Types of Spinal Needle, its parts, uses and benefits
Reading File
Finding Sources
Searching the Web
types of spinal needles parts uses benefits clinical
Finding Sources
Reading Web Page
https://www.sinymedical.com/what-is-a-spinal-needle
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a complete, textbook-grounded overview of spinal needles.
Spinal Needles: Types, Parts, Uses, and Benefits
What Is a Spinal Needle?
A spinal needle is a long, hollow, styletted needle designed to access the subarachnoid (intrathecal) space through the lumbar vertebral interspaces. They are commercially available in a range of sizes, lengths, and tip designs. All spinal needles must have a tightly fitting, removable stylet that completely occludes the lumen - this prevents tracking of epithelial cells into the subarachnoid space.
Parts of a Spinal Needle
| Part | Description |
|---|---|
| Hub | The proximal end that connects to a syringe or drug delivery system; color-coded by gauge |
| Shaft (Cannula) | The long hollow tube through which drugs are injected or CSF is aspirated |
| Stylet | A solid inner rod that occludes the needle lumen during insertion; prevents tissue coring |
| Tip/Bevel | The distal end - its shape defines the needle type (cutting vs. pencil-point) |
| Injection Port | Either at the end (end-injection) or on the side (side-injection), depending on type |
| Introducer | A short, wider needle used to guide fine-gauge spinal needles through skin and tissue |
Classification by Tip Design
The two major categories are cutting-tipped and atraumatic (pencil-point) needles. Atraumatic needles provide better tactile sensation through tissue layers and, most importantly, significantly reduce the incidence of post-dural puncture headache (PDPH).
Types of Spinal Needles
Needle Tip Comparison (Diagram)
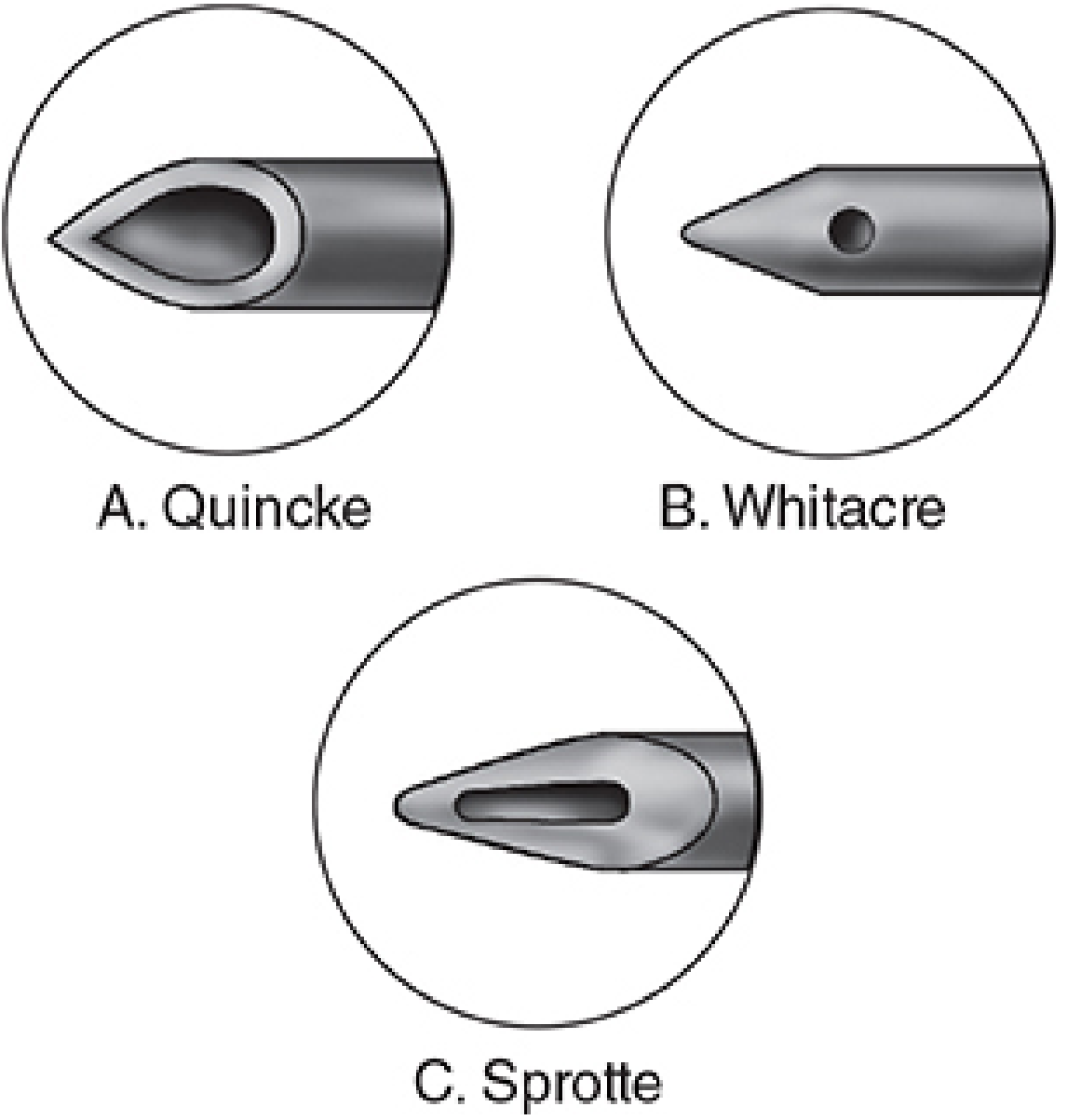
Spinal needle tip designs: Quincke (cutting, end-injection), Whitacre (pencil-point, side-injection), Sprotte (pencil-point with elongated side opening) - Morgan & Mikhail's Clinical Anesthesiology, 7e
Scanning Electron Micrographs of Tip Designs
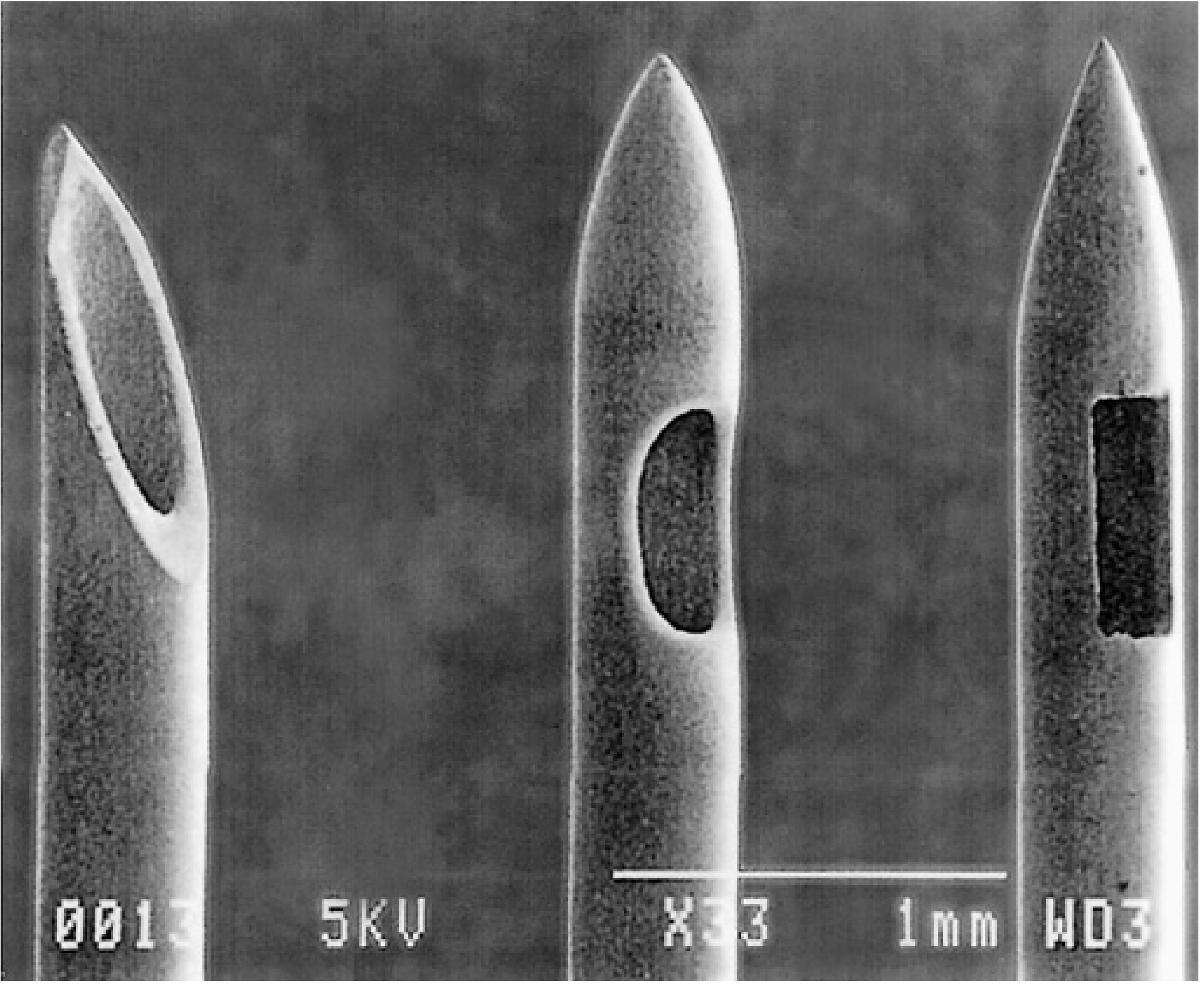
Electron micrographs showing actual dural tip architecture at 33x magnification - Miller's Anesthesia, 10e
1. Quincke Needle (Cutting/Standard)
- Tip: Sharp, beveled cutting tip (like a hypodermic needle)
- Injection: End injection
- How it works: Cuts through the dura mater cleanly
- Gauges: Available 20G-27G
- PDPH risk: Higher - the cut leaves a hole in the dura that leaks CSF until it heals over days to weeks
- Use: Most commonly supplied in standard lumbar puncture kits; widely used in emergency medicine
2. Whitacre Needle (Pencil-Point)
- Tip: Conical, rounded "pencil-point" tip with a small side-injection port
- Injection: Side injection (near the tip)
- How it works: Separates rather than cuts dural fibers, which reappose after withdrawal
- PDPH risk: Significantly lower than Quincke - the dural fibers spring back rather than leaving an open defect
- Use: Preferred for spinal anesthesia in obstetrics (C-sections, labor) and high-PDPH-risk patients (young women)
3. Sprotte Needle (Pencil-Point, Long Opening)
- Tip: Conical pencil-point tip with an elongated side-injection opening
- Injection: Side injection via a long lateral port
- Advantage: More vigorous CSF flow compared with similar gauge needles due to the larger opening
- Caution: Risk of failed block if only the distal part of the opening has entered the subarachnoid space while the proximal part of the opening is still outside the dura - the full drug dose may not be delivered intrathecally
- PDPH risk: Low (similar to Whitacre)
- Use: Common in European practice; 22G Sprotte used in obese patients where finer needles may bend
4. Pitkin Needle (Cutting)
- Tip: Short bevel cutting tip (less aggressive than Quincke)
- A historical cutting-type needle; less commonly used today
5. Pencan Needle (Pencil-Point)
- A variation of the pencil-point design, grouped with Whitacre and Sprotte
- Used similarly to minimize PDPH
6. Tuohy Needle
- Specially designed for epidural and continuous spinal access
- Has a curved tip (Husted bevel) to direct catheter passage
- Used when a spinal catheter needs to be threaded for continuous infusion
Dural Penetration: Cutting vs. Pencil-Point
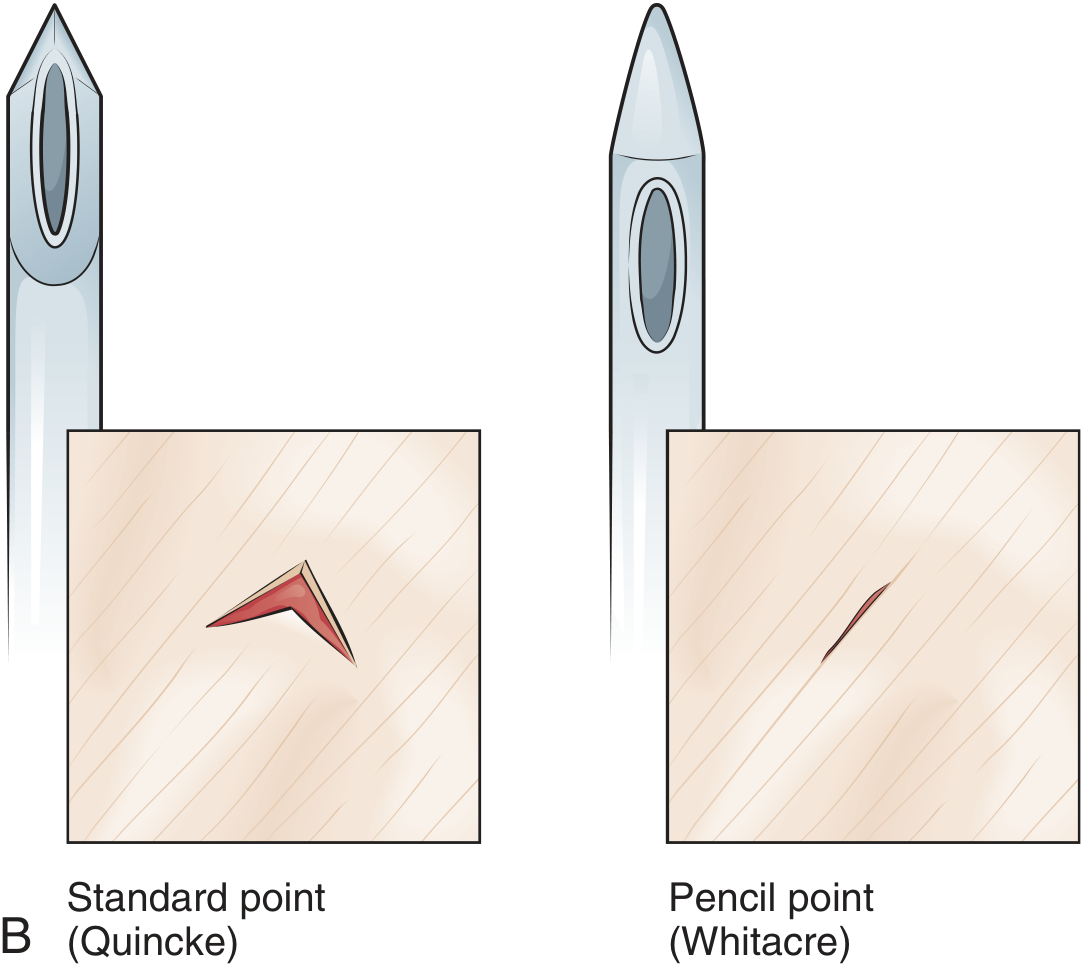
Quincke (left) cuts a triangular wound in the dura that leaks CSF. Whitacre (right) separates dural fibers, which reappose on withdrawal - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Gauge Sizes and PDPH Relationship
| Gauge Category | Sizes | Key Notes |
|---|---|---|
| Fine (25-27G) | 25G, 26G, 27G | Lowest PDPH risk; may need aspiration to confirm CSF; higher procedural failure rate |
| Mid (22-24G) | 22G, 23G, 24G | Balance of tactile feedback and PDPH reduction; 26G atraumatic reportedly lowest combined failure + PDPH rate |
| Coarse (18-22G) | 18G, 20G, 22G | Best tactile feedback; higher PDPH rate (up to 40% with 22G cutting needle); used where CSF flow speed matters |
- PDPH incidence: ~40% with a 22G cutting needle → less than 2% with a 29G needle
- The optimal balance of low PDPH and low procedural failure: 26G atraumatic (pencil-point) needle
Uses of Spinal Needles
| Application | Details |
|---|---|
| Spinal anesthesia | Intrathecal injection of local anesthetics for lower abdominal, pelvic, perineal, and lower limb surgery |
| Obstetric anesthesia | C-sections and labor analgesia (combined spinal-epidural common) |
| Lumbar puncture (diagnostic) | CSF collection for meningitis, subarachnoid hemorrhage, multiple sclerosis, Guillain-Barré |
| Intrathecal drug delivery | Chemotherapy (e.g., methotrexate), opioids, antibiotics directly into CSF |
| Myelography | Injection of contrast dye for spinal imaging |
| Measurement of CSF pressure | Opening and closing pressures in suspected idiopathic intracranial hypertension |
| Chronic pain management | Intrathecal drug delivery systems, nerve blocks |
Benefits of Each Type
| Needle | Key Benefit |
|---|---|
| Quincke | Widely available, easy to use, excellent CSF flow, standard kit component |
| Whitacre | Significantly reduced PDPH, better for young/female patients, separates rather than cuts dura |
| Sprotte | Vigorous CSF flow confirmation at placement, low PDPH, useful in deeper insertions |
| Tuohy | Enables catheter threading for continuous spinal or epidural anesthesia |
| Fine-gauge (25-27G) | Minimal tissue trauma, very low PDPH, ideal for day-surgery and ambulatory patients |
| Coarse-gauge (18-20G) | Strong tactile feedback, fast CSF flow for high-volume procedures |
Clinical Decision Summary
- For routine spinal anesthesia: 25-27G pencil-point (Whitacre or Sprotte) - lowest PDPH risk
- For lumbar puncture in emergency: 20-22G Quincke (standard kit), acceptable when speed matters
- For obese patients or difficult anatomy: 22G Sprotte - won't bend, adequate feedback
- For continuous spinal: Tuohy needle with catheter
- For pediatrics: L4-L5 or L5-S1 approach (cord ends at L3 at birth)
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Spinal Needles section
- Miller's Anesthesia, 10e, Preparation - Spinal Anesthesia
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, Equipment - Lumbar Puncture
- Barash, Cullen, & Stoelting's Clinical Anesthesia, 9e, Postdural Puncture Headache
This is a shared conversation. Sign in to Orris to start your own chat.