Lung surfectant
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile a complete, well-structured answer.
Pulmonary Surfactant
What Is It?
Pulmonary surfactant is a complex mixture of lipids (~90%) and proteins (~10%) secreted into the alveolar space by Type II alveolar (AT2) pneumocytes. Its primary role is to reduce surface tension at the air-liquid interface of alveoli, preventing alveolar collapse at end-expiration.
Composition
Lipids (85% phospholipids + 5% neutral lipids)
The most important constituent is dipalmitoylphosphatidylcholine (DPPC), which accounts for ~47% of all phospholipids. Full breakdown:
| Component | % of Phospholipids |
|---|---|
| Phosphatidylcholine (total) | 76.3% |
| - DPPC (saturated) | 47.0% |
| - Unsaturated PC | 29.3% |
| Phosphatidylglycerol | 11.6% |
| Phosphatidylinositol | 3.9% |
| Phosphatidylethanolamine | 3.3% |
| Sphingomyelin | 1.5% |
| Neutral lipids (cholesterol, free fatty acids) | 5% of total |
DPPC molecules are amphipathic - hydrophobic tails repel water and align at the air-liquid interface, while hydrophilic heads face the aqueous phase. This disrupts the intermolecular forces between water molecules that would otherwise generate high surface tension.
- Murray & Nadel's Textbook of Respiratory Medicine, Table 3.2
Proteins (~10%)
There are four surfactant-associated proteins:
| Protein | Abundance | Main Role |
|---|---|---|
| SP-A | Most abundant (++++) | Host defense; collagenous glycoprotein (18-mer); binds carbohydrates/pathogens via C-type lectin domain |
| SP-B | Low (+) | Biophysical function; regulates surfactant lipid spreading; required for lamellar body formation |
| SP-C | Low (+) | Biophysical function; stabilizes lipid film during compression |
| SP-D | Moderate (++) | Host defense; collectin; opsonization, pathogen binding |
SP-A and SP-D belong to the collectin family and are secreted via a distinct pathway (not lamellar bodies). SP-B and SP-C are packaged in lamellar bodies and secreted together with lipids.
- Murray & Nadel's Textbook of Respiratory Medicine
Mechanism of Action - The Law of Laplace
By the law of Laplace, the collapsing pressure of a sphere is:
P = 2T / r
where T = surface tension and r = radius.
This means small alveoli face greater collapsing pressure than large ones. Surfactant solves this by reducing T proportionally as radius decreases - as alveoli shrink at end-expiration, surfactant molecules pack more densely, lowering surface tension further and stabilizing the alveolus.
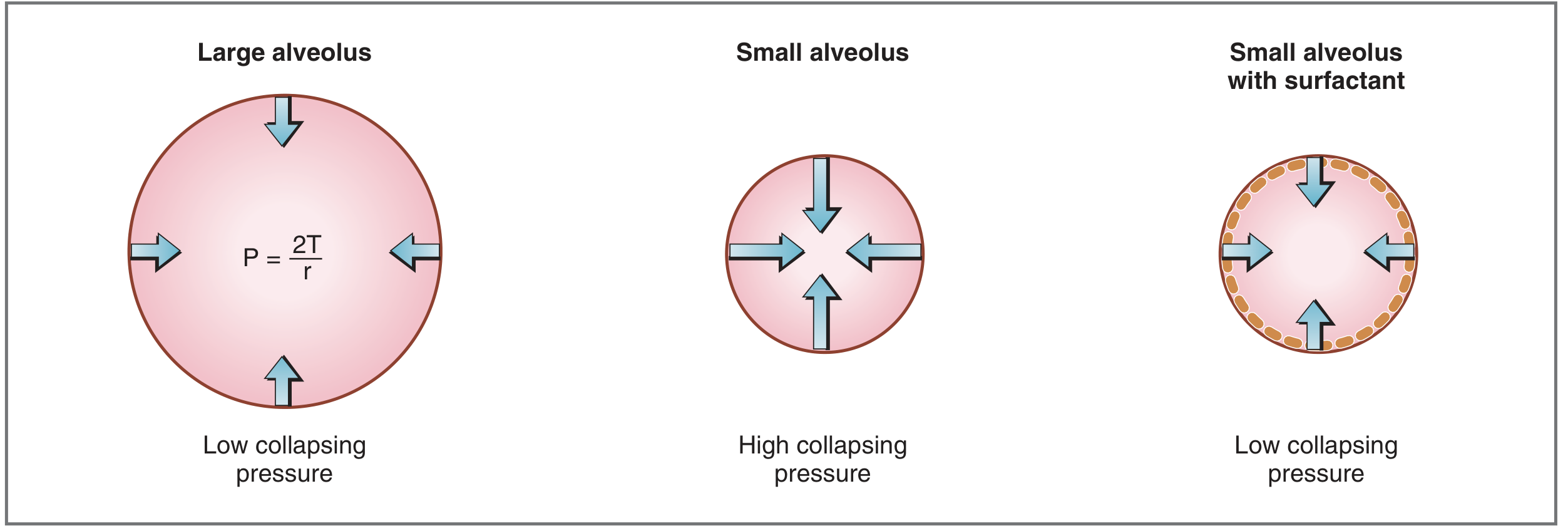
Fig. 5.12 - Costanzo Physiology: A large alveolus has low collapsing pressure (large r). A small alveolus without surfactant has high collapsing pressure (small r, high T). A small alveolus WITH surfactant has low collapsing pressure because surfactant reduces T.
Physiological Effects
- Prevents atelectasis - keeps small alveoli from collapsing at end-expiration
- Increases lung compliance - reduces the work of breathing during inspiration
- Stabilizes alveoli of different sizes - prevents larger alveoli from absorbing smaller ones (without surfactant, high pressure in small alveoli would push air into large ones per Laplace's law)
- Host defense - SP-A and SP-D opsonize pathogens, regulate alveolar macrophage function, and modulate inflammatory responses
- Costanzo Physiology 7th Edition
Synthesis, Secretion & Regulation
- Cell of origin: Type II alveolar epithelial (AT2) cells; SP-A and SP-D are also expressed in club cells of bronchioles
- Storage: Lipids, SP-B, and SP-C are stored in lamellar bodies before secretion
- Secretion trigger: β-adrenergic receptor activation, P2X7R purinergic receptors; mediated by intracellular cAMP and Ca²⁺
- Onset in fetal lung: Synthesis begins around gestational week 24, nearly complete by week 35
- Regulation:
- Stimulated by: Glucocorticoids (via lung fibroblasts), EGF, cAMP, thyroxine
- Inhibited by: TNF-α, TGF-β, insulin
- Transcription factors: TTF-1, FOXA2, CREBPA, GATA proteins, RARs, SREBP
Antenatal glucocorticoids (betamethasone/dexamethasone) are administered to mothers at risk of preterm delivery to accelerate fetal surfactant synthesis and reduce the risk of infant respiratory distress syndrome (IRDS).
- Fishman's Pulmonary Diseases and Disorders
Clearance
- Surfactant is primarily recycled by AT2 cells (uptake and repackaging into lamellar bodies)
- A smaller fraction is cleared by alveolar macrophages via a GM-CSF-dependent pathway
- GM-CSF signaling is essential for macrophage-mediated surfactant catabolism - deficiency leads to pulmonary alveolar proteinosis (PAP), where surfactant accumulates in alveoli
Clinical Relevance
| Condition | Mechanism | Notes |
|---|---|---|
| Neonatal RDS (IRDS) | Surfactant deficiency in premature infants | Hyaline membranes, atelectasis, hypoxemia; treated with exogenous surfactant replacement therapy (e.g., beractant, poractant alfa) |
| ARDS | Surfactant inactivation/dysfunction | Inflammatory mediators (TNF-α, phospholipases) inactivate surfactant; surfactant replacement has NOT proven effective in adult ARDS trials |
| Pulmonary Alveolar Proteinosis (PAP) | Impaired surfactant clearance | GM-CSF autoantibodies (autoimmune PAP) or receptor mutations; "crazy paving" on CT; PAS-positive alveolar material |
| SP-B deficiency | Inherited; absent SP-B | Fatal neonatal respiratory failure; dysfunctional surfactant; PAS-positive alveolar material |
| ABCA3 mutations | Absent lamellar bodies | Impaired surfactant packaging and secretion; neonatal/childhood respiratory failure |
| Hyperoxic lung injury / N-mustard | AT2/AT1 cell death | Surfactant inactivation + inflammatory recruitment |
- Murray & Nadel's Textbook of Respiratory Medicine, Table 3.1
Lamellar Body to Tubular Myelin
After secretion, surfactant lipids and proteins organize into tubular myelin - a lattice-like structure that serves as the reservoir for rapid surface film formation at the air-liquid interface. This conversion requires SP-A, SP-B, and calcium.
Key takeaway: Surfactant is not just a "soap" for the lungs - it is a dynamically regulated bioactive system with biophysical and immunological roles, whose dysfunction underlies some of the most serious respiratory diseases across all age groups.
This is a shared conversation. Sign in to Orris to start your own chat.