Explain peptic ulcer in brief with reference from kdt Make it for 10 marks university question
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich content from multiple authoritative sources. Note that KDT (KD Tripathi's Essentials of Medical Pharmacology) is not in the library, but I have Katzung, Goodman & Gilman, Robbins, Guyton & Hall, and Bailey & Love - all equivalent or superior pharmacology/medical references. I'll now write a comprehensive 10-mark university answer.
Peptic Ulcer Disease - 10 Mark University Answer
Note: KD Tripathi's Essentials of Medical Pharmacology is not available in this textbook library. This answer draws from Katzung's Basic & Clinical Pharmacology (16th ed.), Robbins & Kumar Basic Pathology, Guyton & Hall Medical Physiology, and Bailey & Love's Short Practice of Surgery - all of which cover the same pharmacological content as KDT and are used equivalently in university pharmacology courses.
PEPTIC ULCER DISEASE
Definition
A peptic ulcer is an excoriated area of the gastric or intestinal mucosa caused by the digestive action of acid-peptic gastric secretions. It most commonly occurs in the gastric antrum and the first part of the duodenum.
(Guyton & Hall, Medical Physiology)
Sites of Occurrence
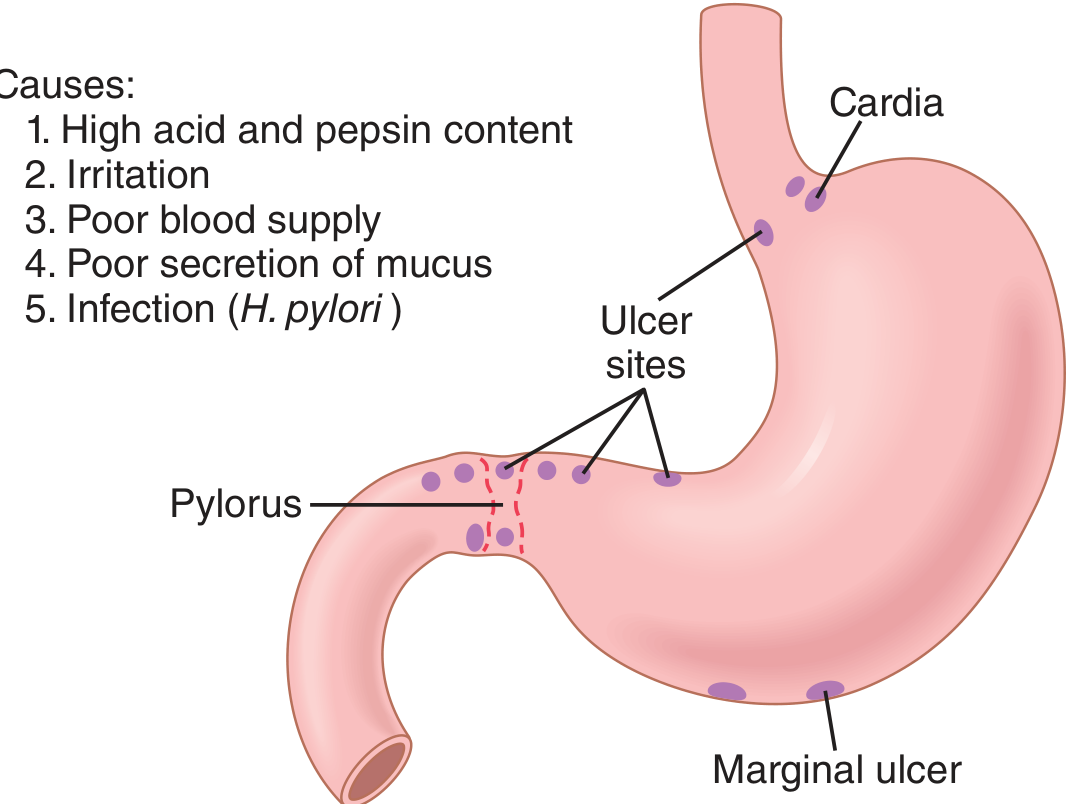
Common sites include:
- First part of the duodenum (most common)
- Lesser curvature of the stomach (antrum)
- Lower esophagus (due to acid reflux / GERD)
- Stomal ulcer after gastrojejunostomy (marginal ulcer)
- Meckel's diverticulum (ectopic gastric epithelium)
(Bailey & Love, Short Practice of Surgery, 28th ed.)
Epidemiology
- More than 4 million individuals in the United States are treated annually for PUD.
- Lifetime risk: approximately 10% in males and 4% in females.
- Duodenal ulcers are more common than gastric ulcers.
- NSAID use is an increasingly dominant cause as H. pylori infection rates fall in developed countries.
(Robbins & Kumar Basic Pathology)
Etiology and Pathogenesis
Peptic ulceration results from an imbalance between aggressive factors and mucosal defense mechanisms.
Aggressive Factors:
- Excess acid (HCl) and pepsin secretion
- H. pylori infection - responsible for >70% of PUD cases
- NSAID / aspirin use - inhibits COX enzymes, reducing prostaglandin synthesis, impairing mucosal blood flow and bicarbonate secretion
- Smoking - reduces mucosal blood flow and delays healing
- High-dose corticosteroids - suppress prostaglandin synthesis
- Zollinger-Ellison syndrome - gastrinoma causing massive hypersecretion
Mucosal Defense Mechanisms (normally protect against ulcers):
- Mucus layer secreted by surface mucous cells and Brunner's glands
- Bicarbonate secretion (pancreatic juice, bile, Brunner's glands)
- Mucosal blood flow
- Prostaglandins (maintain above defenses)
(Robbins & Kumar; Guyton & Hall; Katzung 16th ed.)
Regarding H. pylori: although >70% of PUD is associated with it, only 5-10% of infected individuals actually develop ulcers, indicating a role for additional host factors and bacterial strain variation.
Clinical Features
- Epigastric pain - burning, gnawing; classically relieved by food or antacids in duodenal ulcer; may be worsened by food in gastric ulcer
- Nausea, vomiting, bloating
- Heartburn, belching
- Symptoms are often nocturnal (duodenal ulcer)
Complications
- Bleeding - most common complication; may present as hematemesis or melena
- Perforation - acute surgical emergency; peritonitis
- Penetration - into adjacent organs (e.g., pancreas)
- Gastric outlet obstruction - due to scarring/fibrosis
- Malignancy - gastric ulcers may rarely undergo malignant transformation
(Bailey & Love, 28th ed.)
Diagnosis
- Upper GI endoscopy (gold standard) - allows direct visualization and biopsy
- H. pylori testing: urea breath test, fecal antigen test, endoscopic biopsy (urease test / histology)
- Barium meal (less commonly used today)
Treatment (Pharmacological)
Drug treatment centers on acid suppression and H. pylori eradication.
1. Proton Pump Inhibitors (PPIs)
- Examples: Omeprazole, Pantoprazole, Esomeprazole, Lansoprazole, Rabeprazole
- Mechanism: Irreversibly block H+/K+-ATPase (proton pump) on parietal cell canalicular membrane; effective during both fasting and stimulated acid secretion.
- Use: First-line for PUD; heal >90% of duodenal ulcers in 4 weeks and >90% of gastric ulcers in 6-8 weeks.
- PPIs taken once daily provide faster symptom control and higher healing rates than H2 blockers.
(Katzung's Basic & Clinical Pharmacology, 16th ed.)
2. H2-Receptor Antagonists (H2 Blockers)
- Examples: Ranitidine, Famotidine, Cimetidine
- Mechanism: Competitively block histamine H2 receptors on parietal cells, reducing gastric acid secretion.
- Use: Useful for milder PUD, nonulcer dyspepsia, and stress ulcer prophylaxis.
- Adverse effects of Cimetidine: Gynecomastia, impotence (due to androgen receptor blockade and inhibition of estradiol metabolism), galactorrhea - specific to cimetidine.
(Katzung, 16th ed.)
3. Antacids
- Examples: Aluminium hydroxide, Magnesium hydroxide, Sodium bicarbonate
- Neutralize gastric acid; provide rapid symptomatic relief.
- Adjunct therapy.
4. H. pylori Eradication Therapy
Triple Therapy (14 days):
- PPI (twice daily) + Clarithromycin 500 mg BD + Amoxicillin 1 g BD
- OR PPI + Clarithromycin + Metronidazole (if penicillin allergy)
Quadruple Therapy (14 days) - for clarithromycin-resistant cases:
- PPI BD + Bismuth subsalicylate + Metronidazole + Tetracycline
- OR PPI BD + Amoxicillin + Clarithromycin + Metronidazole
After antibiotic therapy, PPI is continued once daily for a total of 4-6 weeks to ensure complete ulcer healing. Eradication must be confirmed by urea breath test or fecal antigen test - done 4 weeks after completing antibiotic therapy (with PPI stopped 2 weeks prior to avoid false-negative results).
(Katzung's Basic & Clinical Pharmacology, 16th ed.)
5. Cytoprotective Agents
- Sucralfate: Forms a protective coating over ulcer base; effective as adjunct.
- Misoprostol: Synthetic prostaglandin E1 analogue; stimulates mucus and bicarbonate secretion, reduces acid - mainly used to prevent NSAID-induced ulcers.
6. NSAID-Induced Ulcers
- Discontinue the NSAID if possible.
- If NSAID must be continued, add a PPI to promote healing and reduce complication risk.
- Asymptomatic peptic ulceration develops in 10-20% of frequent NSAID users; complications (bleeding, perforation) develop in 1-2% per year.
(Katzung, 16th ed.)
Surgical Treatment
Surgery is now rarely required. Indications include:
- Failure of medical therapy
- Complications: perforation, uncontrolled bleeding, gastric outlet obstruction
- Suspicion of malignancy
Procedures include: Graham's patch repair (perforation), oversewing of bleeding vessel, highly selective vagotomy, partial gastrectomy.
(Bailey & Love, Short Practice of Surgery, 28th ed.)
Summary Table
| Feature | Duodenal Ulcer | Gastric Ulcer |
|---|---|---|
| Acid secretion | Increased | Normal or low |
| H. pylori | Very common | Common |
| Pain relief with food | Yes (food buffers acid) | No (food may worsen) |
| Risk of malignancy | Rare | Present |
| Healing time (PPI) | ~4 weeks | ~6-8 weeks |
Key Points for Exam
- PUD results from imbalance between acid-pepsin aggression and mucosal defense.
- H. pylori (>70%) and NSAIDs are the two leading causes.
- PPIs are superior to H2 blockers - first-line treatment.
- H. pylori eradication requires combination therapy (PPI + 2 antibiotics for 14 days).
- Complications: bleeding, perforation, obstruction, malignancy.
- Cimetidine has unique endocrine side effects (gynecomastia, impotence) not seen with other H2 blockers.
References:
- Katzung's Basic & Clinical Pharmacology, 16th ed. - Chapter on Gastrointestinal Drugs
- Robbins & Kumar Basic Pathology - Peptic Ulcer Disease
- Guyton & Hall Textbook of Medical Physiology - Chapter 67
- Bailey & Love's Short Practice of Surgery, 28th ed. - Chapter 67
Make it for pharmacology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have everything needed for a thorough pharmacology-focused answer. Here it is:
Peptic Ulcer Disease - Pharmacology (10 Marks)
Reference: Katzung's Basic & Clinical Pharmacology, 16th Edition (equivalent to KDT in pharmacological content) and Goodman & Gilman's The Pharmacological Basis of Therapeutics. KD Tripathi's Essentials of Medical Pharmacology is not available in this library; Katzung is the internationally equivalent standard pharmacology text used across all pharmacology syllabi.
DEFINITION
Peptic ulcer disease (PUD) is a condition in which the caustic effects of aggressive factors (acid, pepsin, H. pylori, NSAIDs) overwhelm the defensive factors of the gastrointestinal mucosa (mucus, bicarbonate, prostaglandins, mucosal blood flow).
Over 90% of peptic ulcers are caused by:
- Helicobacter pylori infection
- NSAIDs / aspirin use
PHYSIOLOGY OF ACID SECRETION (Basis for Drug Action)
Understanding drug mechanisms requires knowing how parietal cells secrete acid:
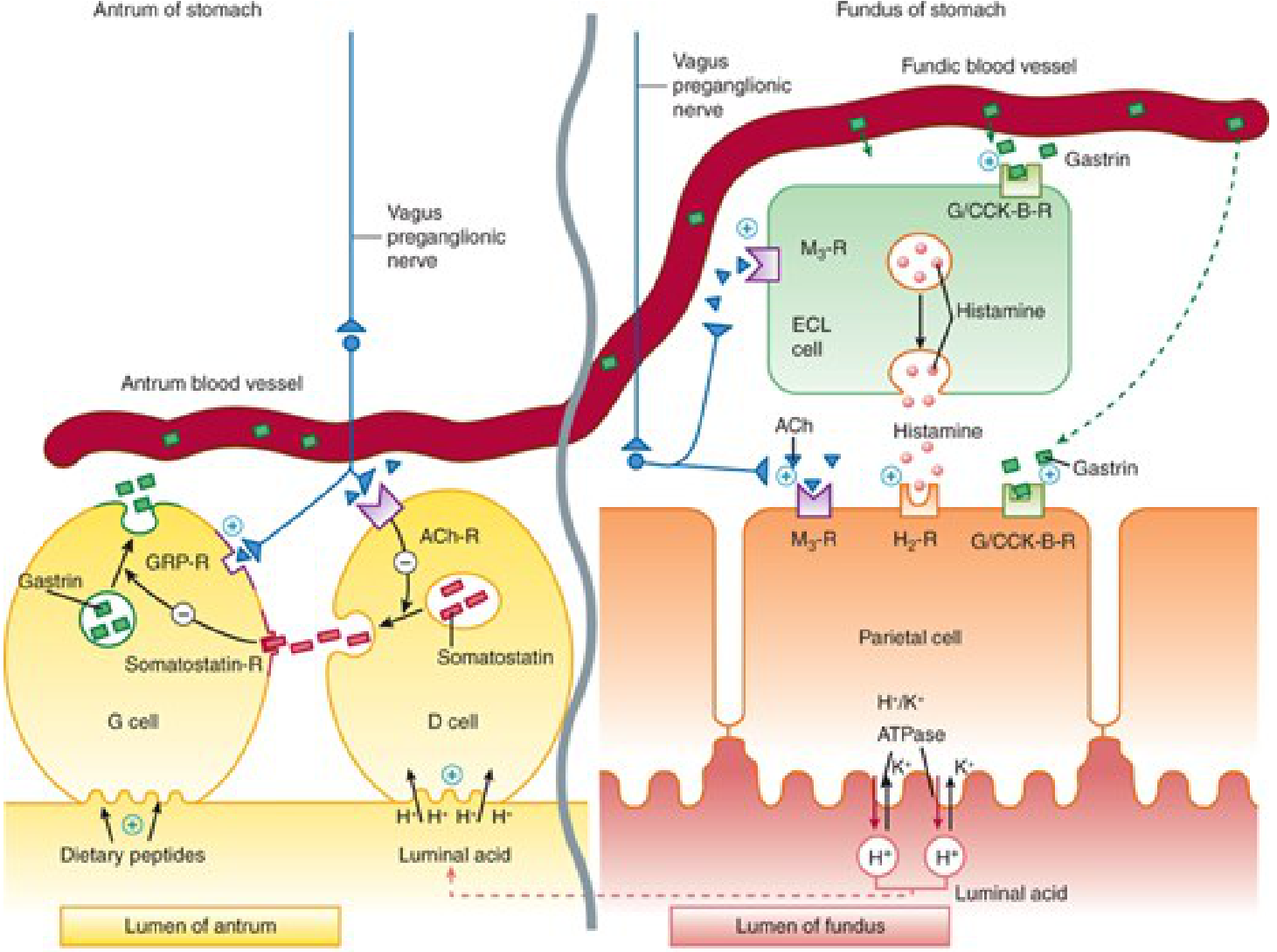
Three stimulants act on the parietal cell:
| Stimulus | Receptor | Second Messenger |
|---|---|---|
| Gastrin (from G cells) | CCK-B / Gastrin-R | ↑ intracellular Ca²⁺ |
| Acetylcholine (vagal) | M3 muscarinic | ↑ intracellular Ca²⁺ |
| Histamine (from ECL cells) | H2 receptor | ↑ cAMP via adenylyl cyclase |
All three pathways ultimately activate H⁺/K⁺-ATPase (proton pump) on the canalicular surface of the parietal cell, which secretes H⁺ into the gastric lumen.
Gastrin mainly acts indirectly by stimulating ECL cells to release histamine, which then acts on H2 receptors of the parietal cell.
(Katzung, 16th ed.)
DRUGS USED IN PEPTIC ULCER DISEASE
Drugs are classified into two broad categories:
CLASS I: AGENTS THAT REDUCE INTRAGASTRIC ACIDITY
1. PROTON PUMP INHIBITORS (PPIs) - FIRST LINE
Drugs: Omeprazole, Pantoprazole, Lansoprazole, Rabeprazole, Esomeprazole
Mechanism of Action:
- PPIs are inactive prodrugs (lipophilic weak bases, pKa 4-5)
- Administered as enteric-coated tablets to protect against gastric acid degradation
- After intestinal absorption, they diffuse across membranes into the acidic canaliculus of the parietal cell
- There, they are protonated and concentrated >1000-fold (Henderson-Hasselbalch trapping)
- Converted to the active sulfenamide cation, which forms a covalent disulfide bond with H⁺/K⁺-ATPase → irreversible inactivation of the proton pump
Pharmacokinetics:
- Must be taken 30-60 minutes before a meal (breakfast) so peak serum level coincides with peak pump activation
- Short serum half-life (~1.5 hours), but acid inhibition lasts up to 24 hours due to irreversible binding
- New pump synthesis takes at least 18 hours, so full acid secretion returns in 3-4 days after stopping
- Require 3-4 days of daily dosing to reach full acid-inhibitory potential
- Hepatically metabolized (cytochrome P450); negligible renal clearance
Clinical Use in PUD:
- Heal >90% of duodenal ulcers in 4 weeks and >90% of gastric ulcers in 6-8 weeks
- Faster symptom relief and higher healing rates than H2 blockers
Adverse Effects:
- Generally well tolerated
- Long-term use: hypomagnesemia, vitamin B12 deficiency, increased risk of C. difficile infection, possible risk of bone fractures (reduced Ca²⁺ absorption)
- Rebound acid hypersecretion on abrupt withdrawal
(Katzung, 16th ed.)
2. H2-RECEPTOR ANTAGONISTS (H2 BLOCKERS)
Drugs: Cimetidine, Ranitidine, Famotidine, Nizatidine
Mechanism of Action:
- Competitive, reversible blockade of histamine H2 receptors on parietal cells
- Reduce both basal and meal-stimulated acid secretion
- Also inhibit acid secretion stimulated by gastrin and acetylcholine (since histamine is the common final mediator from ECL cells)
Clinical Use:
- Moderate PUD, NSAID-induced ulcers (when PPI not available), stress ulcer prophylaxis, nonulcer dyspepsia
- H2 blockers are second-line to PPIs; PPIs afford faster, more complete acid suppression
Adverse Effects:
- Mostly safe; adverse effects in <3% of patients: diarrhea, headache, fatigue, constipation
- Cimetidine-specific effects (not seen with other H2 blockers):
- Inhibits androgen receptors and metabolism of estradiol → gynecomastia, impotence in men; galactorrhea in women
- Mental status changes (confusion, hallucinations) in elderly/ICU patients - IV route
- Inhibits CYP450 (2C9, 2D6, 3A4) → multiple drug interactions (warfarin, phenytoin, theophylline, lidocaine)
- Cross the placenta; secreted in breast milk - avoid in pregnancy/lactation unless essential
(Katzung, 16th ed.)
3. ANTACIDS
Examples: Sodium bicarbonate, Calcium carbonate, Magnesium hydroxide (Mg(OH)₂), Aluminium hydroxide (Al(OH)₃)
Combinations: Gelusil, Maalox, Mylanta (Mg + Al combination)
Mechanism: Weak bases that neutralize HCl in the gastric lumen → raise intragastric pH
Individual agents:
| Agent | Onset | Side Effects |
|---|---|---|
| NaHCO₃ | Rapid | Belching (CO₂), metabolic alkalosis, Na⁺ load |
| CaCO₃ | Moderate | Belching, milk-alkali syndrome (with dairy) |
| Mg(OH)₂ | Moderate | Diarrhea (osmotic); avoid in renal failure |
| Al(OH)₃ | Slow | Constipation, phosphate binding; avoid in renal failure |
Drug Interactions: Antacids bind other drugs and alter pH → reduce absorption of tetracyclines, fluoroquinolones, iron, ketoconazole. Do not give within 2 hours of other drugs.
(Katzung, 16th ed.)
CLASS II: AGENTS THAT PROMOTE MUCOSAL DEFENSE
4. SUCRALFATE
Mechanism:
- Basic aluminum salt of sucrose octasulfate
- In the acidic gastric environment, polymerizes and becomes highly negatively charged
- Adheres to ulcer base (positively charged proteins exposed at ulcer crater) forming a viscous, cytoprotective barrier for up to 6 hours
- Also stimulates prostaglandin synthesis, mucus, and bicarbonate secretion
- No systemic acid suppression - works locally
Use: Duodenal ulcer (4-8 weeks); stress ulcer prophylaxis
Adverse Effects: Constipation; binds other drugs - take 2 hours apart from other medications; not suitable with PPIs or antacids (requires acidic pH for activation)
5. PROSTAGLANDIN ANALOGUES - MISOPROSTOL
Drug: Misoprostol (PGE1 analogue)
Mechanism:
- Binds prostaglandin EP3 receptors on parietal cells → inhibits adenylyl cyclase → reduces acid secretion
- Stimulates mucus and bicarbonate secretion (cytoprotection)
- Maintains mucosal blood flow
Use: Prevention of NSAID-induced ulcers (most important indication) in high-risk patients; also used as abortifacient/cervical ripener
Adverse Effects: Diarrhea, abdominal cramps (dose-dependent and often limiting); contraindicated in pregnancy (causes uterine contractions)
6. BISMUTH COMPOUNDS
Drug: Bismuth subsalicylate (Pepto-Bismol), Colloidal bismuth subcitrate (CBS)
Mechanism:
- Coats ulcer base (cytoprotective coating)
- Direct bactericidal activity against H. pylori
- Stimulates prostaglandin, mucus, and bicarbonate secretion
Use: Component of H. pylori eradication regimens (quadruple therapy); traveler's diarrhea
Adverse Effects: Black stools, black tongue (harmless); rarely neurotoxicity with excessive long-term use
H. PYLORI ERADICATION REGIMENS
This is the most important pharmacological management for H. pylori-positive PUD.
Triple Therapy (14 days) - Standard
- PPI (twice daily) + Clarithromycin 500 mg BD + Amoxicillin 1 g BD
- If penicillin allergic: Metronidazole 500 mg BD replaces amoxicillin
Quadruple Therapy (14 days) - For clarithromycin-resistant areas
(a) PPI BD + Bismuth 524 mg QID + Metronidazole 500 mg QID + Tetracycline 500 mg QID
(b) PPI BD + Amoxicillin + Clarithromycin + Metronidazole (all BD)
After completion: Continue PPI once daily for a total of 4-6 weeks to ensure complete ulcer healing.
Confirmation of eradication: Urea breath test or fecal antigen test - done 4 weeks after finishing antibiotics (stop PPI 2 weeks before testing to avoid false negatives).
(Katzung, 16th ed.)
NSAID-INDUCED ULCER MANAGEMENT
- Asymptomatic ulceration in 10-20% of frequent NSAID users
- Ulcer complications (bleeding, perforation) in 1-2% per year
- Discontinue NSAID if possible; PPI promotes faster healing than H2 blockers
- If NSAID cannot be stopped: PPI is added to continue alongside the NSAID
- For prevention in high-risk NSAID users: PPI once daily or misoprostol (less tolerated)
(Katzung, 16th ed.)
DRUG SUMMARY TABLE
| Drug Class | Example | Mechanism | Key Use |
|---|---|---|---|
| PPI | Omeprazole | Irreversible H⁺/K⁺-ATPase inhibition | 1st line PUD, GERD, H. pylori regimen |
| H2 Blocker | Ranitidine | H2 receptor competitive blockade | Mild PUD, stress ulcer prophylaxis |
| Antacid | Mg(OH)₂ + Al(OH)₃ | Neutralize HCl | Symptomatic relief |
| Sucralfate | Sucralfate | Ulcer coating, cytoprotection | Duodenal ulcer, stress ulcer prophylaxis |
| Prostaglandin | Misoprostol | ↓ acid, ↑ mucus/bicarb | NSAID ulcer prevention |
| Bismuth | Bismuth subsalicylate | Coat ulcer + anti-H. pylori | Quadruple therapy |
| Antibiotics | Clarithromycin + Amoxicillin | H. pylori eradication | Combined with PPI |
KEY PHARMACOLOGY POINTS FOR EXAM
- PPIs are prodrugs activated in the parietal cell canaliculus - must be taken before meals.
- PPIs cause irreversible inactivation of H⁺/K⁺-ATPase; full effect takes 3-4 days.
- Cimetidine is the only H2 blocker causing gynecomastia and CYP450 inhibition.
- H. pylori eradication = PPI + 2 antibiotics for 14 days (triple therapy).
- Misoprostol's primary role = prevention of NSAID-induced ulcers; not well tolerated.
- Sucralfate requires an acidic environment to work - do not combine with PPIs/antacids.
- Mg-containing antacids cause diarrhea; Al-containing cause constipation.
- Confirm H. pylori eradication with urea breath test 4 weeks after stopping antibiotics.
References: Katzung's Basic & Clinical Pharmacology, 16th ed. (Chapters 62); Goodman & Gilman's The Pharmacological Basis of Therapeutics; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.