Pulmonary vasculitis full details for md exams 15marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive 15-mark MD exam answer on Pulmonary Vasculitis:
PULMONARY VASCULITIS
DEFINITION & INTRODUCTION
Pulmonary vasculitis is inflammation of pulmonary blood vessels, usually a manifestation of a systemic disorder affecting vessels of different sizes through a variety of immunologic mechanisms. It can be classified as:
- Primary vasculitis — heterogeneous syndromes of unknown etiology sharing clinical response to immunosuppressive therapy
- Secondary vasculitis — occurs in the context of a defined underlying disorder (SLE, RA, infections) or as an incidental histopathologic finding
— Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
CLASSIFICATION (Chapel Hill 2012 Consensus Nomenclature)
| Category | Disease | Respiratory Involvement | ANCA |
|---|---|---|---|
| Large vessel | Giant-cell arteritis | Rare | No |
| Takayasu arteritis | Frequent | No | |
| Medium vessel | Polyarteritis nodosa | Rare | No |
| Kawasaki disease | No | No | |
| Small vessel (ANCA-associated) | GPA (Wegener) | Frequent | >80% |
| Microscopic polyangiitis (MPA) | Frequent | >80% | |
| EGPA (Churg-Strauss) | Frequent | >50% | |
| Immune complex small vessel | Anti-GBM disease | Frequent | No |
| IgA vasculitis | Rare | — | |
| Cryoglobulinemic vasculitis | Rare | No | |
| Variable vessel | Behçet disease | Common | No |
The three small vessel vasculitides that most frequently present with respiratory symptoms are GPA, MPA, and EGPA — collectively termed "ANCA-associated vasculitis" (AAV).
PATHOGENESIS OF ANCA-ASSOCIATED VASCULITIS
ANCA (antineutrophil cytoplasmic antibodies) are the key serologic markers:
- PR3-ANCA / C-ANCA — cytoplasmic immunofluorescence pattern; characteristic of GPA (>80% positive)
- MPO-ANCA / P-ANCA — perinuclear pattern; predominates in MPA and EGPA
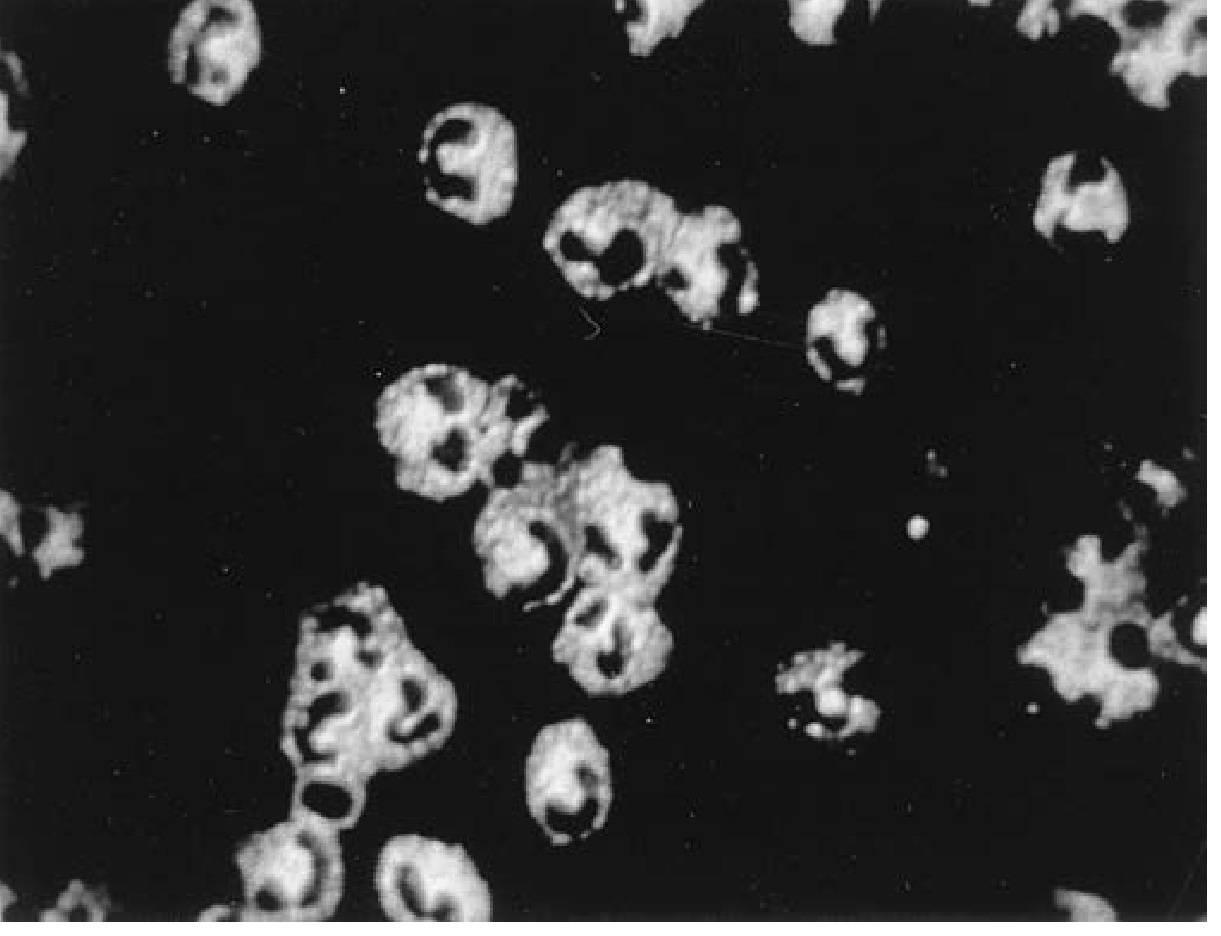
Fig: C-ANCA (PR3) immunofluorescence pattern — Fishman's Pulmonary Diseases
Despite circulating ANCA, tissue lesions show minimal immunoglobulin deposits ("pauci-immune" lesions). Pathogenic mechanisms include:
- ANCA activation of primed neutrophils → release of oxygen radicals and proteolytic enzymes → endothelial apoptosis
- ANCA enhance neutrophil adhesion to endothelial cells via upregulation of adhesion molecules
- Genetic predisposition: HLA-DP association with PR3-ANCA; HLA-DQ with MPO-ANCA
- Epigenetic modifications increase expression of PR3 and MPO on neutrophil surfaces
I. GRANULOMATOSIS WITH POLYANGIITIS (GPA) — Formerly Wegener Granulomatosis
Definition
Necrotizing granulomatous inflammation of the respiratory tract + necrotizing vasculitis of small-to-medium vessels, classically forming a triad: upper airways + lower airways + kidneys.
Epidemiology
- Annual incidence: ~10–12 per million; predominantly whites and northern Europeans
- Can affect any age; incidence plateaus after age 50
Pulmonary Manifestations
Two distinct patterns:
- Diffuse Alveolar Hemorrhage (DAH) from pulmonary capillaritis — presents as hemoptysis, falling Hb, bilateral ground-glass opacities
- Necrotizing granulomatous nodules/masses (most common form) — typically bilateral, may cavitate

- Tracheobronchial involvement in 15–55%, more common in women; presents with cough, wheezing, hemoptysis, subglottic stenosis
- Organizing pneumonia pattern can occur
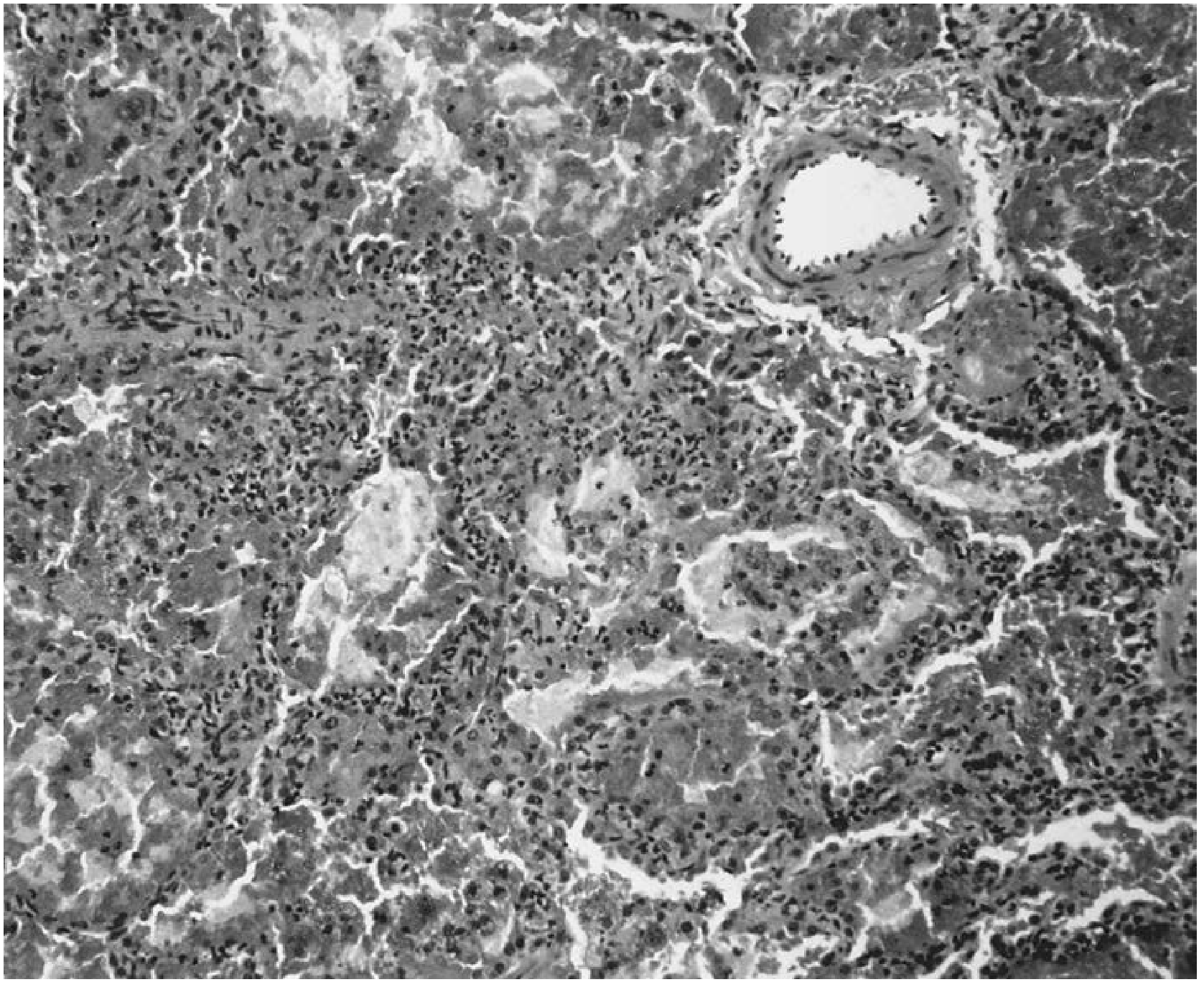
Histopathology
- Small necrotizing microabscesses → coalesce → geographic basophilic necrosis with palisading histiocytes and scattered giant cells
- Granulomatous vasculitis when inflammation extends into vessel walls (secondary to granulomatous inflammation, distinct from capillaritis)
- Background: mixed infiltrate (lymphocytes, plasma cells, giant cells, eosinophils)
- Sarcoid-like non-necrotizing granulomas are NOT found in GPA
Diagnosis
- Serology: C-ANCA/PR3-ANCA positive >80%
- Lab: Elevated ESR/CRP, anemia, elevated creatinine, hematuria, proteinuria
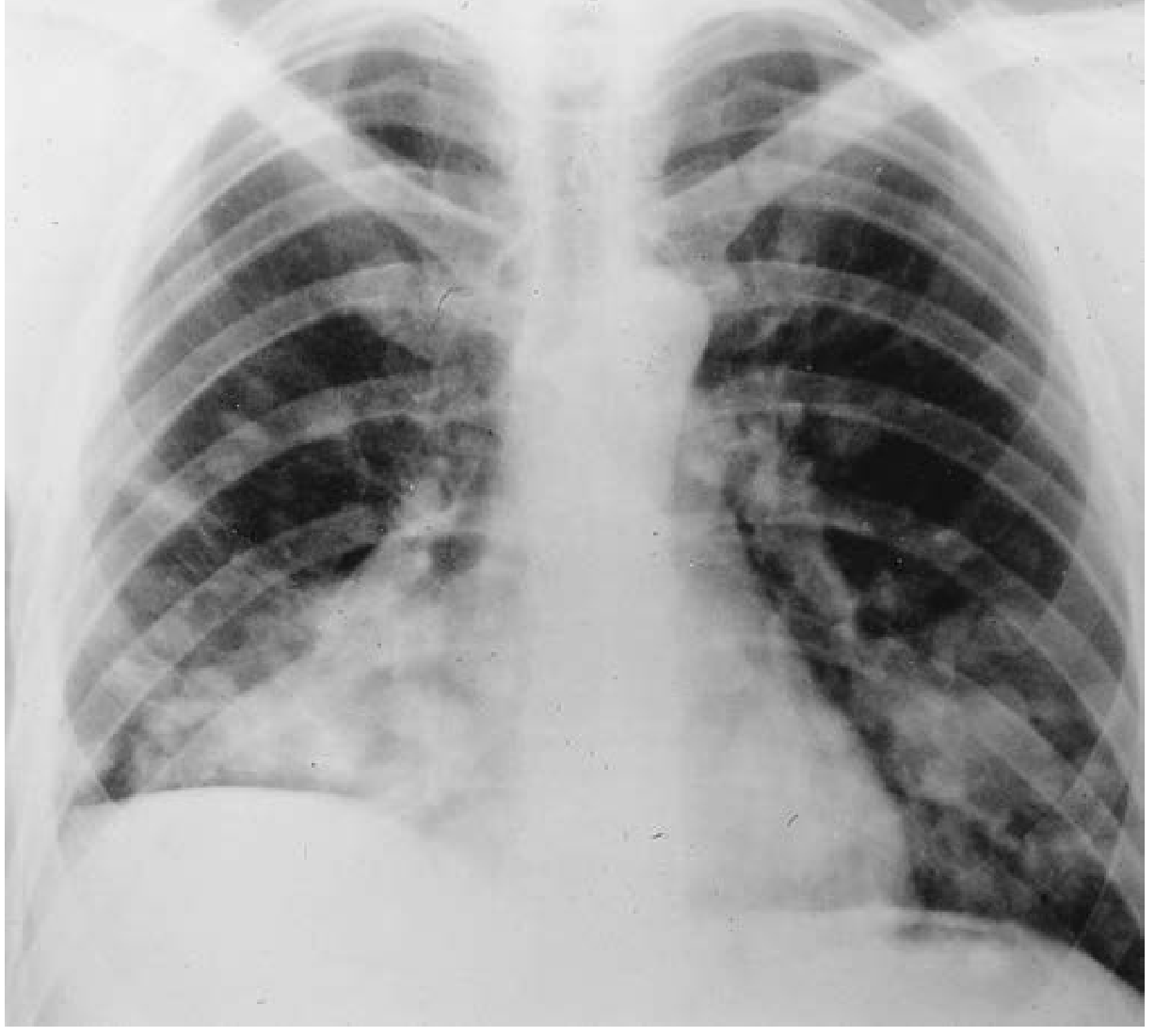
- Imaging: Bilateral nodules, masses, cavities ± ground-glass infiltrates (DAH)
- Biopsy: VATS lung biopsy (highest yield for isolated lung disease); transbronchial biopsy supports diagnosis in ~50% combined with ANCA; renal biopsy shows pauci-immune focal segmental necrotizing glomerulonephritis with crescents
Differential Diagnosis
- Infections (fungal, Nocardia), organizing pneumonia, metastatic disease, lymphomatoid granulomatosis (EBV-related T-cell-rich B-cell lymphoma — an important mimic), lymphoproliferative disorders
II. MICROSCOPIC POLYANGIITIS (MPA)
Key Features
- Necrotizing small vessel vasculitis without granuloma formation — this separates MPA from GPA
- No upper airway involvement (sinusitis, nasal disease absent — their presence suggests EGPA or GPA)
- Kidneys most affected (up to 80%) — pauci-immune focal segmental necrotizing glomerulonephritis with crescents
- DAH from pulmonary capillaritis affects 10–30% of patients
- MPA is the most frequent cause of pulmonary-renal syndrome
- Association with ILD (interstitial lung disease) increasingly recognized, particularly with MPO-ANCA
Serology
- P-ANCA/MPO-ANCA positive in 40–80%; C-ANCA/PR3-ANCA less common
- Histopathologically indistinguishable from GPA capillaritis
Treatment
Same approach as severe GPA (see below).
III. EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) — Formerly Churg-Strauss Syndrome
Definition
Small vessel necrotizing vasculitis classically associated with asthma, allergic rhinitis, peripheral eosinophilia, extravascular necrotizing granulomas, and eosinophilic tissue infiltrates.
Three Clinical Phases
- Prodromal phase: Allergic rhinitis, nasal polyposis, sinusitis, adult-onset asthma
- Eosinophilic phase: Peripheral blood and tissue eosinophilia (typically 5,000–20,000/μL); eosinophilic pneumonia, gastroenteritis
- Vasculitic phase: Small vessel vasculitis — mononeuritis multiplex (75%), palpable purpura, cardiomyopathy (60% — major cause of death), renal involvement (25%)
Pulmonary Manifestations
- Pulmonary opacities (eosinophilic pneumonia pattern): ill-defined, migratory, peripheral-predominant ground-glass to consolidation — present in 37–72% on CXR
- DAH is rare (contrast with GPA/MPA)
- Cavitary lesions extremely unusual
- CT: airspace consolidation, centrilobular nodules, bronchial wall thickening
Diagnostic Criteria (Cottin & Cordier)
- Asthma
- Peripheral eosinophilia >1500/mm³ and/or alveolar eosinophilia >25%
- Extrapulmonary clinical manifestations:
- Mononeuritis multiplex, cardiomyopathy, or palpable purpura, OR
- Any extrapulmonary manifestation + histopathologic vasculitis on biopsy, OR
- ANCA (anti-MPO or anti-PR3) positivity
Serology
- MPO-ANCA positive in 40–60% overall; 75–100% in those with renal involvement
- Elevated IgE levels; markedly elevated eosinophils
Histopathology
- Microgranulomas, fibrinoid necrosis, thrombosis of small vessels
- Eosinophilic infiltrates in vessels and extravascular tissues — distinguishes EGPA from GPA/MPA
IV. OTHER PULMONARY VASCULITIDES
Behçet Disease
- Immune complex–mediated vasculitis affecting vessels of all sizes
- Characterized by oral + genital aphthous ulcers, uveitis, cutaneous lesions
- Pulmonary artery aneurysms are the hallmark — detected by CT/MR angiography
- Massive hemoptysis (often fatal) from erosion of aneurysms into bronchi
- Prognosis: ~1/3 die within 2 years of pulmonary involvement
- Treatment: corticosteroids + cyclophosphamide/azathioprine; TNF-α inhibitors for refractory disease; anticoagulation should be AVOIDED once pulmonary arteritis present
Classic Polyarteritis Nodosa (PAN)
- Affects medium vessels; does NOT cause glomerulonephritis or DAH (no capillary involvement)
- Rare lung hemorrhage via bronchial artery involvement
- Most cases today associated with hepatitis B/C — antiviral therapy is central
Idiopathic Pauci-immune Pulmonary Capillaritis
- Diagnosis of exclusion: capillaritis with no systemic disease, no autoantibodies, no immune deposits
- Histologically identical to AAV; responds to similar immunosuppression
DIFFUSE ALVEOLAR HEMORRHAGE (DAH) — Unifying Concept
DAH is the common clinical presentation of several pulmonary vasculitides:
| Feature | Details |
|---|---|
| Symptoms | Hemoptysis, dyspnea, falling hemoglobin |
| Hemoptysis absent in up to 1/3 of cases | |
| Imaging | Bilateral ground-glass opacities / consolidation |
| BAL | Progressively bloodier aliquots; >20% hemosiderin-laden macrophages |
| Causes | GPA, MPA, anti-GBM disease, SLE, idiopathic capillaritis |
| Histology | Pulmonary capillaritis (neutrophilic infiltration of alveolar septa) |
INVESTIGATIONS SUMMARY
| Investigation | Finding |
|---|---|
| ANCA (IIF + ELISA) | C-ANCA/PR3 → GPA; P-ANCA/MPO → MPA/EGPA |
| FBC | Anemia, eosinophilia (EGPA) |
| ESR, CRP | Elevated |
| Urine | Hematuria, proteinuria, red cell casts |
| Serum creatinine | Elevated in renal involvement |
| Chest X-ray | Nodules, cavities, bilateral infiltrates |
| HRCT | Nodules ± cavitation, ground-glass, consolidation |
| Bronchoscopy + BAL | Confirm DAH; exclude infection |
| Biopsy | Definitive diagnosis (lung, kidney, skin, nerve) |
| Anti-GBM antibody | Exclude Goodpasture syndrome |
TREATMENT
Induction of Remission (Severe AAV — GPA/MPA)
- IV methylprednisolone 1 g/day × 3 days, then oral prednisolone 1 mg/kg/day
- Rituximab (375 mg/m² × 4 doses or 2 × 1 g doses) OR cyclophosphamide (IV/oral)
- RAVE trial: Rituximab = cyclophosphamide for induction; rituximab preferred in relapsing disease
- PEXIVAS trial: Plasmapheresis does NOT reduce end-stage renal disease/death; rapid steroid taper equally effective with fewer side effects
Maintenance Therapy
- Once remission achieved: azathioprine, methotrexate, or mycophenolate mofetil
- Low-dose rituximab effective for maintenance (RITAZAREM trial)
- Duration: typically 24–48 months minimum
- PCP prophylaxis (TMP-SMX) for all patients
EGPA
- Glucocorticoids alone sufficient in most cases (prednisone 1 mg/kg/day)
- Add cyclophosphamide for life-threatening manifestations (cardiac, renal, severe neuropathy)
- Anti-IL-5 therapy: Mepolizumab 300 mg SC every 4 weeks — FDA-approved for EGPA
- Anti-IgE therapy with omalizumab for predominantly asthma/sinonasal disease
- Five-factor score (FFS) guides need for cyclophosphamide addition
Limited GPA (upper airway only)
- Oral DMARDs alone (methotrexate + glucocorticoids) without cyclophosphamide
PROGNOSIS
- Untreated GPA/MPA: mortality approaches 90% within 2 years (mostly from renal/pulmonary failure)
- With treatment: 5-year survival >80%; major causes of death are infection (immunosuppression) and relapse
- Relapse rates: higher with PR3-ANCA than MPO-ANCA; higher in GPA than MPA
- EGPA: 5-year survival >90% with treatment; cardiac involvement is the main mortality determinant
- Behçet pulmonary involvement: poor prognosis; ~1/3 die within 2 years
QUICK SUMMARY TABLE
| Feature | GPA | MPA | EGPA |
|---|---|---|---|
| Former name | Wegener | — | Churg-Strauss |
| Granulomas | Yes (necrotizing) | No | Yes (eosinophilic) |
| Upper airway | Yes | No | Yes (allergic) |
| Asthma/eosinophilia | No | No | Yes (hallmark) |
| DAH/capillaritis | Yes | Yes (most common) | Rare |
| Renal | Yes | Most common | Mild/rare |
| ANCA | PR3/C-ANCA >80% | MPO/P-ANCA >80% | MPO ~50% |
| Induction Rx | RTX / CYC + steroids | RTX / CYC + steroids | Steroids ± CYC |
| Specific agent | — | — | Mepolizumab |
Sources: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Chapter 74); Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume (Chapter 96); Robbins, Cotran & Kumar Pathologic Basis of Disease; The Washington Manual of Medical Therapeutics; Goldman-Cecil Medicine, International Edition.
This is a shared conversation. Sign in to Orris to start your own chat.