I want to learn malaria from basics to clinics i should have proper simplified definition causes pathophysiology symptoms differential symptoms symptoms that confirm the disease
Reading File
Finding Sources
Searching PubMed
"malaria" AND "pathophysiology"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative data from multiple major textbooks plus key images. Let me now compile the complete, well-structured educational response.
Malaria: From Basics to Clinics
1. WHAT IS MALARIA? (Simple Definition)
Malaria is a potentially life-threatening infectious disease caused by a microscopic parasite called Plasmodium, which is transmitted to humans through the bite of an infected female Anopheles mosquito. The parasite invades and destroys red blood cells, causing waves of fever, chills, and severe anemia, and can affect multiple organs if untreated.
Simple analogy: Think of the malaria parasite as a saboteur that sneaks into your liver, trains an army, then repeatedly attacks and destroys your red blood cells in synchronized waves - which is why the fever comes in predictable cycles.
More than 200 million cases occur worldwide annually, causing over 600,000 deaths - most in sub-Saharan African children under 5 years old.
- Robbins & Kumar Basic Pathology
2. CAUSES (Etiology)
The Parasites - 5 Species Infect Humans
| Species | Disease Type | Severity | Fever Cycle | Special Features |
|---|---|---|---|---|
| P. falciparum | Tertian (malignant) | Most dangerous | Every 48 hrs | Cerebral malaria, drug resistance |
| P. vivax | Tertian (benign) | Moderate | Every 48 hrs | Hypnozoites - relapses |
| P. ovale | Tertian (benign) | Mild | Every 48 hrs | Hypnozoites - relapses |
| P. malariae | Quartan | Mild-moderate | Every 72 hrs | Nephrotic syndrome (chronic) |
| P. knowlesi | Daily | Moderate | Every 24 hrs | Zoonosis from macaques |
P. falciparum is the most important - responsible for most deaths. The others cause relatively mild disease.
The Vector
- Exclusively the female Anopheles mosquito (males don't bite)
- Bites primarily at dusk and dawn
- Humans are the only natural reservoir
Other (Rare) Routes of Transmission
- Blood transfusions
- Needle sharing (IV drug use)
- Organ transplantation
- Mother-to-fetus (congenital malaria)
Where Is It Found?
Endemic in parts of Africa, Asia, Oceania, Central America, and South America. With global travel, cases are now seen worldwide. Travelers returning from West Africa represent the most common source of imported falciparum malaria in the US.
3. PATHOPHYSIOLOGY (How It Causes Disease)
The Life Cycle - Step by Step

FIG: Life cycle of P. falciparum - Robbins & Kumar Basic Pathology
Step 1 - Entry (Mosquito Bite)
When an infected female Anopheles mosquito bites, she injects sporozoites into the bloodstream. Within minutes, sporozoites travel to the liver.
Step 2 - Liver Stage (Hepatic Phase, 1-4 weeks)
- Sporozoites use two surface proteins (thrombospondin-related adhesive protein and circumsporozoite protein) to bind to proteoglycans on hepatocytes
- Inside the liver, they multiply and transform into merozoites
- After 1-4 weeks, infected hepatocytes rupture, releasing thousands of merozoites into the blood
- Key point for P. vivax and P. ovale: Some parasites can remain dormant in the liver as hypnozoites - these cause relapses months or years later
Step 3 - Blood Stage (Erythrocytic Phase) - Where Symptoms Happen
- A lectin-like molecule on the merozoite surface binds to glycophorin (a red cell protein), allowing invasion
- Inside the RBC, the parasite forms a ring trophozoite inside a "digestive vacuole"
- Trophozoites differentiate into schizonts, which express PfEMP1 (Plasmodium falciparum Erythrocyte Membrane Protein 1) - this protein forms "knobs" on the RBC surface
- PfEMP1 binds to adhesion molecules on blood vessel walls (ICAM-1, VCAM-1, CD36) → parasitized RBCs stick to capillary walls (sequestration) - this is the key mechanism of severe disease
- After several days, schizonts rupture → release more merozoites → infect more RBCs → this synchronized rupture causes the cyclical fever
- Some trophozoites become gametocytes (sexual forms) - if another mosquito bites this person, the cycle restarts in the mosquito
Why Does This Cause Damage?
| Mechanism | Consequence |
|---|---|
| Mass destruction of RBCs | Hemolytic anemia, jaundice |
| RBC sequestration in capillaries | Organ ischemia, cerebral malaria |
| Synchronized schizont rupture | Cyclical fever and chills |
| Activation of phagocytes | Splenomegaly, hepatomegaly |
| Hemoglobin released → hematin pigment | Brown discoloration of spleen/liver/brain |
| Inflammatory cytokines (TNF, IL-1) | Fever, rigors, hypoglycemia |
| Capillary leak in brain | Cerebral edema, coma |
"The destruction of red cells leads to hemolytic anemia... A characteristic brown malarial pigment derived from hemoglobin called hematin is released from the ruptured red cells and produces discoloration of the spleen, liver, lymph nodes, and bone marrow." - Robbins & Kumar Basic Pathology
4. SYMPTOMS (Clinical Presentation)
The Classic Malaria Attack - "The Fever Paroxysm"
The textbook presentation comes in three stages that repeat in cycles:
| Stage | Duration | What the Patient Feels |
|---|---|---|
| Cold stage (rigor) | 15-60 min | Violent shaking, teeth chattering, intense cold sensation despite rising temperature |
| Hot stage | 2-6 hours | High fever (39-41°C / 102-106°F), throbbing headache, flushed skin, delirium possible |
| Sweating stage | 2-4 hours | Profuse drenching sweats, temperature drops, exhaustion |
Fever periodicity by species:
- Every 24 hours (quotidian) → P. knowlesi
- Every 48 hours (tertian) → P. falciparum, P. vivax, P. ovale
- Every 72 hours (quartan) → P. malariae
Other Common Symptoms
- Headache (very common, often severe)
- Myalgia and arthralgia (muscle and joint pains)
- Nausea, vomiting, anorexia
- Abdominal pain (can mimic gastroenteritis)
- Diarrhea (up to 30% of cases - often misdiagnosed as gastroenteritis)
- Fatigue and malaise
- Pallor (from anemia)
- Jaundice (from RBC hemolysis)
- Splenomegaly (especially in chronic or recurrent infection)
- Hepatomegaly (less common)
"Although it is classically associated with cyclical fevers, malaria presents various symptoms, including headache and diarrhea. Fever is common but not universal at initial presentation." - Rosen's Emergency Medicine
5. SIGNS OF SEVERE / COMPLICATED MALARIA (P. falciparum)
These are red flags requiring immediate IV treatment:
| Warning Sign | Threshold / Clinical Finding |
|---|---|
| Altered consciousness / prostration | Glasgow Coma Scale < 11 |
| Repeated seizures | > 2 generalized seizures |
| Severe anemia | Hemoglobin < 7 g/dL |
| Acute kidney failure | Creatinine > 3 mg/dL |
| Jaundice / liver failure | Total bilirubin > 3 mg/dL |
| Pulmonary edema / respiratory distress | Clinical or radiographic |
| Hypoglycemia | Blood glucose < 40 mg/dL |
| Shock | Systolic BP < 80 mmHg |
| Bleeding / DIC | Spontaneous bleeding |
| Severe acidosis | Bicarbonate < 15 mmol/L or lactate > 5 mmol/L |
| Hemoglobinuria | Dark ("Coca-Cola") urine |
| High parasitemia | > 2% of RBCs parasitized on smear |
Specific Severe Complications
1. Cerebral Malaria
- Parasitized RBCs with PfEMP1 knobs adhere to cerebral capillaries → sludging, ischemia, petechial hemorrhages, cerebral edema
- Features: fever + altered mental status + coma + seizures
- Rapidly fatal if untreated - mainly kills children
2. Blackwater Fever
- Massive intravascular hemolysis → hemoglobinemia + hemoglobinuria + jaundice + renal failure
- Urine turns dark brown or black (hence the name)
- Associated with P. falciparum, especially with quinine treatment
3. Severe Malarial Anemia
- Hemoglobin can fall to critically low levels from:
- Direct lysis of parasitized RBCs
- Immune destruction of non-parasitized RBCs (antibody-mediated)
- Inhibited erythropoietin response
- Splenic sequestration
4. Acute Pulmonary Edema / ARDS
- Cytokine-driven capillary leak in the lungs
- High mortality, can develop even after treatment begins
5. Hypoglycemia
- Especially dangerous in children and pregnant women
- Two mechanisms: parasite consumes glucose directly; quinine stimulates insulin release
6. BLOOD SMEAR APPEARANCE (Microscopic Diagnosis)
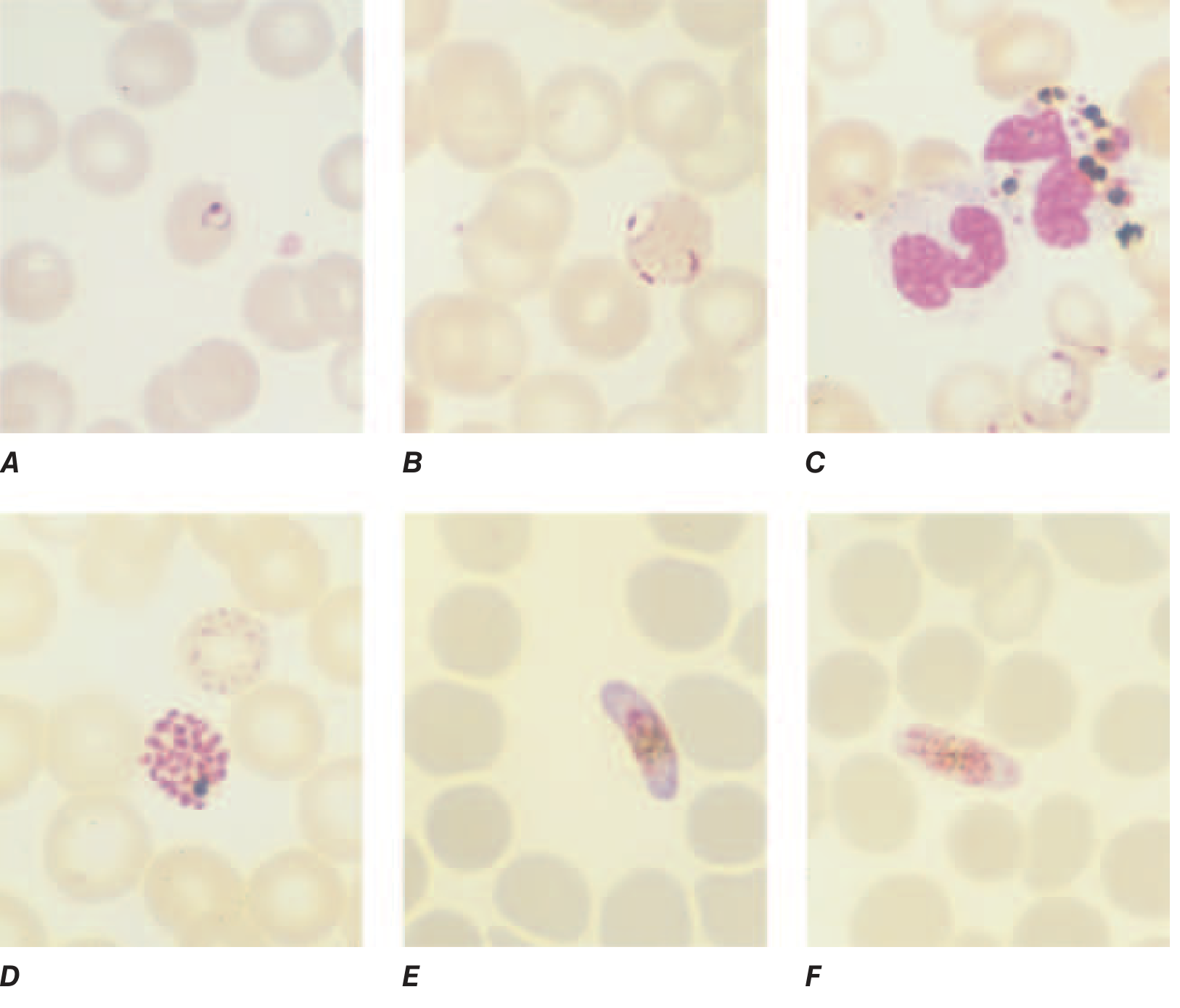
FIG: P. falciparum blood smear - A: young trophozoite (ring form), B: old trophozoite, C: pigment in WBCs, D: schizont, E: female gametocyte (banana/crescent), F: male gametocyte - Harrison's Principles of Internal Medicine
Key identifying features of P. falciparum on smear:
- Multiple ring forms per RBC (other species only have one)
- Rings at the periphery of the RBC ("appliqué" or "accolé" forms)
- Banana/crescent-shaped gametocytes - pathognomonic for P. falciparum
- No enlargement of infected RBC (P. vivax enlarges the RBC)
- No Schüffner's dots (P. vivax and ovale have these)
7. DIFFERENTIAL DIAGNOSIS
Malaria is the "great mimicker" of tropical medicine. Consider these conditions when evaluating febrile patients with travel history:
Common Conditions to Rule Out First
| Condition | How it's Similar | Key Distinguishing Feature |
|---|---|---|
| Influenza | Fever, myalgia, headache | No travel history, no anemia, smear negative |
| Typhoid fever | Prolonged fever, abdominal pain | Stepladder fever, rose spots, blood culture positive |
| Dengue fever | High fever, severe headache, myalgia | "Breakbone" pain, rash, thrombocytopenia, Aedes mosquito |
| Leptospirosis | Fever, headache, jaundice | Water/animal exposure, conjunctival suffusion, muscle tenderness |
| Bacterial sepsis | High fever, altered mentation | Localizing source (UTI, pneumonia, etc.), blood culture |
| Viral gastroenteritis | Fever, diarrhea, vomiting | No travel to endemic area, smear negative |
| UTI / Pyelonephritis | Fever, flank pain | Positive urinalysis and urine culture |
Conditions to Distinguish from Severe Malaria
| Condition | Resembles | Key Distinction |
|---|---|---|
| Bacterial meningitis | Cerebral malaria (fever + coma) | Neck stiffness, CSF pleocytosis, smear negative |
| Viral encephalitis | Cerebral malaria | CSF viral PCR; smear negative |
| Stroke | Focal neurological signs | Imaging shows infarct; no fever/parasitemia |
| Hemolytic uremic syndrome | Hemolytic anemia + renal failure | No travel history; blood smear shows schistocytes but no parasites |
| Sickle cell crisis | Anemia + painful crisis | Sickle hemoglobin on electrophoresis |
| Viral hepatitis | Jaundice + fever | Hepatitis serology; no cyclical fever, smear negative |
"Cerebral malaria may manifest with confusion and mental status changes and should be differentiated from meningitis and encephalitis." - Rosen's Emergency Medicine
Bottom line on differential: Always think malaria in any febrile patient who has traveled to an endemic region. As Harrison's states: "Malaria is not a clinical diagnosis" - you must confirm with a blood smear or rapid test.
8. SYMPTOMS THAT CONFIRM THE DIAGNOSIS (Pathognomonic / Highly Specific Features)
While no symptom alone is diagnostic, these features together strongly point to malaria:
Clinical Features Highly Suggestive
-
Periodic fever with rigors - The classic synchronized cycle (every 48 or 72 hours) is the most characteristic symptom. When the fever paroxysm is clearly cyclical with cold-hot-sweating stages, malaria is the top differential.
-
Banana/crescent-shaped gametocytes on blood smear - Pathognomonic for P. falciparum. Nothing else looks like this.
-
Travel to endemic region + fever - Sensitivity of fever and/or headache > 95% in low-endemicity areas.
-
Splenomegaly in a febrile traveler - Not diagnostic alone, but adds strong specificity.
-
Hemoglobinuria (dark urine) + fever - Blackwater fever; very specific for severe falciparum malaria.
Definitive Diagnostic Criteria (from Harrison's)
The diagnosis requires laboratory confirmation:
-
Thick and thin blood smears (Giemsa stain at pH 7.2) - GOLD STANDARD
- Thick smear: more sensitive (concentrates parasites)
- Thin smear: identifies species and counts parasitemia
- If smear is negative by an experienced microscopist → patient does not have malaria
-
Rapid Diagnostic Tests (RDTs) - Antigen-based dipstick tests; used when reliable microscopy is unavailable
-
PCR - Most sensitive; used for low parasitemia or species confirmation
9. TREATMENT (Overview)
Uncomplicated Malaria
| Situation | First-Line Treatment |
|---|---|
| Chloroquine-sensitive P. falciparum (Central America, Caribbean) | Chloroquine |
| Chloroquine-resistant P. falciparum (most of world) | Artemether + Lumefantrine (Coartem) OR Atovaquone + Proguanil (Malarone) |
| P. vivax / P. ovale | Chloroquine + Primaquine (to eliminate hypnozoites and prevent relapse) |
| P. malariae | Chloroquine alone |
Severe / Complicated Malaria
- IV Artesunate - First-line worldwide; superior to quinine (2.4 mg/kg IV every 12 hrs on day 1, then daily)
- IV Quinine - Alternative if artesunate unavailable
- Supportive care: IV fluids, blood transfusion, anti-seizure medication, ventilation as needed
Chemoprophylaxis for Travelers
- Atovaquone-proguanil (Malarone) - Daily; start 1-2 days before, continue 7 days after
- Mefloquine - Weekly; start 2-3 weeks before
- Doxycycline - Daily; start 1-2 days before
- Chloroquine - Weekly; only in chloroquine-sensitive areas
10. QUICK SUMMARY TABLE
| Feature | Details |
|---|---|
| Cause | Plasmodium parasite (5 species); P. falciparum most deadly |
| Vector | Female Anopheles mosquito |
| Incubation | 1-4 weeks (up to months for P. vivax/ovale with hypnozoites) |
| Classic symptom | Periodic fever paroxysm: cold → hot → sweating |
| Fever cycle | 24h (P. knowlesi), 48h (P. falciparum, vivax, ovale), 72h (P. malariae) |
| Deadly complication | Cerebral malaria (P. falciparum) |
| Pathognomonic finding | Banana-shaped gametocytes (P. falciparum) on blood smear |
| Diagnosis | Thick/thin blood smear (Giemsa stain) or rapid antigen test |
| Treatment (uncomplicated) | Artemether-lumefantrine or Atovaquone-proguanil |
| Treatment (severe) | IV Artesunate |
| Prevention | Bed nets, insect repellent, mosquito control, chemoprophylaxis |
Sources: Robbins & Kumar Basic Pathology, Harrison's Principles of Internal Medicine (22e), Rosen's Emergency Medicine, Goldman-Cecil Medicine, Goodman & Gilman's Pharmacological Basis of Therapeutics.
This is a shared conversation. Sign in to Orris to start your own chat.