General lab diagnosis for fungal infection
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive content now. Let me compile the full, detailed answer.
General Laboratory Diagnosis of Fungal Infections
Diagnosis of fungal infections depends on three core laboratory approaches: (1) Microbiologic, (2) Immunologic/Biochemical, and (3) Histopathologic. These are supplemented by molecular methods. Prompt diagnosis requires clinical suspicion, proper specimen collection, and integration of findings across all modalities.
1. Specimen Collection and Processing
Proper collection is the foundation of lab diagnosis. Key principles:
- Collect specimens before starting antifungal therapy when possible.
- Specimen type depends on suspected site: skin/nail scrapings, BAL/sputum, blood, CSF, tissue biopsy, urine, or wound swabs.
- Specimens for culture should not be fixed in formalin (which kills organisms). Tissue sent to anatomical pathology is formalin-fixed and cannot be cultured.
- For biosafety: Coccidioides spp. in culture form are classified as Category A infectious substance (higher risk) and require BSL-3 handling.
2. Microbiologic Methods
A. Direct Microscopy (Stains)
Direct microscopy is among the most rapid and cost-effective methods - results available in under an hour vs. days/weeks for culture. It can detect and sometimes identify fungi by distinctive morphology.
| Stain | Fungi Detected | Notes |
|---|---|---|
| Calcofluor white | Broad (all fungi) | Binds cell walls; fungi fluoresce bright green/blue-white under UV; fastest and most sensitive direct exam |
| Gram stain | Yeasts (Candida, Cryptococcus), molds (Aspergillus) | Fungi typically gram-positive but may appear speckled or gram-negative |
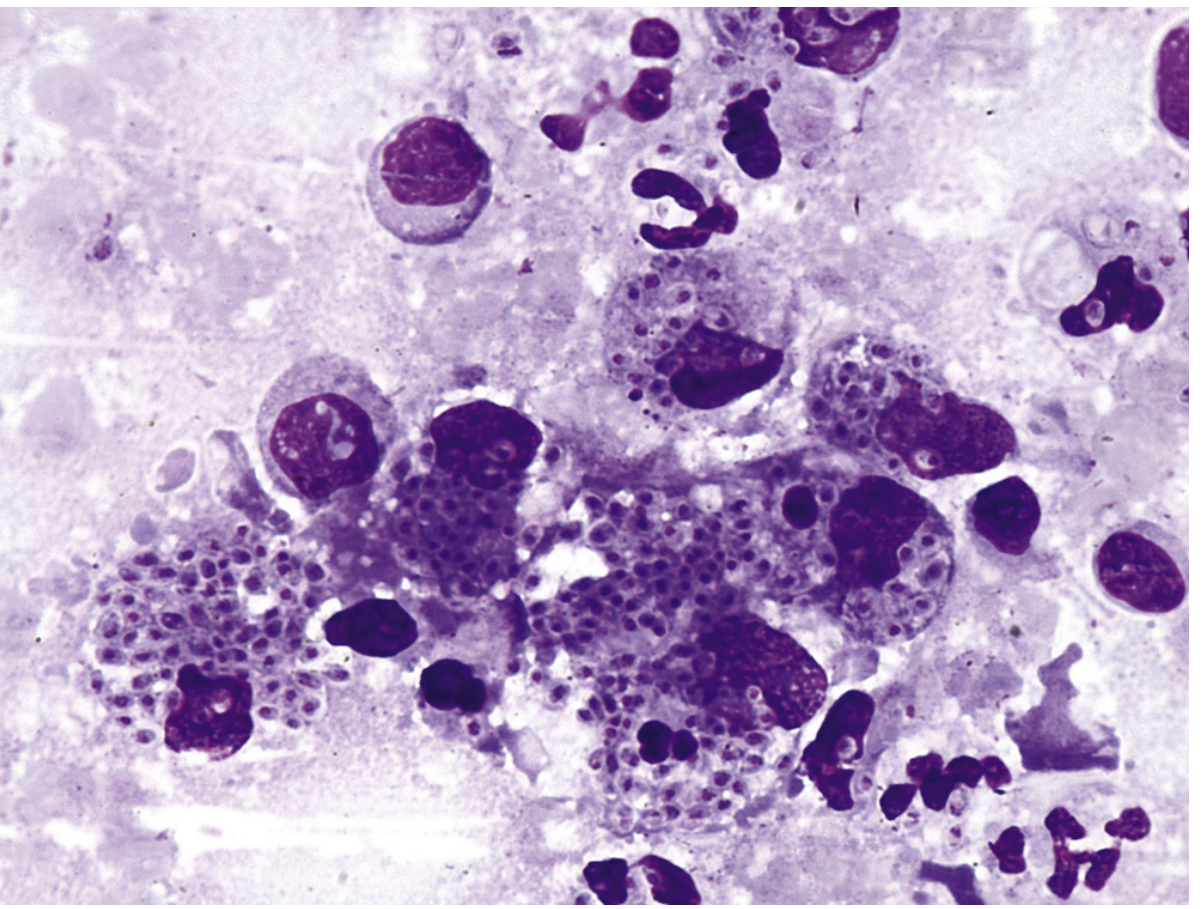
| Giemsa stain | Histoplasma capsulatum (intracellular yeast) | Especially useful in peripheral blood smears, bone marrow, touch preps |
| KOH (potassium hydroxide) | Dermatophytes, most fungi | Dissolves keratin; used for skin/nail/hair - reveals hyphae |
| India Ink | Cryptococcus neoformans | Capsule appears as clear halo around yeast; used on CSF |
| Gomori Methenamine Silver (GMS) | All fungi (histopath) | Stains fungal cell walls black; very sensitive |
| PAS (Periodic Acid-Schiff) | All fungi (histopath) | Stains cell walls magenta; useful in tissue sections |
| Mucicarmine | Cryptococcus capsule | Stains polysaccharide capsule red; specific for Cryptococcus |
| H&E | General screening | Less sensitive for fungi alone; used as baseline |
Fig. 60.1 - Calcofluor white showing budding yeasts and pseudohyphae of Candida albicans:
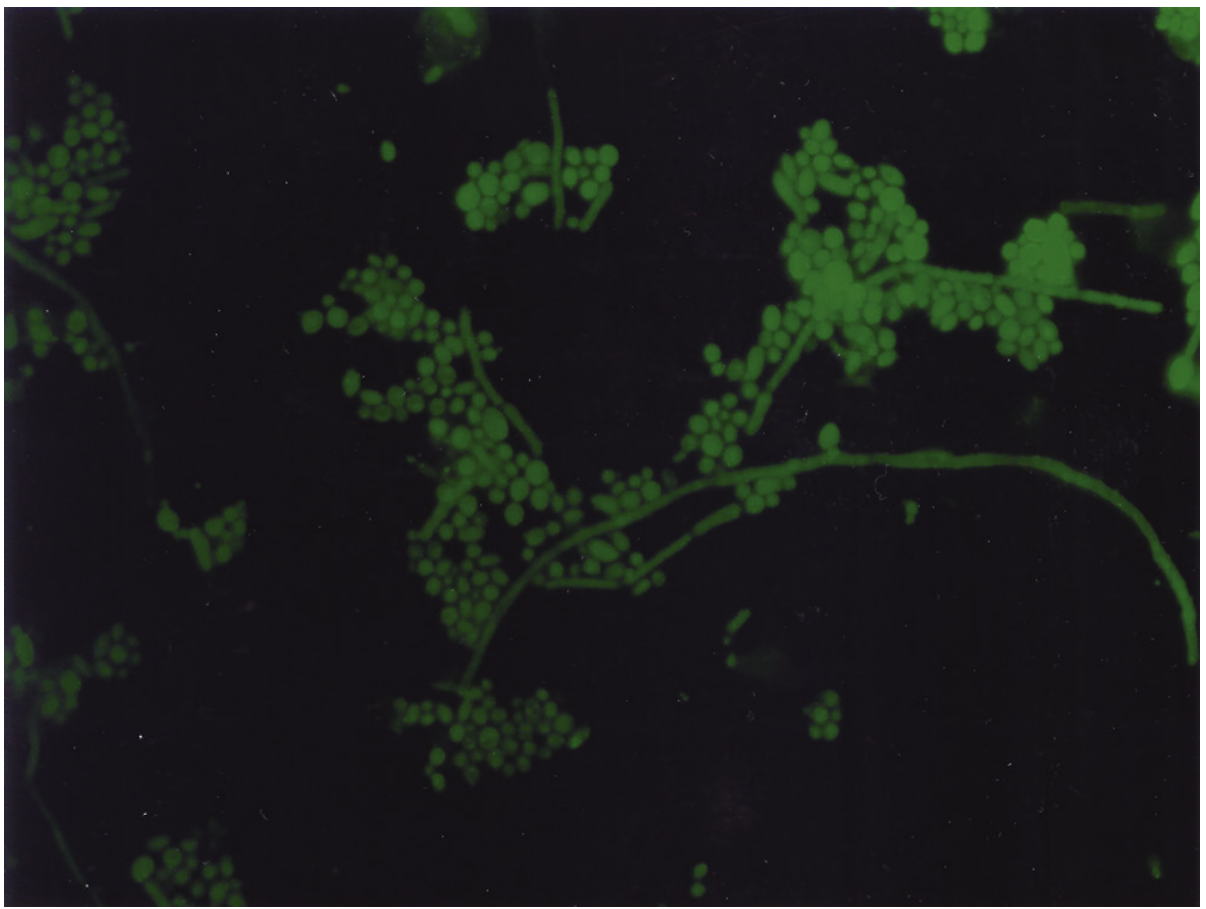
Fig. 60.4 - Giemsa stain showing intracellular Histoplasma capsulatum yeast forms:
Important: Microscopy is less sensitive than culture. A negative direct exam does NOT rule out fungal infection. Both false-positives and false-negatives occur.
Morphologic characteristics that allow etiologic diagnosis by microscopy alone:
- Pneumocystis jirovecii - characteristic cysts (in BAL/induced sputum)
- Histoplasma capsulatum - intracellular yeast in macrophages
- Blastomyces dermatitidis - broad-based budding yeast
- Coccidioides immitis/posadasii - large spherules with endospores
B. Fungal Culture
Culture remains the gold standard for definitive diagnosis and is required for species identification and antifungal susceptibility testing. Disadvantages include slow turnaround (days to weeks) and the potential for contamination.
Common Culture Media:
| Media | Purpose |
|---|---|
| Sabouraud Dextrose Agar (SDA) | General-purpose; primary isolation for most pathogenic fungi |
| Inhibitory Mold Agar (IMA) | Contains chloramphenicol to inhibit bacteria; good for molds |
| Dermatophyte Test Agar (DTA/DTM) | Selective for dermatophytes; contains cycloheximide + antibacterials; color change indicator |
| Brain Heart Infusion (BHI) Agar | Enriched; for dimorphic and fastidious fungi |
| Birdseed Agar (Niger Seed Agar) | Selective/differential for Cryptococcus - colonies turn tan/brown due to phenol oxidase |
| Candida Chromogenic Agar | Differential; C. albicans = green, C. tropicalis = blue, C. krusei = pink/purple |
| Dixon's Agar / Leeming-Notman Agar | Primary isolation of Malassezia spp. (lipid-supplemented) |
| Mycobiotic / Mycosel Agar | Contains cycloheximide; for dermatophytes and dimorphic fungi; inhibits saprobes |
Note: Cycloheximide inhibits many saprophytic/rapidly growing fungi but must not be used alone - many pathogens (e.g., Cryptococcus, Aspergillus) are also susceptible to cycloheximide.
Culture incubation: Most fungi are incubated at 25-30°C (room temperature) for molds, and at 35-37°C for yeasts and dimorphic fungi (in their yeast phase).
C. Organism Identification
After culture, identification is done by:
- Morphology - colony appearance, pigmentation, texture, growth rate
- Microscopic morphology - hyphal structure, conidia, spore arrangement
- MALDI-TOF MS (Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry) - now widely used; provides rapid, accurate species-level identification from cultured isolates within minutes; a major advance in clinical mycology
- Biochemical tests - germ tube test (C. albicans), urease test (Cryptococcus, Trichosporon), phenol oxidase test
- Molecular methods (see below)
D. Antifungal Susceptibility Testing (AST)
- Done by broth microdilution (CLSI or EUCAST methods) or disk diffusion (limited utility for fungi)
- Determines MIC (minimum inhibitory concentration) for azoles, echinocandins, polyenes, etc.
- Important for guiding therapy in resistant species (e.g., azole-resistant Aspergillus fumigatus, Candida auris)
3. Immunologic Methods
Useful for rapid, non-culture-based detection, especially in invasive infections where culture sensitivity may be low.
Antigen Detection
| Test | Organism | Specimen | Method |
|---|---|---|---|
| Cryptococcal Antigen (CrAg) | Cryptococcus neoformans/gattii | Serum, CSF | Latex agglutination (LA), EIA, Lateral Flow Device (LFD) - LFD is POC capable |
| Galactomannan (GM) | Aspergillus spp. | Serum, BAL | EIA; cell wall polysaccharide marker; serial monitoring in high-risk patients |
| 1,3-β-D-Glucan (BDG) | Pan-fungal (Candida, Aspergillus, PCP, most fungi) | Serum | Limulus-based test; NOT positive for Cryptococcus or Mucorales |
| Histoplasma Antigen | Histoplasma capsulatum | Urine, serum | EIA/RIA; most sensitive in disseminated histoplasmosis |
| Blastomyces Antigen | Blastomyces dermatitidis | Urine, serum | EIA; cross-reacts with Histoplasma |
Antibody Detection
- Used mainly for endemic mycoses in immunocompetent hosts (who can mount an antibody response)
- Coccidioidomycosis: complement fixation (CF) and immunodiffusion (ID)
- Histoplasmosis: immunodiffusion, complement fixation
- Aspergillus precipitins (IgG) - for allergic bronchopulmonary aspergillosis (ABPA) and chronic pulmonary aspergillosis
- Limitation: Poor sensitivity in immunocompromised patients (cannot mount antibody response)
4. Histopathologic Methods
The anatomical pathology lab provides definitive evidence of invasive disease by showing tissue invasion. Stains used in histopath are generally more sensitive than clinical mycology lab stains.
| Stain | Use |
|---|---|
| H&E | Background; shows tissue reaction (granulomas, abscesses) |
| GMS (Gomori Methenamine Silver) | Stains all fungal cell walls black against green background; gold standard for tissue |
| PAS (Periodic Acid-Schiff) | Fungi stain magenta/red; good counterstain |
| Mucicarmine | Stains Cryptococcus capsule red; specific |
| Direct Immunofluorescence | Antibody-based; specific organism detection in tissue |
| In Situ Hybridization (ISH) | Nucleic acid-based; for non-culturable organisms like P. jirovecii, Rhinosporidium seeberi |
Histopath enables etiologic diagnosis of dimorphic fungi and non-culturable organisms (P. jirovecii, Rhinosporidium seeberi) based on characteristic morphology in tissue.
5. Molecular Methods
Rapidly expanding area; allow direct detection from clinical specimens without culture.
- PCR/Nucleic Acid Amplification Tests (NAATs) - detect fungal DNA directly from blood, BAL, CSF, tissue
- Aspergillus PCR (BAL preferred): included in ESCMID diagnostic algorithm
- Pneumocystis jirovecii PCR: high sensitivity from BAL
- Candida PCR: emerging role for bloodstream infection
- T2 Candida Panel (T2 Biosystems): detects 5 Candida spp. directly from whole blood in ~3-5 hours, without waiting for positive blood culture
- ITS (Internal Transcribed Spacer) sequencing - universal fungal identifier; sequences the 18S-ITS1-5.8S-ITS2-28S rRNA gene region for species-level ID
- Whole Genome Sequencing (WGS) - for outbreak investigation, strain typing (e.g., Candida auris outbreaks)
- Multiplex platforms - e.g., FilmArray, MALDI-TOF for rapid broad-range detection
6. Biochemical Methods
| Marker | Organism | Method |
|---|---|---|
| D-Arabinitol | Candida (metabolite in bloodstream infection) | Enzymatic assay / GC-MS |
| D-Mannitol | Cryptococcus, Aspergillus | GC-MS |
| Cell wall chitin | Broad | Spectrophotometry |
Summary: Comparison of Methods
| Method | Speed | Sensitivity | Species ID? | Notes |
|---|---|---|---|---|
| Direct microscopy | Minutes to 1 hr | Low-moderate | Sometimes | Best for rapid guidance |
| Culture | Days to weeks | High (gold standard) | Yes (with MALDI-TOF) | Required for AST |
| Antigen detection | Hours | High (organism-specific) | Indirect | Best for invasive infections |
| Serology (antibody) | Hours | Poor in immunocompromised | No | Best in endemic mycoses |
| Histopath | 1-3 days | High | Sometimes | Definitive proof of invasion |
| Molecular (PCR) | Hours | High | Yes | No culture needed; emerging standard |
Sources:
- Medical Microbiology, 9e, Ch. 60 - Conventional Laboratory Diagnosis of Fungal Infections
- Tietz Textbook of Laboratory Medicine, 7th Ed., Ch. 87 - Clinical Mycology and Anatomical Pathology
This is a shared conversation. Sign in to Orris to start your own chat.