Make notes of respiratory system according to md pathology using robins and ackerman book. Including sll important questions that can come from this chapter for md pathology exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Molecular and prognostic marker of lung carcinoma
Finding Sources
Finding Sources
Searching PubMed
lung carcinoma molecular markers prognostic
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Now I have everything I need. Here are comprehensive notes on molecular and prognostic markers of lung carcinoma, drawn from Robbins Basic Pathology and Murray & Nadel's Respiratory Medicine.
Molecular & Prognostic Markers of Lung Carcinoma
(Robbins Basic Pathology + Murray & Nadel's Respiratory Medicine)
1. OVERVIEW — WHY MOLECULAR MARKERS MATTER
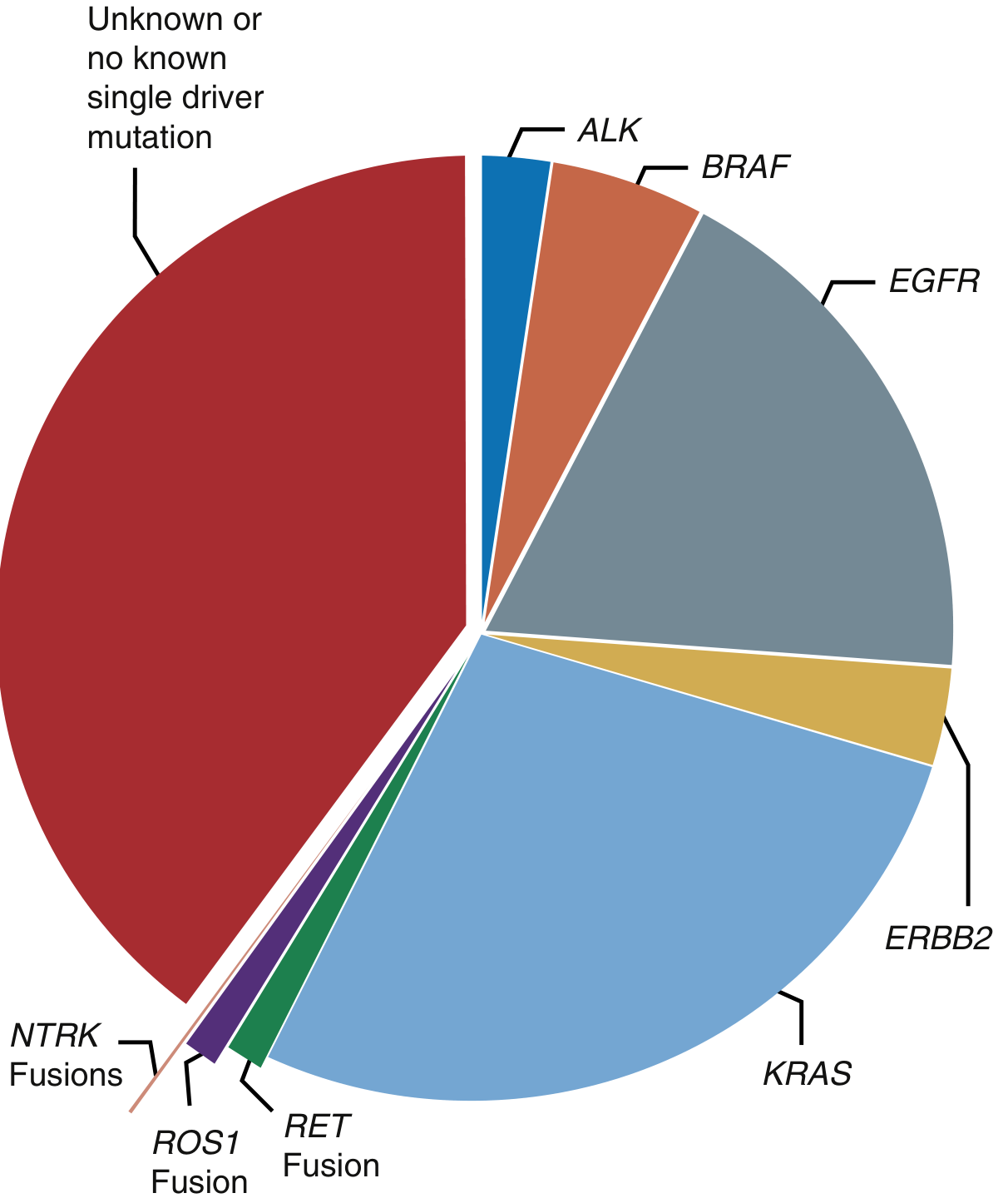
- ~50% of non-squamous NSCLC harbour a known, targetable driver mutation
- Driver mutations confer evolutionary growth/survival advantages and are clonally preserved — they define the tumor's behaviour and treatment response
- Next-generation sequencing (NGS) of every locally advanced or metastatic adenocarcinoma is now the standard of care
- Panel-based NGS is superior to single-gene testing — detects mutations, fusions, copy number alterations and RNA rearrangements in one test
- Liquid biopsy (circulating tumour DNA from blood) is used at diagnosis AND at progression to detect resistance mutations
Mutation frequency varies significantly by geographic origin, environmental exposure, and tobacco use. — Murray & Nadel's Respiratory Medicine
2. DRIVER MUTATIONS — MOLECULAR TARGETS
Proportion of NSCLC Driver Mutations (AACR GENIE data):
A. EGFR / HER2 (ERBB1/ERBB2) PATHWAY
| Feature | Details |
|---|---|
| Gene | EGFR (ERBB1) — receptor tyrosine kinase |
| Mechanism | Constitutive activation → ERK, Akt, c-SRC → cyclin D1 → uncontrolled proliferation |
| Common mutations | Exon 19 deletions (most common), L858R point mutation on exon 21 |
| Resistance mutation | T790M on exon 20 — most common cause of acquired resistance to 1st/2nd-gen TKIs |
| Frequency | 9–46% of NSCLC (highest in East Asian females, never-smokers, adenocarcinoma) |
| HER2 (ERBB2) | Mutated in ~3% NSCLC; amplification also seen in subset of adenocarcinomas |
| Targeted drugs | Osimertinib (3rd gen), Erlotinib, Gefitinib, Afatinib, Dacomitinib |
| Prognostic value | Good prognosis with targeted therapy; dramatic improvement in OS vs. EGFR-negative |
Exam point: EGFR mutations are most common in never-smoking Asian women with adenocarcinoma. Exon 19 deletion has slightly better prognosis than L858R.
B. KRAS PATHWAY
| Feature | Details |
|---|---|
| Gene | KRAS — RAS family GTPase (downstream of EGFR) |
| Frequency | ~25–30% of NSCLC (most common in smokers, Western populations) |
| Mutation type | Point mutations (G12C most actionable) |
| Prognosis | Historically poor prognosis; resistance to EGFR-TKIs |
| Targeted drug | Sotorasib (AMG 510) — first approved KRAS G12C inhibitor |
| Key fact | KRAS and EGFR mutations are mutually exclusive |
Exam point: KRAS is the most common oncogene mutated in smoking-related lung adenocarcinoma.
C. ALK / ROS1 / NTRK GENE FUSIONS
| Feature | ALK | ROS1 | NTRK |
|---|---|---|---|
| Mechanism | EML4-ALK fusion → constitutive kinase activity | ROS1 fusion (CD74-ROS1 most common) | NTRK1/2/3 fusions |
| Frequency | ~5% NSCLC | ~1–2% NSCLC | <1% NSCLC |
| Population | Young, never/light smokers, adenocarcinoma | Young, never smokers | Any histology |
| Detection | FISH, IHC, NGS | FISH, NGS | NGS, FISH |
| CNS mets | High propensity — CNS is common "sanctuary" site | Less common | Variable |
| Drugs | Alectinib (1st line), Brigatinib, Ceritinib, Lorlatinib (2nd line) | Crizotinib, Entrectinib | Larotrectinib, Entrectinib |
| Prognosis | Excellent with targeted therapy; resistance inevitable |
Exam point: ALK+ lung cancer — young, non-smoker, adenocarcinoma, signet-ring cell histology. Best response to alectinib (superior to crizotinib in 1st line).
D. BRAF MUTATIONS
| Feature | Details |
|---|---|
| Frequency | ~2–4% NSCLC |
| Key mutation | V600E (most common, ~50% of BRAF-mutated NSCLC) |
| Drugs | Dabrafenib + Trametinib (BRAF + MEK inhibitor combination) |
| Prognosis | Moderate improvement with combination targeted therapy |
E. RET FUSIONS
| Feature | Details |
|---|---|
| Frequency | ~1–2% NSCLC |
| Population | Young, never-smokers, adenocarcinoma |
| Drugs | Selpercatinib, Pralsetinib (highly selective RET inhibitors) |
F. MET (Mesenchymal-Epithelial Transition) Pathway
- MET exon 14 skipping mutations: ~3–4% NSCLC
- Drugs: Capmatinib, Tepotinib
- Also: MET amplification — common acquired resistance mechanism after EGFR-TKI therapy
3. IMMUNOTHERAPY BIOMARKERS
PD-L1 (Programmed Death-Ligand 1)
| Feature | Details |
|---|---|
| Test | IHC — Tumor Proportion Score (TPS) |
| Cutoffs | TPS ≥50% → pembrolizumab monotherapy 1st line; TPS 1–49% → combination chemo-immunotherapy |
| Relevance | Predictive (not purely prognostic) marker for checkpoint inhibitor response |
| Key caveat | PD-L1 expression is lower in oncogene-driven (EGFR/ALK) tumors → immunotherapy less effective in these patients |
TMB (Tumor Mutational Burden)
- High TMB (≥10 mutations/megabase) correlates with better response to checkpoint inhibitors
- Measured by NGS
- Independent of PD-L1 expression
Exam point: In EGFR/ALK+ adenocarcinoma, targeted therapy is always preferred over immunotherapy as 1st line.
4. TUMOR SUPPRESSOR GENES (Robbins Pathology)
| Gene | Role | Lung Cancer Relevance |
|---|---|---|
| TP53 | Cell cycle arrest, apoptosis | Mutated in >50% of all lung cancers (NSCLC + SCLC); especially squamous cell carcinoma |
| RB1 (Retinoblastoma) | G1/S checkpoint | Lost in virtually all SCLC; also lost in some NSCLC |
| CDKN2A (p16/INK4a) | Inhibits CDK4/6 → maintains RB | Deleted/inactivated in adenocarcinoma and squamous |
| STK11 (LKB1) | Serine-threonine kinase | Mutated in ~20% lung adenocarcinoma; associated with KRAS co-mutation and immunotherapy resistance |
| KEAP1/NRF2 | Oxidative stress pathway | Mutated in squamous cell carcinoma; poor prognosis |
| SMARCA4 (BRG1) | SWI/SNF chromatin remodelling | Mutated in ~10% NSCLC; aggressive behaviour |
5. MOLECULAR MARKERS BY HISTOLOGICAL SUBTYPE
Adenocarcinoma (most amenable to targeted therapy)
- EGFR, KRAS, ALK, ROS1, RET, NTRK, BRAF, MET exon 14, HER2
- Immunohistochemistry: TTF-1+, Napsin A+
- Always test for all driver mutations before starting treatment
Squamous Cell Carcinoma
- FGFR1 amplification (~20%) — investigational targets
- EGFR mutations rare (~3%)
- PIK3CA mutations (~10%)
- PDGFRA amplification
- IHC: p40+, p63+, CK5/6+, TTF-1 negative
- PD-L1 expression often higher
Small Cell Lung Cancer (SCLC)
- No known targetable driver mutations currently
- Universal RB1 loss (virtually 100%) + TP53 mutation
- MYCL1/MYCN amplification — drives proliferation
- Neuroendocrine markers: chromogranin A, synaptophysin, CD56, NSE (diagnostic, not targeted)
- DLL3 overexpression — Rovalpituzumab tesirine (investigational)
- Response to platinum-based chemotherapy initially excellent, but almost universal resistance/recurrence
- Immunotherapy (atezolizumab + chemo) now standard in extensive SCLC
Large Cell Neuroendocrine Carcinoma (LCNEC)
- Shares molecular features with SCLC (RB1/TP53) or NSCLC
- Neuroendocrine IHC positive
6. PROGNOSTIC MARKERS — OVERALL
Clinical Prognostic Factors (Robbins)
| Factor | Better Prognosis | Worse Prognosis |
|---|---|---|
| Stage | I, II | III, IV |
| Cell type | Adenocarcinoma (esp. with driver) | SCLC, large cell |
| Resectability | Resectable | Unresectable |
| Performance status | ECOG 0–1 | ECOG 3–4 |
| Weight loss | Absent | >10% body weight |
| Lymph node involvement | N0 | N2/N3 (mediastinal) |
Molecular Prognostic Markers
| Marker | Prognostic Significance |
|---|---|
| EGFR mutation | Good — excellent response to TKIs; better OS than EGFR-wt |
| ALK fusion | Good — excellent response; better OS with alectinib |
| KRAS mutation | Poor historically; improving with KRAS G12C inhibitors |
| TP53 mutation | Poor — especially in NSCLC |
| STK11/LKB1 mutation | Poor — immunotherapy resistance, rapid progression |
| SMARCA4 loss | Poor — aggressive, rapid progression |
| High TMB | Better immunotherapy response (predictive) |
| PD-L1 TPS ≥50% | Better immunotherapy response (predictive) |
| RB1 loss | Very poor — universal in SCLC |
| MYC amplification | Poor — rapid proliferation, chemotherapy resistance |
7. CONCEPTS IN MOLECULAR BIOLOGY OF LUNG CANCER (Robbins/Murray & Nadel)
Hallmarks of Cancer (Hanahan & Weinberg) applicable to lung:
Established (2000): Sustained proliferation, evasion of tumor suppressors, invasion/metastasis, replicative immortality, angiogenesis, resisting apoptosis
Added (2011): Metabolic reprogramming, genomic instability, tumor-promoting inflammation, immune evasion
Carcinogenesis Pathway
- Tobacco carcinogens (PAHs) → Phase I enzymes (CYP1A1) → active carcinogens → DNA adducts → mutations in TP53, KRAS, etc.
- Epigenetic changes → gene silencing (methylation of CDKN2A)
- Chromosomal instability → loss of heterozygosity at 3p, 9p, 17p
- Field cancerization — widespread epithelial DNA damage from carcinogen exposure → multiple independent tumours possible
Epithelial-Mesenchymal Transition (EMT)
- Key step in invasion and metastasis
- Tobacco smoke itself can induce EMT early in carcinogenesis
- Reverse (MET — Mesenchymal-Epithelial Transition) allows establishment at metastatic niche
Tumour Heterogeneity
- Major driver of treatment resistance
- Subclonal populations shift with therapy pressure → clonal selection of resistant clones
- Requires liquid biopsy at progression to detect new resistance mutations
8. RESISTANCE MECHANISMS
| Primary Mutation | Common Resistance Mechanism |
|---|---|
| EGFR exon 19 del / L858R (1st/2nd-gen TKI) | T790M exon 20 mutation → use Osimertinib |
| EGFR + Osimertinib | C797S mutation, MET amplification, HER2 amplification, histological transformation to SCLC |
| ALK (Crizotinib) | Secondary ALK domain mutations (L1196M, G1202R) → use Alectinib/Lorlatinib |
| KRAS G12C (Sotorasib) | KRAS amplification, Y96D mutation, bypass pathway activation |
9. KEY EXAM QUESTIONS — MD PATHOLOGY
Q1. Which molecular mutation is most common in never-smoking Asian women with lung adenocarcinoma?
A: EGFR mutation (exon 19 deletion or L858R — exon 21)
Q2. What is the most common acquired resistance mutation after EGFR-TKI therapy?
A: T790M mutation (exon 20) — overcome by Osimertinib
Q3. ALK gene rearrangement in lung cancer: typical patient profile?
A: Young, non-smoker/light smoker, adenocarcinoma with signet-ring cell features; EML4-ALK fusion; predilection for CNS metastasis; treated with Alectinib (1st line)
Q4. Name the molecular markers tested routinely in metastatic NSCLC adenocarcinoma.
A: EGFR, KRAS, ALK, ROS1, BRAF V600E, RET, NTRK, MET exon 14, HER2, PD-L1, TMB (by NGS panel)
Q5. Which tumor suppressor gene is lost in virtually ALL small cell lung cancers?
A: RB1 (retinoblastoma gene) — nearly universal loss, along with TP53
Q6. What is the difference between a driver mutation and a passenger mutation?
A: Driver mutations confer selective growth/survival advantage and are clonally preserved; passenger mutations are genetically irrelevant to tumor progression
Q7. Which mutation is associated with immunotherapy resistance despite high tumor mutational burden?
A: STK11/LKB1 mutation (associated with KRAS co-mutation, cold immune microenvironment)
Q8. PD-L1 testing: what cutoff is used for pembrolizumab monotherapy?
A: TPS ≥50% (first line monotherapy); TPS 1–49% → combination chemo-immunotherapy
Q9. KRAS mutation: frequency, typical patient, and first approved targeted drug?
A: ~25–30% NSCLC; smokers, Western populations; KRAS G12C targeted by Sotorasib (AMG 510)
Q10. What is "field cancerization" in the context of lung cancer?
A: Widespread DNA damage from carcinogen (tobacco) exposure across respiratory epithelium, predisposing to multiple independent primary tumors; explains why lung cancer patients can develop second primaries
Q11. Name neuroendocrine markers used in diagnosing SCLC.
A: Chromogranin A, Synaptophysin, CD56, Neuron-Specific Enolase (NSE); also TTF-1+ in ~90% SCLC
Q12. What is liquid biopsy and when is it used in lung cancer management?
A: Blood-based detection of circulating tumour DNA (ctDNA) by sequencing; used at initial diagnosis (if tissue unavailable), at progression (to detect resistance mutations), and for monitoring disease response
Q13. Immunohistochemical profile of adenocarcinoma vs. squamous cell carcinoma?
A: Adenocarcinoma: TTF-1+, Napsin A+; Squamous: p40+, p63+, CK5/6+, TTF-1−
Q14. What molecular subtypes of SCLC are recognized, and what drives their heterogeneity?
A: Defined by transcription factor expression (ASCL1-high, NEUROD1-high, POU2F3-high, YAP1-high); cellular plasticity and subpopulation communication drives chemo-resistance; no targetable driver mutations yet identified
10. SUMMARY TABLE — MOLECULAR MARKERS AT A GLANCE
| Marker | Histotype | Frequency | Drug | Prognosis |
|---|---|---|---|---|
| EGFR exon 19 del / L858R | Adeno | 9–46% | Osimertinib | Good |
| KRAS G12C | Adeno | ~25–30% | Sotorasib | Poor → improving |
| ALK fusion (EML4-ALK) | Adeno | ~5% | Alectinib | Good |
| ROS1 fusion | Adeno | 1–2% | Crizotinib, Entrectinib | Good |
| BRAF V600E | Adeno | 2–4% | Dabrafenib+Trametinib | Moderate |
| RET fusion | Adeno | 1–2% | Selpercatinib | Good |
| NTRK fusion | Any | <1% | Larotrectinib | Good |
| MET exon 14 skip | Adeno | 3–4% | Capmatinib | Moderate |
| HER2 (ERBB2) mutation | Adeno | ~3% | T-DM1 | Moderate |
| TP53 mutation | All | >50% | None targeted | Poor |
| RB1 loss | SCLC | ~100% | None targeted | Very poor |
| PD-L1 TPS ≥50% | Any | Variable | Pembrolizumab | Better immuno Rx |
| High TMB | Any | Variable | Checkpoint inhibitors | Better immuno Rx |
Sources: Murray & Nadel's Textbook of Respiratory Medicine, Chapter 73; Robbins Basic Pathology (Robbins & Kumar); Henry's Clinical Diagnosis & Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.