Creatine
Reading File
Searching PubMed
creatine supplementation exercise performance
Searching the Web
creatine supplementation benefits dosing safety 2024 2025
Finding Sources
Searching PubMed
creatine supplementation muscle health
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough breakdown of creatine covering biochemistry, physiology, supplementation, and the latest evidence.
Creatine: Complete Overview
1. Biochemistry & Synthesis
Creatine is a non-protein nitrogenous compound synthesized endogenously in the kidneys and liver from three amino acids:
- Arginine + Glycine → (via amidinotransferase, in kidneys) → Guanidinoacetate
- Guanidinoacetate → (via methyltransferase + S-adenosylmethionine, in liver) → Creatine
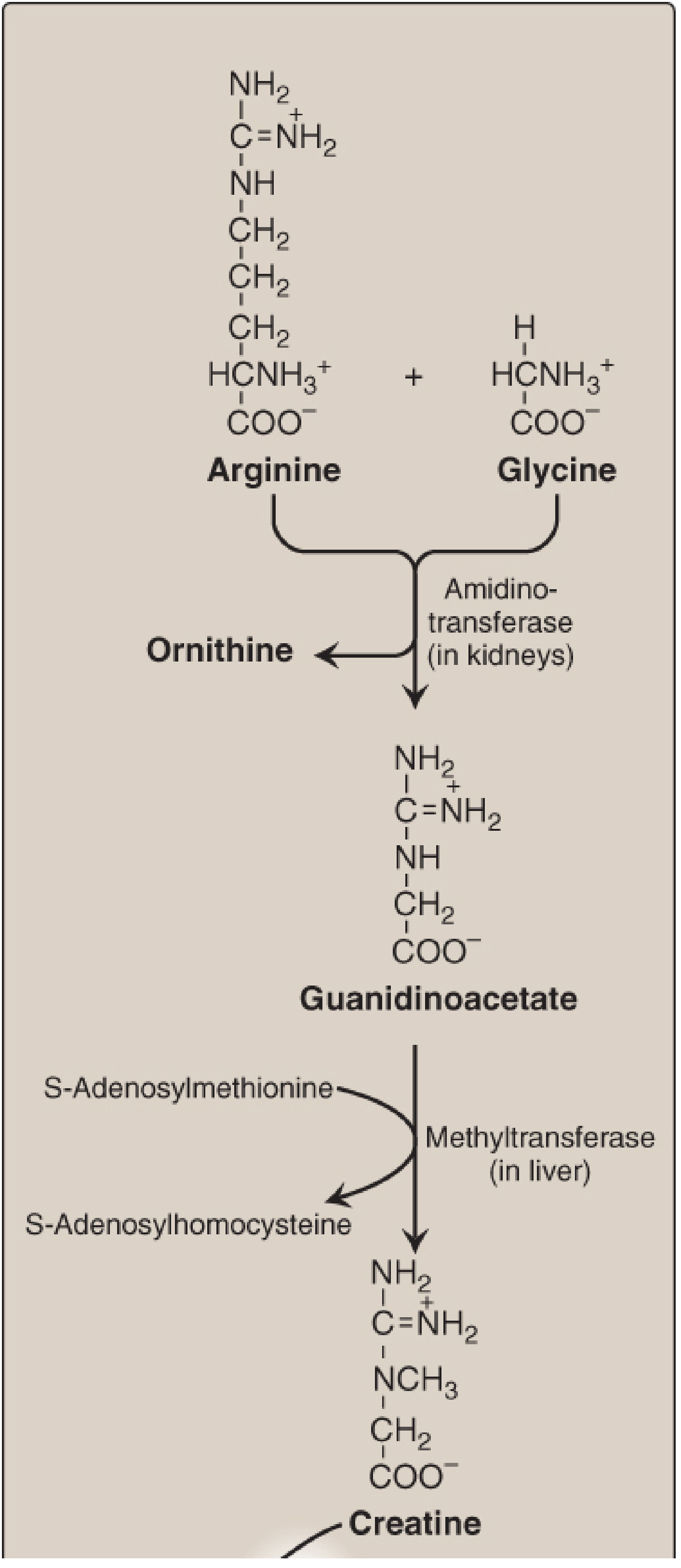
About half the body's creatine comes from endogenous synthesis; the other half from dietary sources (primarily red meat and fish).
2. How It Works - The Phosphocreatine System
Once in muscle, creatine is phosphorylated to creatine phosphate (phosphocreatine) by creatine kinase, using ATP as the donor. During intense exercise, this reaction runs in reverse - phosphocreatine rapidly donates its phosphate group to ADP to regenerate ATP:
Creatine phosphate + ADP → Creatine + ATP (catalyzed by creatine kinase)
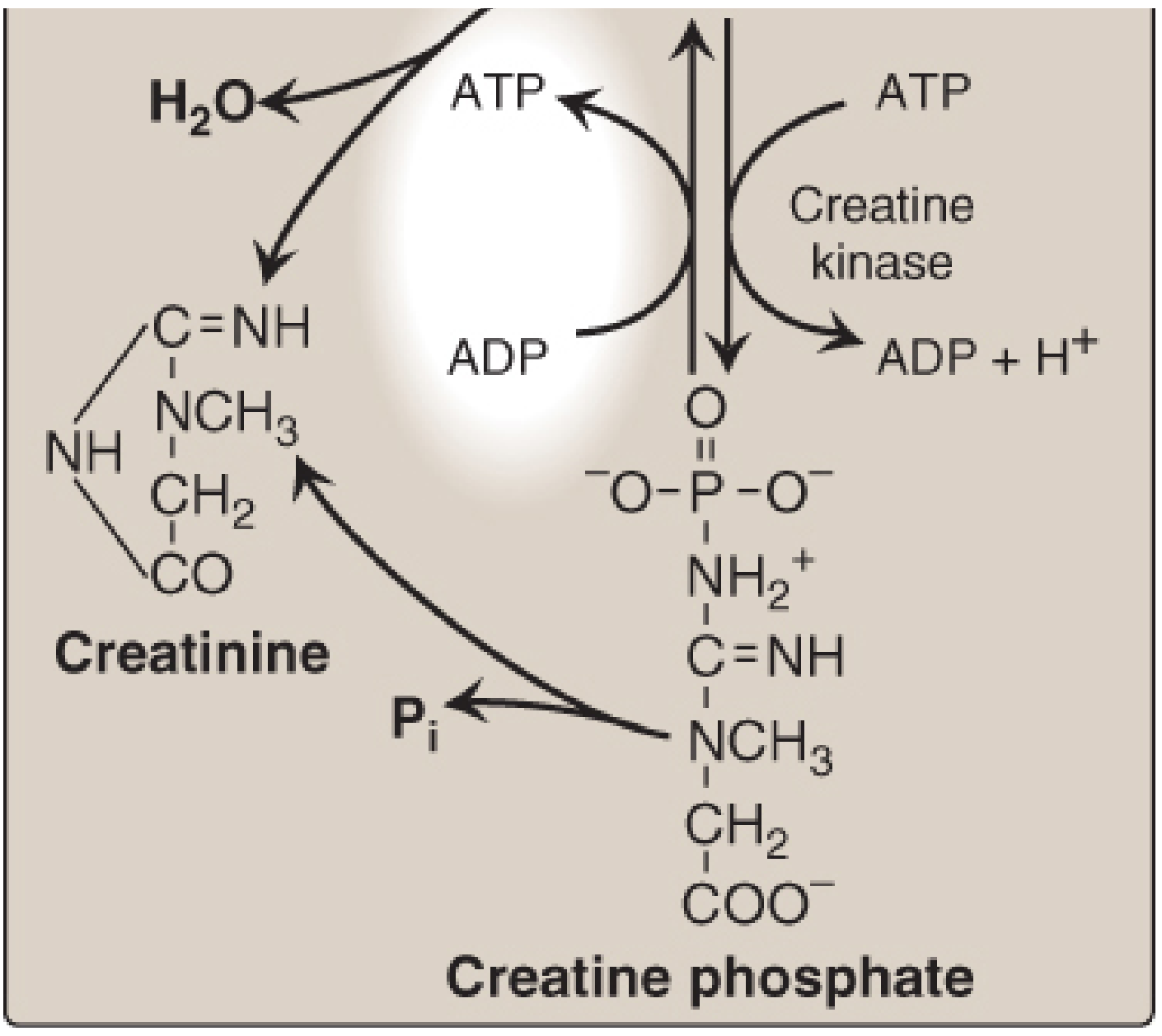
This system provides a small but instantly available reserve of high-energy phosphates during the first few seconds of explosive, high-intensity activity (sprints, heavy lifts). It bridges the gap until glycolysis and oxidative phosphorylation ramp up.
- Lippincott's Illustrated Reviews: Biochemistry, 8th ed., p. 812-813
- Harper's Illustrated Biochemistry, 32nd ed., p. 323
3. Creatinine - The Degradation Product
Creatine and creatine phosphate spontaneously and irreversibly cyclize to form creatinine, which is excreted in urine. Clinically relevant points:
- Urinary creatinine output (~1-2 g/day in adult males) is proportional to total muscle mass - used to verify complete 24-hour urine collection
- A rise in serum creatinine signals impaired renal clearance (kidney malfunction), since it is normally cleared rapidly
- Loss of muscle mass (paralysis, muscular dystrophy) → reduced urinary creatinine
4. Supplementation
Forms
Creatine monohydrate is the gold standard. It is the most studied, cheapest, and most effective form. Other marketed forms (ethyl ester, buffered, hydrochloride) show no meaningful advantage.
Dosing Protocols
| Protocol | Dose | Timeline |
|---|---|---|
| Loading (optional) | 20 g/day in 4 divided doses | 5-7 days |
| Maintenance | 3-5 g/day | Ongoing |
| Without loading | 3-5 g/day | ~4 weeks to saturate |
Loading is faster but not necessary - both achieve the same muscle saturation level by ~4 weeks. The total daily creatine pool in muscle is about 120-140 g; supplementation raises it by ~20-40%.
Performance Benefits (Evidence-Based)
- Strength and power: Increases maximal strength, peak power, and sprint performance, particularly in repeated high-intensity bouts (<30 seconds)
- Muscle hypertrophy: Augments lean mass gains when combined with resistance training - partly via increased training volume, partly via cellular hydration
- Recovery: May reduce muscle damage markers and assist post-exercise glycogen resynthesis
- Cognitive function: Emerging evidence for benefits in sleep-deprived individuals and older adults (creatine is found in brain tissue, not just muscle)
A 2024 meta-analysis (Wang et al., Nutrients) confirmed significant gains in muscle strength in adults under 50 with creatine + resistance training. A 2025 systematic review in J Diet Suppl also showed benefits in combat sport athletes. And a 2025 systematic review specifically in active females showed comparable performance-enhancing effects.
5. Safety
The 2025 JISSN analysis found side effect rates were identical between creatine and placebo groups (13.7% vs 13.2%, p = 0.776) across clinical trials - a strong indication creatine's perceived side effects are largely nocebo or unrelated.
A 2025 Frontiers in Nutrition review addressed common safety concerns:
| Concern | Evidence |
|---|---|
| Kidney damage | No adverse effects in healthy individuals |
| Cancer risk | Theoretical concern (carcinogenic heterocyclic amines from cooked meat), but no link to creatine supplementation itself |
| Dehydration / cramps | Not supported - creatine may actually reduce cramping |
| Thermoregulation | No significant impairment; may assist |
Caution: Individuals with pre-existing kidney disease should use creatine cautiously and under medical supervision. Evidence is also insufficient for pregnant women.
6. Clinical Notes
- Creatine kinase (CK) isoforms have diagnostic value: the MB isoform elevated in serum indicates myocardial damage (MI marker)
- Creatine deficiency syndromes (rare inborn errors of creatine synthesis or transport) present in children as intellectual disability, seizures, and speech delay
- Serum creatinine is a standard kidney function marker - but note that creatine supplementation can modestly raise serum creatinine (not reflecting actual kidney damage), which can confuse interpretation
Bottom line: Creatine monohydrate at 3-5 g/day is safe, effective for power/strength/hypertrophy, and supported by decades of research. The 2025 literature continues to confirm this. It is the most evidence-backed sports supplement available.
Creatine in gym how does it work and sd we take it
Searching PubMed
creatine supplementation resistance training strength
Searching the Web
creatine gym how it works should you take it 2025
Here's everything you need to know about creatine for the gym, kept practical and honest.
Creatine for the Gym
How It Works (Simple Version)
When you do a heavy set - squats, bench press, deadlifts - your muscles burn through ATP (energy) in seconds. Your body can't make new ATP fast enough to keep up.
That's where creatine comes in.
Your muscles store creatine as phosphocreatine. During those explosive, heavy moments, phosphocreatine rapidly donates a phosphate to "recharge" ADP back into ATP. Think of it as a backup power battery that kicks in instantly.
Phosphocreatine + ADP → Creatine + ATP (instant energy)
The result:
- You can push one or two more reps on a heavy set
- You recover faster between sets
- Over weeks, those extra reps add up to more muscle and strength
What It Actually Does For You in the Gym
| Benefit | What to Expect |
|---|---|
| Strength | Measurably more weight lifted over time |
| Muscle size | Lean mass gain (partly muscle, partly water in muscle cells) |
| High-intensity performance | Better sprints, explosive lifts |
| Recovery between sets | Slightly faster - you feel less fatigued |
A 2024 meta-analysis in Nutrients confirmed significant strength gains in adults under 50 combining creatine with resistance training. A 2025 meta-analysis specifically confirmed upper and lower body strength and power improvements.
Should You Take It?
Yes, if you:
- Do resistance training (weights, CrossFit, powerlifting)
- Do any explosive sport (sprinting, martial arts, football)
- Are vegetarian or vegan (you get very little dietary creatine - animal products are the main food source, so you benefit most from supplementing)
- Are over 50 (helps preserve muscle mass and emerging evidence supports cognitive benefits too)
You probably won't notice much if you:
- Only do steady-state cardio (jogging, cycling at moderate pace) - creatine helps short, explosive efforts, not endurance
- Already eat a lot of red meat and fish (your levels may already be fairly saturated)
Worth noting - a 2025 UNSW trial found no lean mass difference at 5 g/day over 12 weeks in untrained beginners. This is a minority finding vs. the large body of literature, but it highlights that creatine is not magic - it works best when paired with hard, consistent training.
How to Take It
Form: Creatine monohydrate only. Ignore "buffered", "ethyl ester", "HCl" - they cost more and have no proven edge.
Dose:
- Simple approach: 3-5 g every single day. That's it. Mix in water, a shake, juice - doesn't matter.
- Loading (optional): 20 g/day (split into 4 doses) for 5-7 days, then 3-5 g/day. Saturates your muscles faster but you end up in the same place after ~4 weeks either way.
Timing: Doesn't matter much. Post-workout has a slight edge in some studies but consistency beats perfect timing. Just take it daily.
With food or without? Fine either way. Taking it with a meal (especially carbs) may slightly improve uptake.
Cycling? No need. You don't need to cycle on and off. Take it year-round.
Side Effects / Safety
- Very safe for healthy people. Side effect rates in clinical trials are the same as placebo (about 13-14% each), meaning creatine is not actually causing them.
- Water weight: You'll gain 1-2 kg in the first week - this is water being pulled into muscle cells (intracellular hydration), not fat. It's actually a good sign.
- GI discomfort: Rare, usually from taking too much at once (common during loading). Split the dose if this happens.
- Kidney concerns: No evidence of harm in healthy people. If you have pre-existing kidney disease, check with your doctor first.
The Practical Bottom Line
Buy plain creatine monohydrate powder. Take 3-5 g daily, mixed into anything. Don't overthink timing or loading. Train hard. That's the whole protocol - backed by 30+ years of research.
It's the single most evidence-supported supplement in sports nutrition. If you're lifting weights, it's worth taking.
This is a shared conversation. Sign in to Orris to start your own chat.