter 6 (Radiographic Findings in COPD/Emphysema)
- Harrison's Principles of Internal Medicine, 22e - Chapter 30 (Laboratory Findings in COPD)
- Goldman-Cecil Medicine - Chapter 76 (Imaging in COPD)
This is a shared conversation. Sign in to Orris to start your own chat.