Mechanism of metastasis in form of flow chart
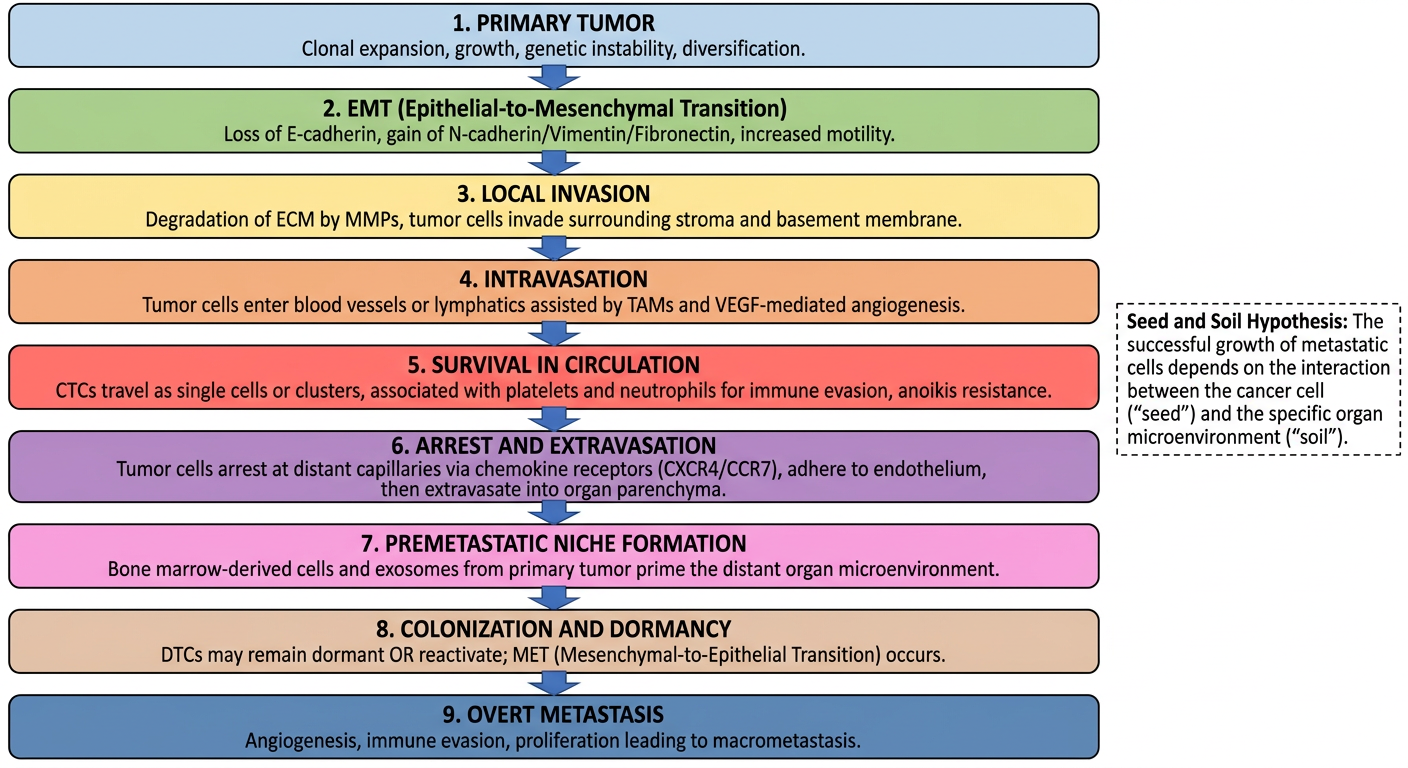
A detailed medical flowchart showing the mechanism of metastasis (the metastatic cascade). The flowchart flows top to bottom with labeled boxes and arrows. Steps in order: 1. PRIMARY TUMOR - Clonal expansion, growth, genetic instability, diversification. 2. EMT (Epithelial-to-Mesenchymal Transition) - Loss of E-cadherin, gain of N-cadherin/Vimentin/Fibronectin, increased motility. 3. LOCAL INVASION - Degradation of ECM by MMPs, tumor cells invade surrounding stroma and basement membrane. 4. INTRAVASATION - Tumor cells enter blood vessels or lymphatics assisted by TAMs and VEGF-mediated angiogenesis. 5. SURVIVAL IN CIRCULATION - CTCs travel as single cells or clusters, associated with platelets and neutrophils for immune evasion, anoikis resistance. 6. ARREST AND EXTRAVASATION - Tumor cells arrest at distant capillaries via chemokine receptors (CXCR4/CCR7), adhere to endothelium, then extravasate into organ parenchyma. 7. PREMETASTATIC NICHE FORMATION - Bone marrow-derived cells and exosomes from primary tumor prime the distant organ microenvironment. 8. COLONIZATION AND DORMANCY - DTCs may remain dormant OR reactivate; MET (Mesenchymal-to-Epithelial Transition) occurs. 9. OVERT METASTASIS - Angiogenesis, immune evasion, proliferation leading to macrometastasis. Seed and Soil Hypothesis noted at the side. Clean white background, professional medical illustration style, color-coded steps with blue arrows connecting each box.
Mechanism of Metastasis - The Metastatic Cascade
Textbook Diagram: Metastatic Cascade (Tietz Textbook of Laboratory Medicine)
Step-by-Step Explanation
Step 1 - Primary Tumor
- Clonal expansion of transformed cells with genetic instability
- Tumor heterogeneity develops through mutation and selection pressure
- Must reach >1-2 mm to require new blood supply (angiogenic switch)
Step 2 - EMT (Epithelial-to-Mesenchymal Transition)
- Loss of E-cadherin, Cytokeratin, EpCAM (epithelial markers)
- Gain of N-cadherin, Vimentin, Fibronectin (mesenchymal markers)
- Driven by TGF-β, Wnt, Notch, and cancer stem cell (CSC) signals
- Cells become motile, invasive, and resistant to anoikis
Step 3 - Local Invasion
- Matrix metalloproteinases (MMPs) degrade the basement membrane and ECM
- Cancer-associated fibroblasts (CAFs) and tumor-associated macrophages (TAMs) remodel stroma
- Invadopodia form at the leading edge of invading cells
Step 4 - Intravasation
- Tumor cells penetrate blood vessel or lymphatic vessel walls
- VEGF promotes angiogenesis and increases vascular permeability
- TAMs (M2 macrophages) facilitate entry into the vasculature
- Angptl4 (induced by TGF-β) disrupts pulmonary microvascular junctions to promote lung-specific seeding
Step 5 - Survival in Circulation
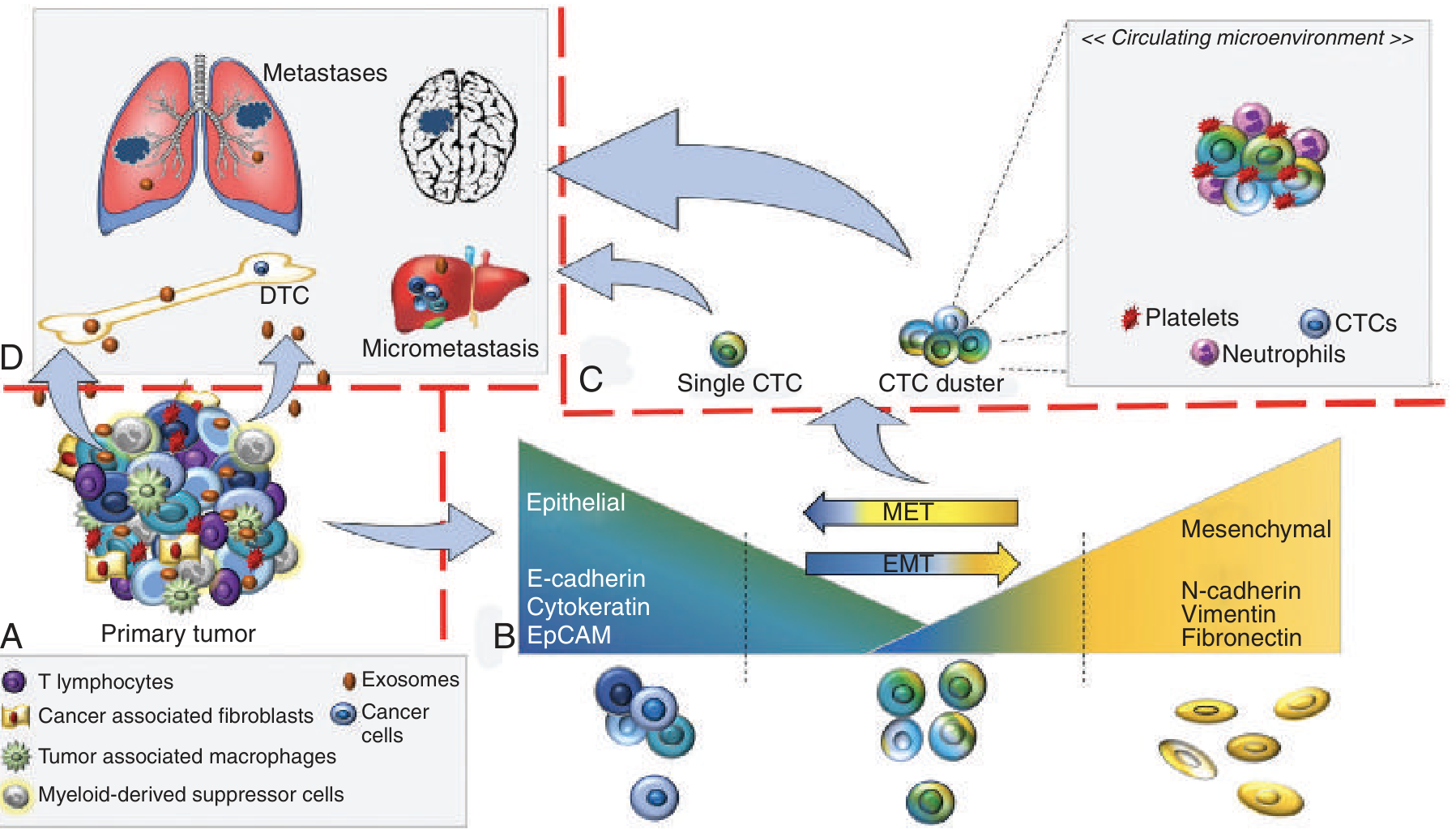
- Circulating tumor cells (CTCs) travel alone or in clusters/microemboli
- Platelets and neutrophils coat CTCs → immune evasion, protection from NK cells
- CTC clusters have 50x higher metastatic potential than single CTCs
- Anoikis resistance is required for survival without ECM contact
Step 6 - Arrest and Extravasation
- CTCs arrest in distant capillaries (size-dependent or receptor-mediated)
- Chemokine receptors on tumor cells (e.g., CXCR4, CCR7) bind organ-specific ligands (CXCL12, CCL21) - this explains organ tropism ("seed and soil")
- Surface protein metadherin facilitates adherence to pulmonary vascular endothelium
- Cells then extravasate into the organ parenchyma
Step 7 - Premetastatic Niche Formation
- Exosomes from the primary tumor travel ahead to distant organs
- Bone marrow-derived VEGFR1+ cells establish a permissive microenvironment before tumor cells arrive
- The niche is tumor-type specific (explains why different cancers favor different organs)
Step 8 - Dormancy vs. Reactivation
- Disseminated tumor cells (DTCs) may enter dormancy (months to years) - controlled by dormancy gene signatures
- MET (Mesenchymal-to-Epithelial Transition) reverses EMT to allow proliferation at the new site
- Immune surveillance, nutrient availability, and microenvironmental signals determine fate
Step 9 - Overt Metastasis (Colonization)
- Micrometastasis → macrometastasis via angiogenesis and immune evasion
- Metastasis-initiator cells (MICs) with stemness features drive outgrowth
- Final clinically detectable metastatic lesion
Key Molecular Players Summary
| Step | Key Molecules |
|---|---|
| EMT | TGF-β, Wnt, Notch, Snail, Twist, E-cadherin ↓ |
| Invasion | MMPs, uPA, integrins |
| Intravasation | VEGF, Angptl4, TAMs |
| Circulation | Platelets, neutrophils, CXCR4/CCR7 |
| Niche formation | Exosomes, VEGFR1+ BMDCs |
| Colonization | MET, stemness genes, angiogenesis |
- Tietz Textbook of Laboratory Medicine, 7th Edition (Fig. 71.13)
- Murray & Nadel's Textbook of Respiratory Medicine