Mallampati grading Methods of airway assessment Bedside predictors of difficult intubation POGO score Cormack-Lehane grading Intubation Difficulty Score
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to write a detailed, well-structured response. Let me compile everything.
Airway Assessment: A Comprehensive Reference
1. Mallampati Grading (Modified)
Originally described by Mallampati in 1983, then modified by Samson and Young to add a Class IV. The test is performed with the patient seated upright, head neutral, mouth maximally open, tongue protruded maximally, and without phonation.
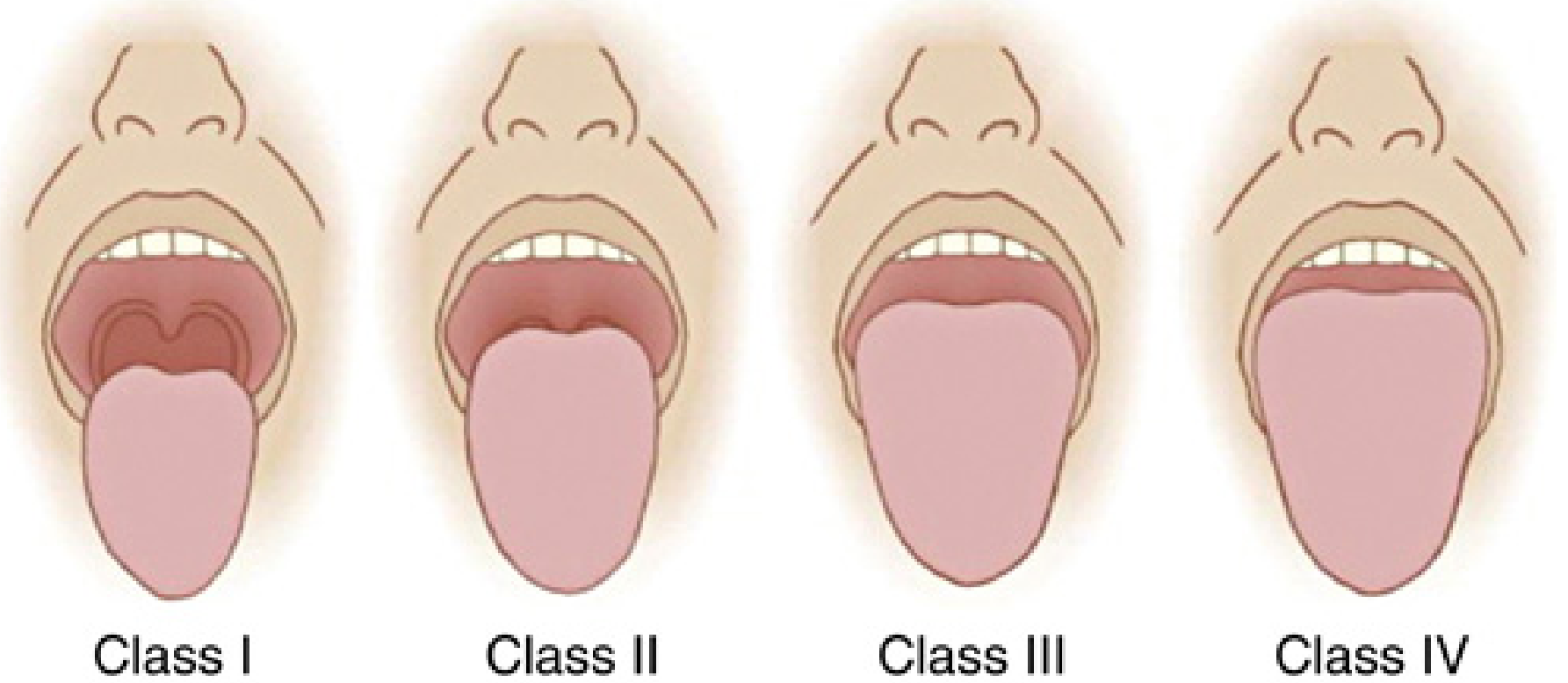
| Class | Structures Visible |
|---|---|
| I | Soft palate, fauces, uvula, tonsillar pillars |
| II | Soft palate, fauces, base of uvula (uvula partially obscured by tongue) |
| III | Soft palate only; base of uvula not seen |
| IV | Hard palate only visible; soft palate not seen |
Key points:
- Higher Mallampati class = larger tongue relative to the oropharyngeal space = poorer direct laryngoscopy view
- Class III/IV predicts difficult direct laryngoscopy
- As a stand-alone test it has poor predictive value (low sensitivity and specificity); it is most useful in combination with other predictors
- Some studies support obtaining the score with the tongue protruded vs. in neutral; phonation during the test can falsely lower the class
- Miller's Anesthesia, 10e; Sabiston Textbook of Surgery
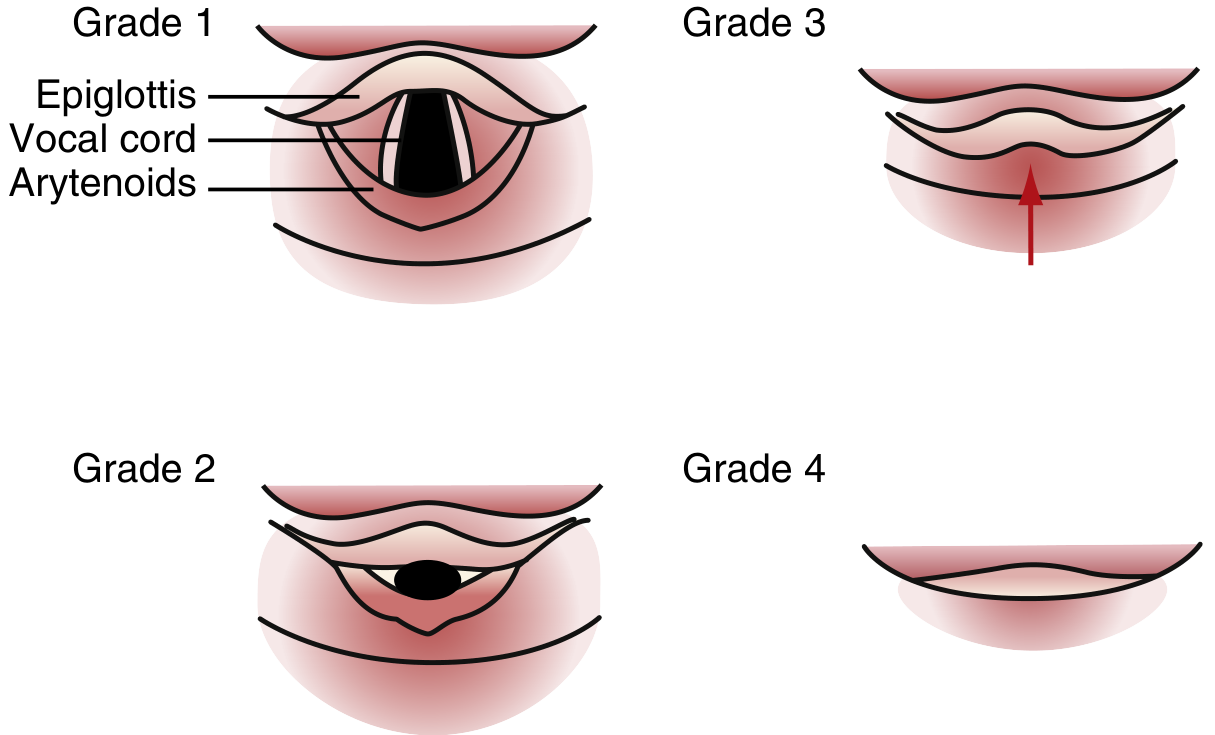
2. Cormack-Lehane (CL) Grading
Developed by Cormack and Lehane in 1984 to describe the laryngoscopic view obtained during direct laryngoscopy. It is the most widely used intraoperative grading system. The modified version (by Yentis and Lee) subdivides Grade 2.
| Grade | View | Clinical Significance |
|---|---|---|
| 1 | Full glottis visualized; vocal cords, arytenoids visible | Easy intubation; ~100% first-pass success |
| 2a | Partial cords and full arytenoids seen | Manageable; low failure rate (<5%) |
| 2b | Only arytenoids visible (no cords) | Significantly more difficult; failure in up to 2/3 of cases |
| 3 | Only epiglottis visible | Difficult intubation; use bougie or VL |
| 4 | Not even the epiglottis visible | Very difficult; alternative technique mandatory |
Epidemiology:
- Grade 3 or 4: found in 1.5-8.5% of adult laryngoscopies
- Grade 4: < 1% of elective patients
- Grade 3: < 5% of elective patients
- Grade 2 overall: 10-30% of patients
Limitations: Subject to inter-rater variability; this led to the modified Grade 2 (2a/2b) subdivision.
- Miller's Anesthesia, 10e; Rosen's Emergency Medicine; Fishman's Pulmonary Diseases
3. POGO Score (Percentage of Glottic Opening)
Introduced as a continuous, more descriptive alternative to the Cormack-Lehane system.
Definition: The percentage (0-100%) of the glottic aperture (from the anterior commissure to the interarytenoid notch) that is visualized during laryngoscopy.
| POGO Score | Interpretation |
|---|---|
| 100% | Full glottic opening seen (= CL Grade 1) |
| 1-99% | Partial view |
| 0% | No glottis visible (= CL Grade 3/4) |
Advantages over CL:
- Continuous numerical scale reduces ambiguity of Grade 2 (2a vs. 2b)
- Validated in studies as a reliable metric
- Better intrarater reliability
Disadvantages:
- Not widely adopted in clinical practice despite validation
- Requires estimation of a percentage, which can still be subjective
- Rosen's Emergency Medicine; Fishman's Pulmonary Diseases, 2-Volume Set
4. Methods of Airway Assessment (Bedside Predictors)
A complete preintubation assessment evaluates four domains: (1) direct laryngoscopy/intubation, (2) bag-mask ventilation, (3) extraglottic device placement, (4) cricothyrotomy.
A. LEMON - Difficult Direct Laryngoscopy
| Letter | Parameter | Detail |
|---|---|---|
| L | Look externally | General gestalt: facial trauma, burns, blood, deformity, obesity, neck pathology |
| E | Evaluate 3-3-2 rule | 3 fingers between incisors (mouth opening); 3 fingers from chin to hyoid (submandibular space); 2 fingers from laryngeal prominence to chin (laryngeal position) |
| M | Mallampati score | Class III or IV predicts difficulty |
| O | Obstruction / Obesity | Airway mass, epiglottitis, peritonsillar abscess, obesity (BMI > 35) |
| N | Neck mobility | Limited extension (rheumatoid arthritis, ankylosing spondylitis, halo/collar) |
3-3-2 Rule details:
- < 3 fingers mouth opening = inadequate mouth opening
- < 3 fingers mentum to hyoid = inadequate submandibular space (tongue cannot be displaced)
- < 2 fingers from laryngeal prominence to chin = high, anterior larynx (worst predictor)
LEMON has reasonable sensitivity and high negative predictive value for difficult direct laryngoscopy.
B. ROMAN - Difficult Bag-Mask Ventilation
| Letter | Parameter |
|---|---|
| R | Resistance / Radiation - Intrinsic lung disease (asthma, COPD, ARDS), prior head-neck radiation |
| O | Obstruction / Obesity / OSA - Supraglottic obstruction; obesity causes redundant airway tissues and reduced FRC |
| M | Mallampati / Mask seal / Male - High class, beard or facial trauma (poor seal), male sex |
| A | Age > 55 years |
| N | No teeth (edentulous) - Dentures should be kept in for ventilation, removed for intubation |
Difficult BMV is found in ~1/50 general anesthesia patients. Impossible BMV: ~1/600. Difficult BMV makes difficult intubation 4x more likely and impossible intubation 12x more likely.
C. RODS - Difficult Extraglottic Device (EGD/LMA) Placement
| Letter | Parameter |
|---|---|
| R | Restricted mouth opening OR Resistance to ventilation |
| O | Obstruction / Obesity / OSA |
| D | Distorted anatomy |
| S | Short thyromental distance |
D. SMART - Difficult Cricothyrotomy
| Letter | Parameter |
|---|---|
| S | Surgery (prior neck surgery/scarring) |
| M | Mass (hematoma, abscess, tumor) |
| A | Access/anatomy problems (obesity, edema) |
| R | Radiation (prior neck radiation - fibrosis) |
| T | Tumor |
E. Additional Individual Bedside Predictors (Miller's Box 40.3)
| Predictor | Abnormal Finding |
|---|---|
| Upper incisors | Long/prominent (buck teeth) |
| Overbite | Prominent; inability to prorate mandible |
| Mouth opening (interincisor gap) | < 3 cm (2 fingerbreadths); some use < 4 cm |
| Mallampati class | III or IV |
| Palate | High, arched |
| Thyromental distance (TMD) | < 6 cm (< 3 fingerbreadths) |
| Neck circumference | > 43 cm (17 inches) - stronger predictor than BMI |
| Neck mobility | Limited extension/flexion |
| Mandibular prognathism (Upper Lip Bite Test) | Cannot bite upper vermillion border with lower incisors |
| Sternomental distance | < 12.5 cm |
Best combination: Mallampati + thyromental distance has the most evidence for predicting difficult intubation.
- Miller's Anesthesia 10e; Sabiston Textbook of Surgery; Rosen's Emergency Medicine
5. Intubation Difficulty Scale (IDS)
Introduced by Adnet et al. (1997). A numeric, post-hoc scoring system that quantifies the overall difficulty of an intubation after it has been completed. Useful for documentation, research, and audit.
IDS Components (7 variables):
| Variable (N) | Score |
|---|---|
| N1 - Number of additional intubation attempts beyond the first | Each attempt = +1 |
| N2 - Number of additional operators beyond the first | Each extra operator = +1 |
| N3 - Number of alternative techniques used | Each technique = +1 |
| N4 - Cormack-Lehane grade minus 1 | Grade 1 = 0; Grade 2 = 1; Grade 3 = 2; Grade 4 = 3 |
| N5 - Lifting force required | Normal = 0; Increased = 1 |
| N6 - External laryngeal manipulation (BURP/backward-upward-rightward pressure) | Not needed = 0; Needed = 1 |
| N7 - Vocal cord position | Abducted (open) = 0; Adducted (closed) = 1 |
IDS = N1 + N2 + N3 + N4 + N5 + N6 + N7
Interpretation:
| Score | Intubation |
|---|---|
| 0 | Ideal (no difficulty) |
| 1-5 | Slight difficulty |
| > 5 | Moderate to major difficulty |
Key uses:
- Standardized documentation in the medical record after intubation
- Research comparison across studies and institutions
- Quality audit of difficult airway management
- Miller's Anesthesia, 10e (citing Adnet et al., Anesthesiology, 1997)
Summary Table: Scoring Systems at a Glance
| System | Purpose | Timing | Scale |
|---|---|---|---|
| Mallampati (modified) | Predict DL difficulty | Pre-intubation | I - IV |
| LEMON | Predict DL difficulty (ED/emergency) | Pre-intubation | Mnemonic |
| ROMAN | Predict difficult BMV | Pre-intubation | Mnemonic |
| RODS | Predict difficult EGD | Pre-intubation | Mnemonic |
| SMART | Predict difficult cricothyrotomy | Pre-intubation | Mnemonic |
| Cormack-Lehane | Grade actual laryngoscopic view | Intra-procedure | I - IV (+ 2a/2b) |
| POGO | Grade actual glottic view (continuous) | Intra-procedure | 0-100% |
| IDS | Quantify overall intubation difficulty | Post-intubation | 0 - ∞ (>5 = difficult) |
Clinical Pearl: No single predictor reliably identifies all difficult airways. The ASA and most guidelines recommend a multiparameter assessment combining at least Mallampati class, mouth opening, thyromental distance, neck mobility, and overall external inspection. A reassuring bedside assessment does not guarantee an easy intubation - always be prepared for unexpected difficulty. - Rosen's Emergency Medicine; Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.