Give me detailed explanation about cataract
Reading File
Finding Sources
Searching PubMed
cataract pathogenesis classification treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive response. Let me compile the full answer:
Cataract - Detailed Explanation
1. Definition
A cataract is an opacification of the crystalline lens of the eye. It is the commonest cause of reversible visual disability in the world, and cataract surgery (phacoemulsification with intraocular lens implantation) is the most frequently performed surgical procedure globally.
- Kanski's Clinical Ophthalmology, 10th ed.
2. Anatomy of the Lens
Understanding cataract begins with lens anatomy:
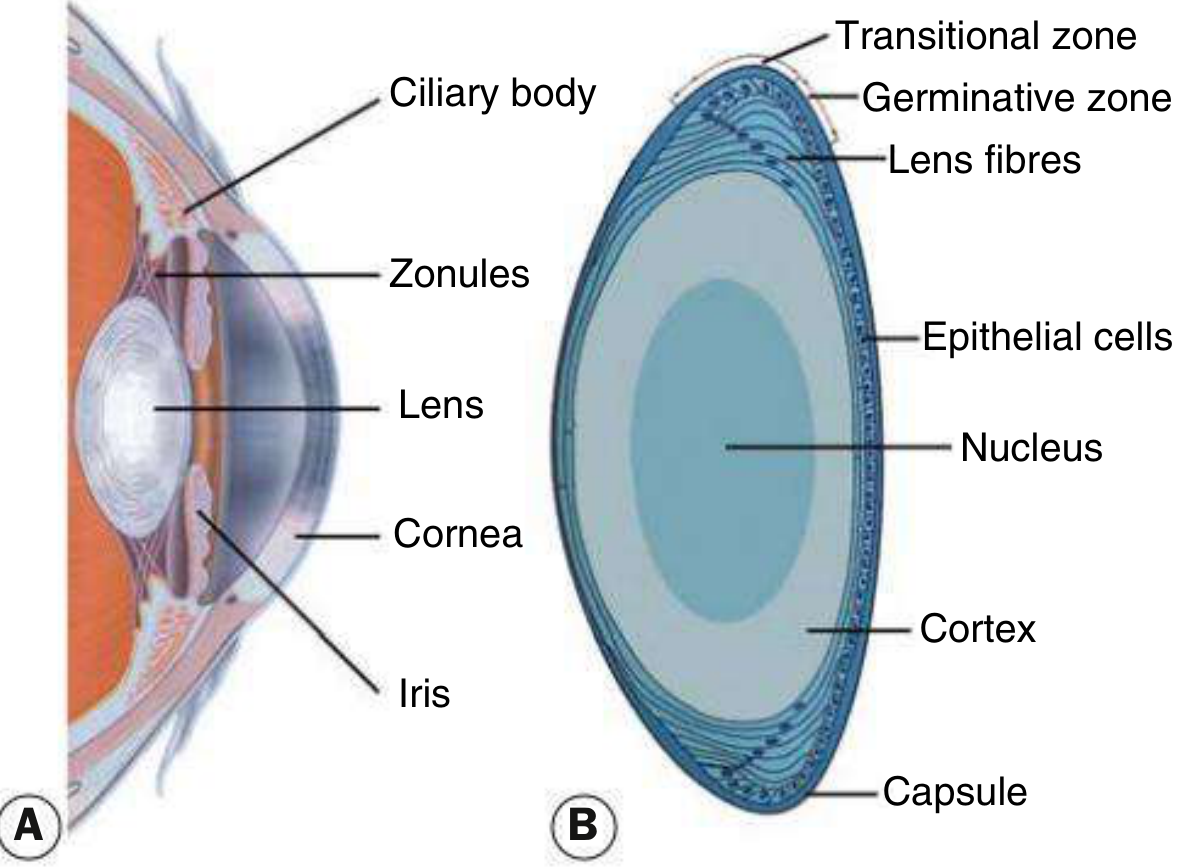
Fig. 10.1 - Cross-sectional anatomy of the anterior segment of the eye (A) and histological features of the lens in cross section (B). - Kanski's Clinical Ophthalmology
| Structure | Function |
|---|---|
| Capsule | Acellular membrane enclosing all lens material |
| Epithelial cells | Cuboid cells under the anterior capsule; in the germinative zone they continuously divide and differentiate into lens fibers |
| Cortex | Surrounding cortical material made of younger lens fibers |
| Nucleus | Central, older, compressed lens fibers |
| Zonules | Hold the lens in position from the ciliary body |
The lens doubles in volume between birth and age 70 as new fiber cells are continuously laid down. Older fibers cannot be desquamated and are compressed into the nucleus. At birth the lens is completely transparent and pliable.
3. Epidemiology and Risk Factors
- Cataract is the leading cause of reversible blindness worldwide
- Prevalence increases sharply with age; most cataracts are age-related
- Risk factors include:
- Age (most important)
- UV-B radiation exposure
- Smoking and alcohol
- Diabetes mellitus
- Corticosteroid use (systemic or topical)
- Trauma
- Uveitis/chronic inflammation
- High myopia
- Ionizing radiation
- Nutritional deficiencies
- Congenital infections (rubella, toxoplasmosis, CMV)
- Metabolic disorders (galactosaemia, Lowe syndrome)
4. Symptoms
The effect on vision depends on the type, density, and position of the opacity:
- Gradual, painless loss of vision - the hallmark symptom
- Glare - particularly from headlights at night (worst with posterior subcapsular cataract)
- Monocular diplopia or polyopia
- Frequent changes in spectacle prescription
- Acquired myopia ("second sight") - nuclear sclerosis increases the refractive index, allowing some elderly patients to read without glasses temporarily
- Dull colors/reduced contrast
- Difficulty in low-light conditions and poor night vision
- Symptoms tend to develop slowly; patients are often unaware of early changes
5. Classification
5.1 Acquired Cataract
A. Age-Related Cataract (Most Common)
There are three main morphological subtypes:
i. Posterior Subcapsular (PSC) Cataract
- Located just in front of the posterior capsule
- Has a granular or plaque-like appearance on oblique slit lamp examination
- Appears black and vacuolated on retroillumination - the vacuoles are swollen migratory lens epithelial cells (Bladder/Wedl cells)
- Causes profound visual symptoms relative to its size, due to its location at the nodal point of the eye
- Characteristic glare from oncoming headlights; symptoms worsen with miosis (in bright light and near tasks)
ii. Nuclear Sclerotic Cataract
- An exaggeration of normal ageing
- Characterized by a yellowish hue due to deposition of urochrome pigment; advanced cases appear brown ("brunescent") or even black
- Best assessed with oblique slit lamp beam
- Often associated with myopic shift ("second sight of the aged")
- Retroillumination shows a good red reflex with subtle nucleus-cortex distinction
iii. Cortical Cataract
- May involve anterior, posterior, or equatorial cortex
- Starts as clefts and vacuoles between lens fibres due to cortical hydration
- Results in cuneiform (wedge-shaped) or radial spoke-like opacities; often begins in the inferonasal quadrant
- Glare is a common symptom
iv. Christmas Tree Cataract
- Uncommon; characterized by polychromatic needle-like formations in the deep cortex and nucleus
B. Cataract in Systemic Disease
| Disease | Cataract Type |
|---|---|
| Diabetes mellitus | Snowflake/cortical, premature nuclear sclerosis |
| Hypocalcaemia/hypoparathyroidism | Punctate or lamellar opacities |
| Myotonic dystrophy | "Polychromatic" (Christmas tree) cataract |
| Wilson's disease | "Sunflower" anterior subcapsular cataract |
| Atopic dermatitis | Anterior or posterior subcapsular |
| Steroids (systemic/topical) | Posterior subcapsular cataract |
C. Secondary (Complicated) Cataract
Develops as a result of other primary ocular disease:
- Chronic anterior uveitis - most common cause; earliest finding is polychromatic lustre at the posterior pole; progresses with inflammation and posterior synechiae
- Acute angle closure glaucoma - causes small anterior grey-white subcapsular opacities (glaukomflecken) - focal infarcts of lens epithelium, pathognomonic of previous acute angle closure
- High myopia - associated with posterior subcapsular opacity and early nuclear sclerosis
- Hereditary fundus dystrophies (retinitis pigmentosa, Leber congenital amaurosis, gyrate atrophy, Stickler syndrome) - usually associated with posterior subcapsular opacity
D. Traumatic Cataract
- Results from blunt or penetrating ocular trauma
- Rosette-shaped opacity at the anterior or posterior pole is characteristic of blunt (concussion) trauma
- Penetrating injuries cause rapid cortical opacification at the site of capsular rupture
- Vossius ring - a ring imprint of iris pigment on the anterior lens following blunt trauma
- Electric and lightning shock can produce anterior and posterior subcapsular opacities
5.2 Cataract Maturity (Morphological Stage)
| Stage | Features |
|---|---|
| Immature | Lens partially opaque; some cortex remains clear |
| Mature | Lens totally opaque; no red reflex; white pupil (leukocoria) |
| Hypermature (Morgagnian) | Liquefied cortex; nucleus sinks inferiorly; wrinkled capsule |
| Intumescent | Swollen lens due to cortical hydration; risk of phacomorphic glaucoma |
5.3 Congenital Cataract
Occurs in approximately 3 in 10,000 live births.
Aetiology:
- One-third associated with systemic disease
- One-third inherited (autosomal dominant most common)
- One-third unknown cause
- Two-thirds bilateral; one-third unilateral (usually sporadic)
Associated Metabolic Disorders:
| Disorder | Cataract Feature |
|---|---|
| Galactosaemia (GALT deficiency, AR) | "Oil droplet" opacity; develops within first days/weeks; may reverse with galactose exclusion |
| Lowe (oculocerebrorenal) syndrome (X-linked recessive, OCRL1) | Cataract universal; also microphakia; congenital glaucoma in ~50% |
| Mannosidosis (AR, alpha-mannosidase deficiency) | Spoke-like posterior cortical opacities; corneal clouding |
| Hypo/pseudohypoparathyroidism | Lamellar/punctate opacities |
| Hyperglycaemia/hypoglycaemia | Various opacities |
Associated Intrauterine Infections (TORCH):
- Rubella - pearly nuclear or diffuse cataract in ~15%; occurs first trimester
- Toxoplasmosis - less commonly causes isolated cataract; mostly retinal disease
- CMV, Varicella - rare causes
Inherited Congenital Cataract Patterns:
- Autosomal dominant - most common
- Chromosomal abnormalities (Trisomy 21 [Down], Trisomy 18, Turner, etc.)
6. Pathogenesis / Mechanism of Opacification
The lens relies on active metabolic processes to maintain transparency:
- The lens epithelium maintains ionic balance via Na+/K+ ATPase pumps
- Oxidative stress (UV radiation, free radicals) damages lens proteins and epithelial cells
- Crystallin proteins (alpha, beta, gamma) are the main structural proteins; their aggregation leads to light scattering
- In nuclear cataract: compression of lens fibers + cross-linking/aggregation of crystallins + deposition of urochrome pigment
- In cortical cataract: disruption of lens fiber membranes leads to hydration, ion imbalance, and protein precipitation
- In PSC cataract: fibrous metaplasia and migration of lens epithelial cells to the posterior pole
Key biochemical mechanisms:
- Polyol pathway (sorbitol accumulation in diabetes) - osmotic damage to lens fibers
- Protein glycosylation (advanced glycation end products)
- Oxidative damage to glutathione-dependent antioxidant systems
- UV-B photochemical damage
7. Clinical Evaluation
History: onset, progression, associated symptoms (glare, diplopia, color change), systemic diseases, medications (steroids), trauma, family history
Examination:
- Visual acuity - Snellen chart; near and distance
- Pupil reflexes - rule out afferent defect (suggests retinal/optic nerve co-pathology)
- Slit lamp examination - direct illumination, retroillumination, grading (LOCS system)
- Red reflex - direct ophthalmoscopy; absent/reduced in dense cataract
- Fundal examination - assess retina before planning surgery
- Biometry - A-scan or IOL Master for axial length; keratometry for corneal curvature (needed to calculate IOL power)
- Specular microscopy - corneal endothelial cell count if Fuchs' dystrophy suspected
- Visual potential tests - entoptic phenomena, laser interferometry
Grading system: The LOCS (Lens Opacities Classification System) III grades nuclear color/opalescence, cortical opacity, and posterior subcapsular opacity.
8. Management
8.1 Conservative (No Medical Cure)
- There is no medical treatment to prevent development or progression of cataract
- Optimizing refraction (glasses/contact lenses) may help in early stages
- Avoidance of risk factors (UV protection, smoking cessation, diabetes control)
- Mydriatic drops may temporarily improve vision in PSC cataract (by dilating around the opacity)
8.2 Surgical Management
Surgery is elective and is indicated when decreased vision sufficiently interferes with the patient's lifestyle/daily activities.
A. Phacoemulsification (Standard of Care)
The gold standard in high-income countries and most regional centers worldwide.
Steps:
- Clear corneal or limbal incision (2.2-2.8 mm), self-sealing
- Continuous curvilinear capsulorhexis (CCC) - circular opening in anterior capsule
- Hydrodissection - fluid injected between cortex and capsule to free the nucleus
- Phacoemulsification - ultrasonic energy (40,000 Hz) emulsifies and aspirates the nucleus via a phaco tip; irrigation/aspiration removes remaining cortex
- IOL implantation - foldable lens inserted through the small incision into the capsular bag
Key technical considerations:
- Phacodynamics: bottle height, aspiration flow rate (AFR), vacuum levels, and pump type (peristaltic or Venturi) are calibrated per case
- Post-occlusion surge - sudden increase in outflow when phaco tip occlusion breaks; suppressed by modern machines to avoid capsular rupture
B. Manual Small-Incision Cataract Surgery (MSICS)
- Used in high-volume, resource-limited settings for dense cataracts
- Self-sealing sclerocorneal tunnel incision
- Manual nucleus expression; no expensive phaco equipment needed
- Visual outcomes comparable to phacoemulsification
C. Extracapsular Cataract Extraction (ECCE)
- Large 8-10 mm incision with nucleus expression; now largely replaced by phacoemulsification in developed settings
- Still used for very dense (brunescent/black) cataracts
D. Intracapsular Cataract Extraction (ICCE)
- Historical; entire lens with capsule removed using cryoprobe; no longer routinely performed
E. Femtosecond Laser-Assisted Cataract Surgery (FLACS)
- Laser creates the incisions, capsulorhexis, and nucleus fragmentation
- Evidence shows outcomes comparable to standard phacoemulsification (Goldman-Cecil Medicine)
8.3 Intraocular Lenses (IOL)
| IOL Type | Notes |
|---|---|
| Monofocal | Single focal point (distance or near); most common |
| Toric | Corrects astigmatism |
| Multifocal/EDOF | Multiple focal zones; reduces spectacle dependence |
| Accommodating | Attempts to mimic natural accommodation |
IOLs are calculated using the SRK/T, Haigis, Barrett Universal II or similar formulas based on axial length and corneal curvature.
8.4 Anaesthesia Options
- Topical (drops only) - most common; no injection required
- Sub-Tenon's - periocular injection; good akinesia
- Peribulbar/retrobulbar - block techniques; more akinesia
- General anaesthesia - for children or patients unable to cooperate
9. Complications of Cataract Surgery
Intraoperative
- Posterior capsular rupture with vitreous loss (~1% with experienced surgeons)
- Zonular dehiscence
- Dropped nucleus into vitreous (~0.2%)
- Suprachoroidal haemorrhage (0.04%)
Postoperative
| Complication | Notes |
|---|---|
| Posterior capsular opacification (PCO) | Most common late complication; "after-cataract"; treated with Nd:YAG laser capsulotomy |
| Cystoid macular oedema (CMO) | Reduced acuity, usually treatable with NSAIDs/steroids |
| Endophthalmitis | Rare (0.1%) but devastating; typically Staphylococcus epidermidis; requires urgent intravitreal antibiotics |
| Corneal decompensation | Requires corneal graft |
| Refractive surprise | Unexpected refractive outcome |
| Retinal detachment | <1%; higher risk in myopia |
| IOL dislocation | Especially with zonular weakness |
| Dry eye syndrome | Up to 1 in 3 patients postoperatively |
| IOP spike | Usually transient |
| Ptosis/diplopia | Persistent cases need further management |
9.1 Risk Summary (Informed Consent Figures)
- In ~1 in 1,000 operations: eye left with little or no sight
- In ~1 in 10,000: patient may lose the eye
- Endophthalmitis: 0.1%
- Suprachoroidal haemorrhage: 0.04%
10. Posterior Capsular Opacification (PCO)
PCO ("after-cataract") is the most common late complication of cataract surgery. Residual lens epithelial cells proliferate on the posterior capsule, causing visual deterioration similar to the original cataract. It is treated with Nd:YAG laser posterior capsulotomy, a brief outpatient procedure.
11. Congenital Cataract Management
Early treatment is critical to prevent deprivation amblyopia (permanent vision loss from a deprived visual axis during the sensitive period of visual development):
- Surgery should not be delayed once visually significant opacity confirmed
- Visual rehabilitation with contact lenses or glasses after surgery is mandatory
- Patching therapy of the sound eye to force the amblyopic eye to develop
- Prognosis is better for isolated inherited cataracts than for those with systemic or ocular co-pathology
12. Summary Table
| Feature | Key Points |
|---|---|
| Definition | Opacification of the crystalline lens |
| Global impact | Commonest reversible cause of blindness |
| Main types | Age-related (nuclear, cortical, PSC), secondary, traumatic, congenital |
| Key symptom | Painless, progressive visual loss + glare |
| Diagnosis | Slit lamp + retroillumination + biometry |
| Medical treatment | None proven effective |
| Surgery | Phacoemulsification + IOL (gold standard) |
| Main late complication | Posterior capsular opacification (treated with Nd:YAG) |
| Serious complication | Endophthalmitis (0.1%) |
| Congenital | 3/10,000 births; treat urgently to prevent amblyopia |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | Goldman-Cecil Medicine, International Edition | Robbins & Kumar Basic Pathology | Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.