Flow volume loop. Differences from a healthy patient. Restrictive. And obstructive. Lung disease patient.
Reading File
Finding Sources
Finding Sources
Searching the Web
flow volume loop normal restrictive obstructive differences diagram explained
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have excellent textbook diagrams and content. Here is a thorough breakdown:
Flow-Volume Loop: Normal vs. Obstructive vs. Restrictive
What Is a Flow-Volume Loop?
A flow-volume loop (FVL) is a graphical plot of airflow (y-axis, L/s) against lung volume (x-axis, L) during a maximal forced expiration followed immediately by a maximal forced inspiration. The upper half of the loop = expiration, the lower half = inspiration.
Key landmarks on a normal loop:
- Peak expiratory flow (PEF) - the sharp early peak, reflects large airway patency; it is effort-dependent
- FEF25-75% (mid-expiratory flows, V50/V25) - the descending limb after the peak; this is effort-independent and reflects small airway/peripheral airway function
- FVC - total width of the loop along the volume axis
- RV - residual volume at the end of expiration (the loop's rightmost point)
- Inspiratory limb - smooth, symmetric, roughly semicircular
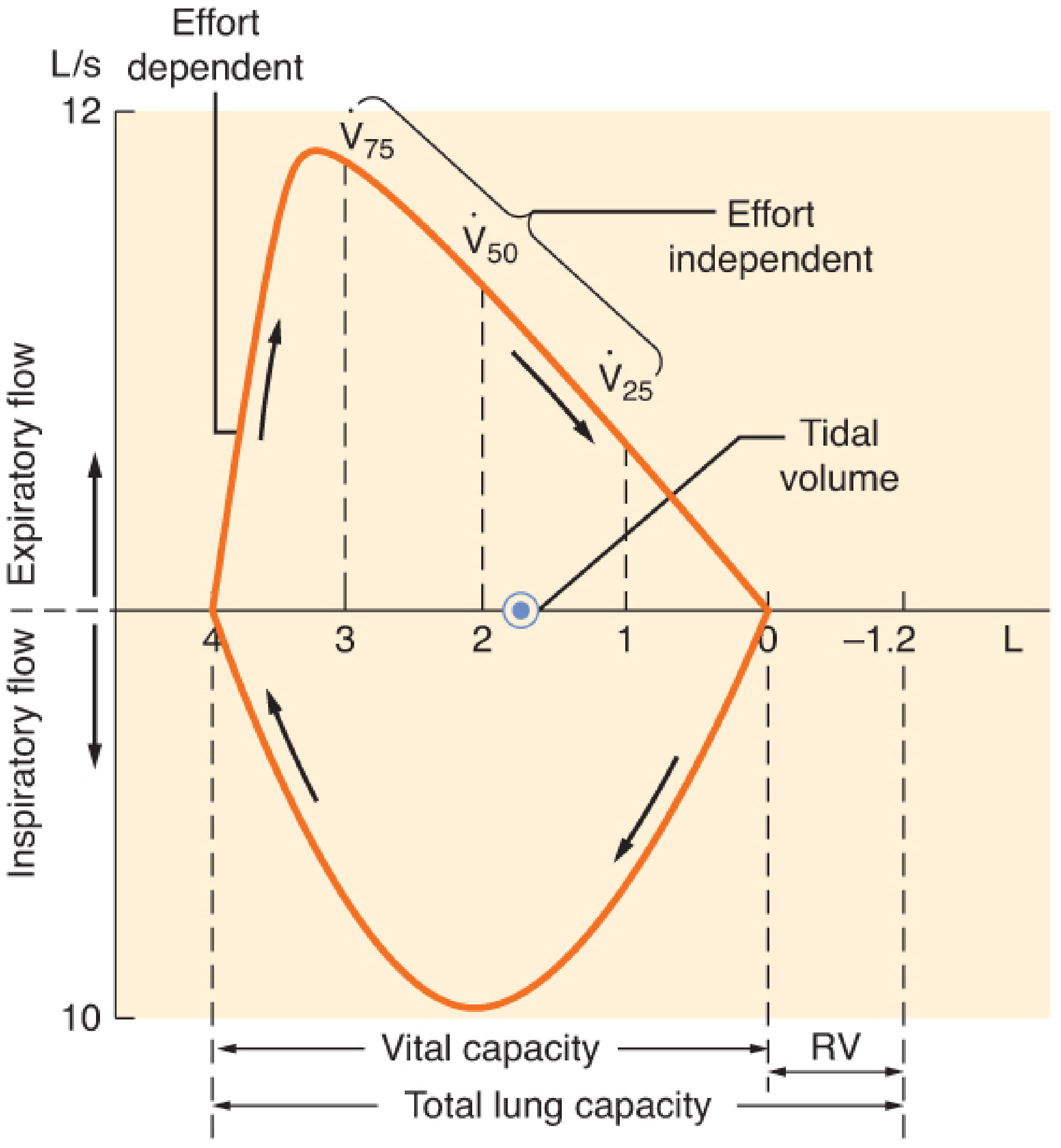
Normal FVL - Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
Side-by-Side Comparison
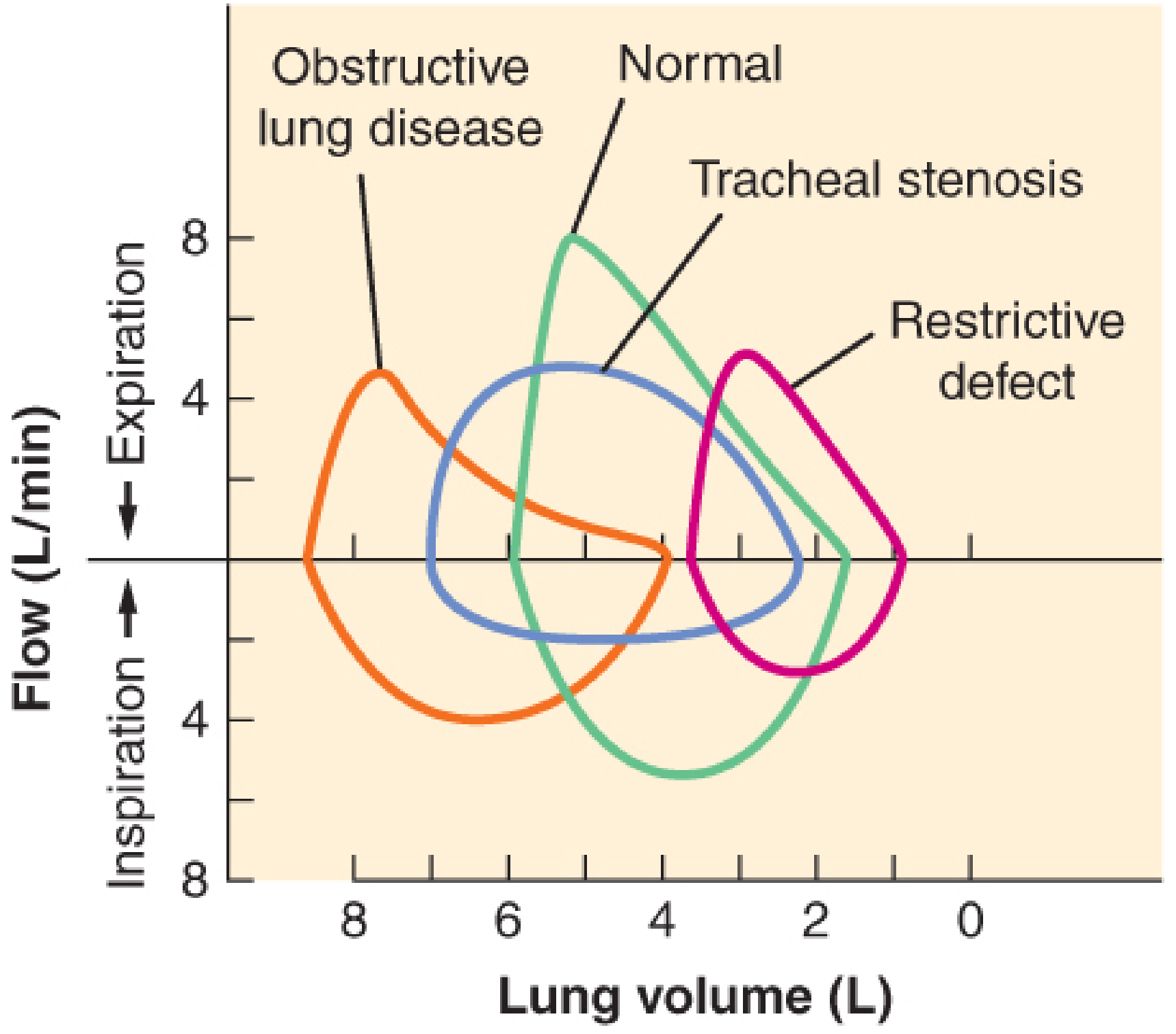
Flow-volume loops compared across disease states - Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e

Normal Pattern
| Feature | Normal |
|---|---|
| Shape | Wide, triangular expiratory limb; smooth symmetric inspiratory arc |
| Peak expiratory flow | Normal (effort-dependent) |
| Expiratory descending limb | Straight to mildly convex (bowing outward) |
| FVC | Normal |
| FEV1/FVC | ≥ 0.70 (≥ 70%) |
| TLC | Normal |
| RV | Normal |
Obstructive Pattern (COPD, Asthma, Emphysema, Bronchiectasis)
The hallmark is increased airway resistance - air cannot leave quickly.
Shape on the FVL:
- "Scooped" or "coved" expiratory limb - the descending portion bows inward (concave upward) instead of being straight. This is the most recognizable feature.
- Reduced peak expiratory flow - the early peak is blunted
- FEF25-75% markedly reduced - the effort-independent portion reflects small airway obstruction
- Loop is shifted to the LEFT (toward higher lung volumes) - because TLC increases due to air trapping, and RV is elevated
- Wider loop on the volume axis - the loop extends further left because RV is increased (hyperinflation)
- Inspiratory limb is relatively preserved (unless severe)
Spirometry numbers:
| Value | Direction |
|---|---|
| FEV1 | ↓↓ |
| FVC | ↓ or normal |
| FEV1/FVC | ↓ (< 0.70) - defining criterion |
| TLC | ↑ (hyperinflation) |
| RV | ↑↑ (air trapping) |
| FEF25-75% | ↓↓ |
Why the scoop? In obstructive disease, dynamic airway collapse during forced expiration causes premature small airway closure. At lower lung volumes (reduced elastic recoil + narrowed airways), flow drops off faster than normal, pulling the curve inward.
Restrictive Pattern (Pulmonary Fibrosis, Scoliosis, Neuromuscular Disease, Pleural Disease)
The hallmark is reduced lung volumes - the lungs cannot fully expand, but the airways themselves are normal.
Shape on the FVL:
- Smaller overall loop - the entire loop is narrow and shifted to the RIGHT (toward lower volumes)
- Shape is preserved - the expiratory limb remains straight/convex (no scooping), because airway resistance is normal
- Reduced peak expiratory flow - but proportional to the reduced lung volumes
- Normal-looking curve, just miniaturized
Spirometry numbers:
| Value | Direction |
|---|---|
| FEV1 | ↓ |
| FVC | ↓↓ |
| FEV1/FVC | Normal or ↑ (> 0.70-0.80) - airway resistance intact |
| TLC | ↓ - confirming criterion |
| RV | ↓ or normal |
| FEF25-75% | Normal or proportionally reduced |
Why preserved shape? Because the airways are patent and resistance is normal. The lungs simply cannot fill or empty as much total volume. The shape of the flow-rate curve relative to its volume is normal; there is just less volume to work with.
Key Distinguishing Summary
| Feature | Normal | Obstructive | Restrictive |
|---|---|---|---|
| Expiratory limb shape | Straight/convex out | Scooped inward (concave) | Straight/convex - preserved shape |
| Loop size | Normal | Wide/large (air trapping) | Small/narrow |
| Loop position | Central | Shifted left (high volumes) | Shifted right (low volumes) |
| FEV1/FVC | ≥ 0.70 | < 0.70 | Normal or high |
| TLC | Normal | ↑ | ↓ |
| RV | Normal | ↑↑ | ↓ or normal |
| Inspiratory limb | Normal arc | Relatively preserved | Smaller arc, normal shape |
A Note on Mixed Disease
Some patients have both obstructive and restrictive components simultaneously (e.g., COPD + obesity or COPD + fibrosis). The FVL in those cases shows a scooped expiratory limb (obstructive signature) combined with reduced total loop size. TLC measurement is necessary to confirm restriction when FEV1/FVC is already low.
Bonus: Upper Airway Obstruction Patterns
The FVL is especially useful for detecting large airway (tracheal) problems:
- Fixed obstruction (e.g., tracheal stenosis): Both expiratory AND inspiratory limbs are flat - a box-shaped loop
- Variable extrathoracic obstruction (e.g., vocal cord paralysis): Only the inspiratory limb is flattened
- Variable intrathoracic obstruction (e.g., tracheomalacia): Only the expiratory limb is flattened
Sources: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e; Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.