Prune belly syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"prune belly syndrome"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Excellent - I have rich data from multiple textbook sources and two clinical images. I now have enough to write a comprehensive answer.
Prune Belly Syndrome (Eagle-Barrett Syndrome)
Definition and Classic Triad
Prune Belly Syndrome (PBS), also called Eagle-Barrett syndrome, is defined by three cardinal features:
- Absent or deficient anterior abdominal wall musculature - giving the newborn's skin a wrinkled, prune-like appearance
- Massive dilation of the urinary tract - megacystis, grossly dilated and tortuous ureters, hydronephrosis
- Bilateral cryptorchidism (intra-abdominal testes)
PBS almost exclusively affects males (~95%). Female cases (~5%) show the abdominal wall and urinary tract features but obviously lack cryptorchidism.
Clinical appearance - lax "pot belly" abdominal wall in older patients:
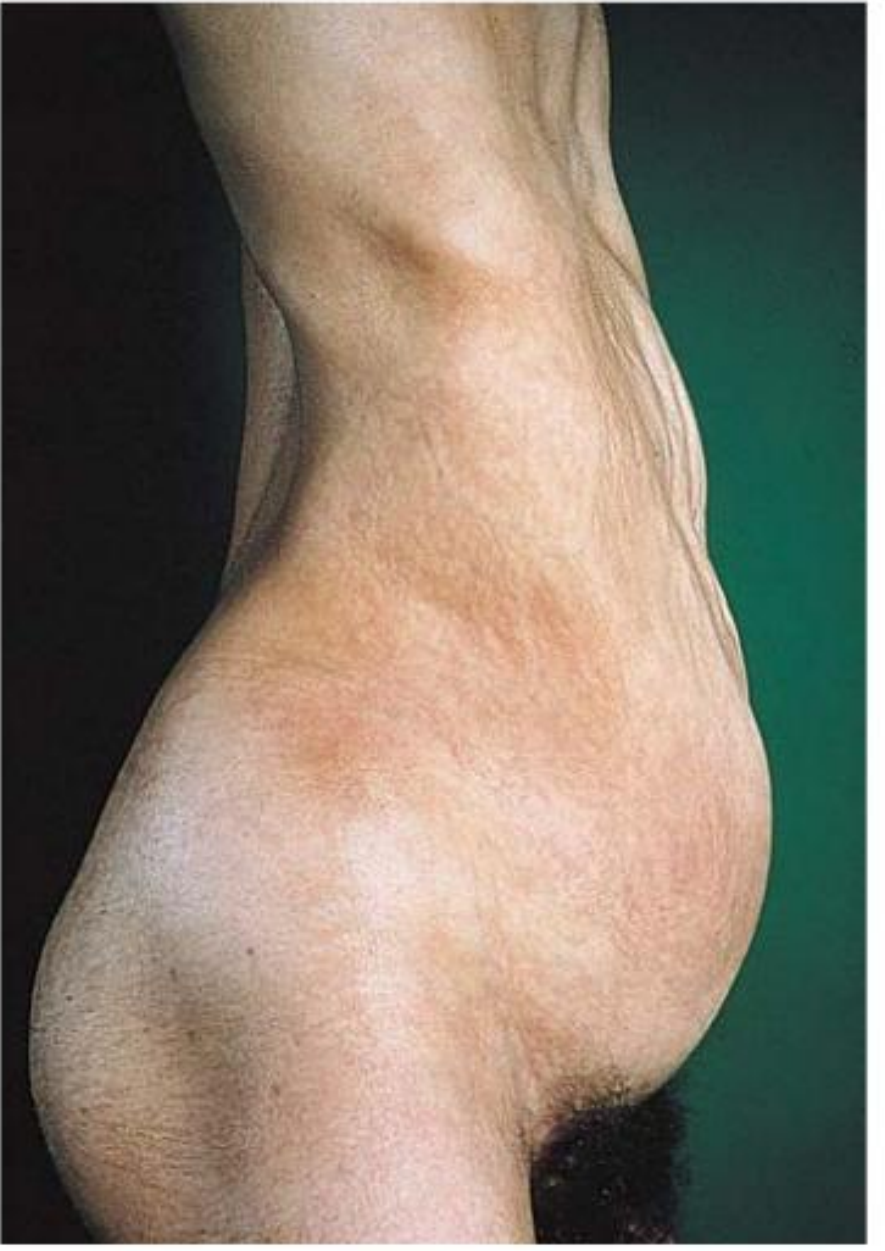
Comprehensive Clinical Nephrology, 7th Edition - Fig. 52.9: Lax abdominal musculature leading to a pot-bellied appearance, with marked thoracic cage deformity.
Epidemiology
- Incidence: 1 in 35,000 to 1 in 50,000 live births
- ~43% of affected newborns are premature
- ~20% die in the perinatal period (from pulmonary hypoplasia or renal failure)
Pathogenesis
The exact cause remains debated. Two main theories exist:
- Urethral obstruction theory: Transient or persistent fetal urethral obstruction causes massive urinary tract dilation, which in turn compresses developing abdominal mesenchyme and prevents testicular descent. Supporting evidence: an almost identical syndrome can result from urethral atresia.
- Primary mesodermal defect theory: A localized arrest of mesenchymal development occurs, supported by absent prostatic differentiation (the epithelial element in the prostate is absent or hypoplastic) and similar involvement of smooth muscle across multiple organs. This explains the non-obstructive aperistalsis of ureters.
Genetic basis: Some familial cases have been reported. Biallelic loss-of-function mutations in CHRM3 (a muscarinic acetylcholine receptor involved in parasympathetic-mediated detrusor contraction) have been identified in one family with a prune-belly-like syndrome. Ultrastructural studies of ureters show massive replacement of smooth muscle with fibrous and collagen tissue, plus absence of nerve plexuses. - Comprehensive Clinical Nephrology, 7th Edition
Genitourinary Anomalies
Kidneys
- A spectrum from normal parenchyma to severe dysplasia (Potter type II or IV)
- Dysplasia present in ~50% of cases
- Renal collecting system is characteristically dilated - though the degree of dilation does not correlate with degree of dysplasia
- Vesicoureteral reflux in 75% of cases
- Renal infection (not obstruction) poses the greatest risk to long-term renal function
Ureters
- Dilated, tortuous, and redundant
- Proximal (upper) segments are less abnormal than distal
- Histologically: lack of smooth muscle cells, increased fibrous/collagen tissue, reduced myofibrils - resulting in poor peristalsis and upper tract stasis
- Elevated collagen-to-smooth-muscle ratio especially in refluxing ureters
Bladder
- Massively distended (megacystis), often thick-walled or thin-walled
- Bladder empties poorly; true obstruction (bladder outlet obstruction) must be distinguished from functional stasis
Prostate & Urethra
- Prostate is absent or hypoplastic (epithelial element missing)
- Prostatic urethra may be dilated or atretic
- Megalourethra may coexist
Testes
- Bilateral cryptorchidism (intra-abdominal)
- Low risk of germ cell malignancy due to lack of germinal epithelium, but scrotal placement and long-term follow-up are still required
Imaging - IVU and CT urogram showing grossly dilated ureters, bilateral hydronephrosis, and absent abdominal musculature:
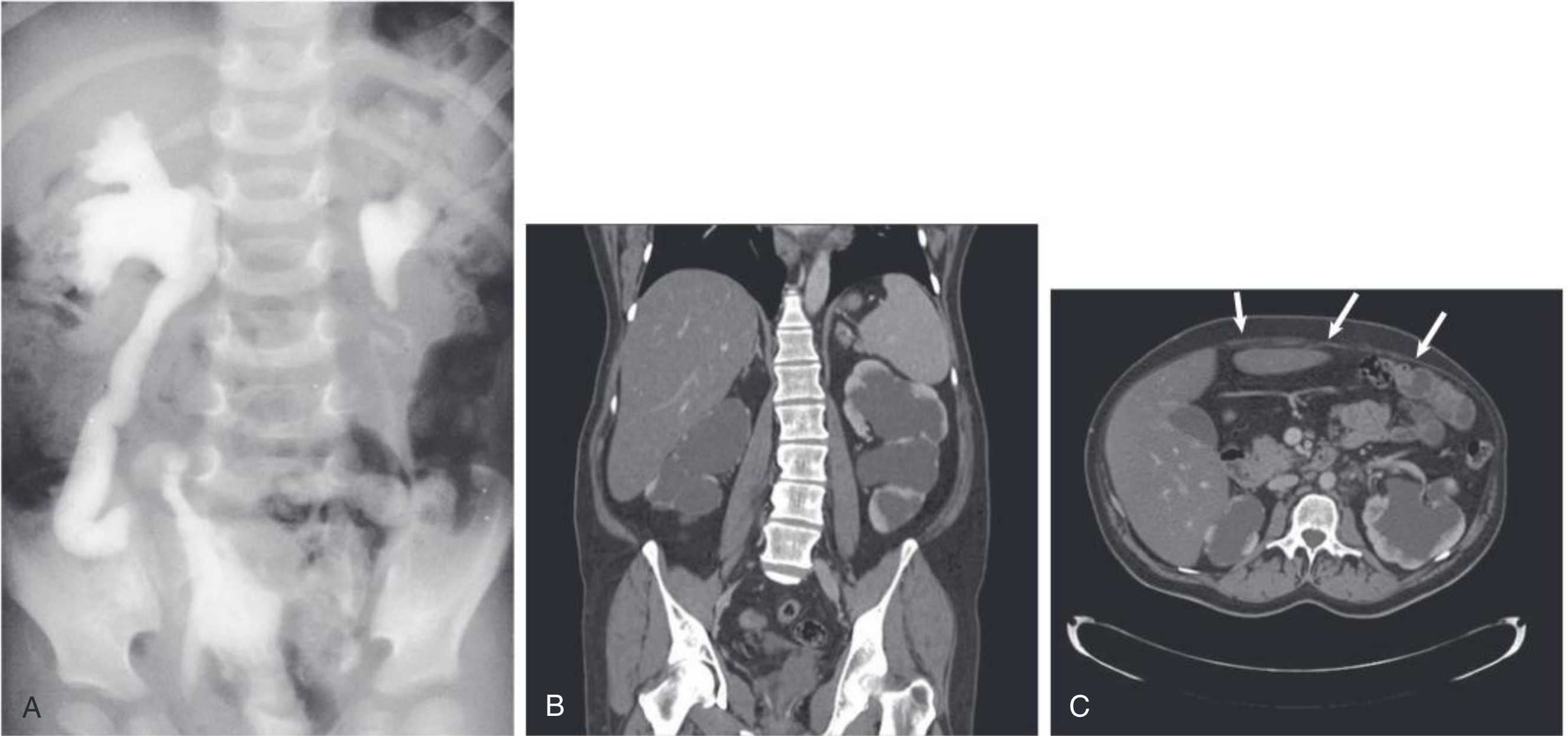
Comprehensive Clinical Nephrology, 7th Edition - Fig. 52.10: (A) IVU showing massively dilated tortuous ureters. (B) CT urogram - gross bilateral hydronephrosis. (C) CT axial - absence of anterior abdominal wall musculature (arrows).
Extragenitourinary (Associated) Abnormalities
75% of PBS patients have non-urinary tract abnormalities:
| Associated Condition | Prevalence (%) |
|---|---|
| Respiratory (pulmonary hypoplasia, pneumothorax) | 58% |
| Cardiovascular | 25% |
| Gastrointestinal (malrotation, volvulus, imperforate anus) | 24% |
| Musculoskeletal (scoliosis, hip dislocation, talipes) | 23% |
| Metabolic/endocrine | 22% |
| Prematurity | 43% |
| Sepsis/infection | 14% |
Additional features include pectus excavatum, thoracic cage deformity, and inability to sit up from a supine position in later life.
Spectrum of Disease (Woodard Classification)
Three clinical categories based on neonatal presentation:
| Category | Characteristics | Outcome |
|---|---|---|
| I (~20%) | Renal dysplasia, oligohydramnios, pulmonary hypoplasia, Potter features, often urethral atresia | Stillbirth or early neonatal death from pulmonary hypoplasia/renal failure |
| II (~20%) | Full triad, minimal or unilateral renal dysplasia, no pulmonary hypoplasia | May progress to renal failure; requires diversion and reconstruction |
| III (~60%) | Incomplete or mild triad features, mild-to-moderate uropathy, no renal dysplasia | Stable renal function, good long-term health |
Evaluation and Management
Initial (Neonatal) Management
A multidisciplinary team is required: neonatologist, nephrologist, urologist ± cardiologist and orthopedics.
- Immediate CXR - exclude pneumothorax, pneumomediastinum, pulmonary hypoplasia
- Serum creatinine, BUN, electrolytes - a baseline creatinine <0.7 mg/dL predicts adequate renal function through childhood
- Renal/bladder ultrasound once stabilized
- VCUG - to assess outlet obstruction and reflux (present in up to 70%)
- MR urography - reveals calyceal diverticula, abnormal renal pelvic anatomy, and renal dysplasia not evident on standard imaging
- Circumcision and antibiotic prophylaxis - to reduce UTI risk given urinary stasis
- Early urologic intervention only if true bladder outlet obstruction (suprapubic tube)
Long-term Urologic Management
Conservative approach (preferred for most Category III and stable Category II):
- Prophylactic antibiotics, surveillance, timed voiding
- Bowel management to improve intra-abdominal pressure
Surgical options:
- Vesicostomy - temporary diversion for bladder decompression in neonates with outlet obstruction
- Ureteral reconstruction (ureteroplasty/tapering) - for persistently dilated ureters; proximal segments are preferred as they contain more normal smooth muscle
- Abdominoplasty (Randolph/Monfort technique) - excision of the redundant abdominal wall and tightening of muscles to improve appearance, posture, bowel/bladder function
- Orchiopexy - bilateral, early (ideally by 2 years); Fowler-Stephens technique often needed for high intra-abdominal testes
- Reduction cystoplasty - for massive bladder (controversial benefit)
- Early total reconstruction (Woodard-Parrott) - simultaneous abdominoplasty + ureteral reconstruction + orchiopexy at one operation
Prenatal intervention is rarely justified - only in urethral atresia with progressive oligohydramnios threatening lung development.
Prognosis
- Renal outcome is determined primarily by the degree of renal dysplasia at birth, not by the anatomic severity of the urinary tract dilation
- ~60% of patients (Category III) maintain stable renal function long-term
- Major causes of morbidity/mortality: pulmonary hypoplasia (early), recurrent UTIs, and progressive chronic kidney disease
- Fertility is almost universally impaired due to cryptorchidism and prostatic hypoplasia; a 2024 scoping review (PMID 38267308) confirmed very poor fertility prospects even after orchiopexy
Sources:
- Campbell Walsh Wein Urology, 3-Volume Set (Chapter 32 - primary reference)
- Comprehensive Clinical Nephrology, 7th Edition (Chapter 52)
- The Developing Human: Clinically Oriented Embryology (Chapter 15)
- Smith and Tanagho's General Urology, 19th Edition (Chapter 22)
- Recent review: Conegundes et al. (2025) "Prune-belly Syndrome: An Update." Curr Pediatr Rev. PMID 38879764
This is a shared conversation. Sign in to Orris to start your own chat.