Cardiac APD phages
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of the phases of the cardiac action potential (AP) and their ionic mechanisms, drawn from Braunwald's Heart Disease and Goodman & Gilman's Pharmacology.
Cardiac Action Potential - Phases (APD)
The cardiac AP is divided into 5 phases (0-4). The total duration from phase 0 through phase 3 constitutes the action potential duration (APD).
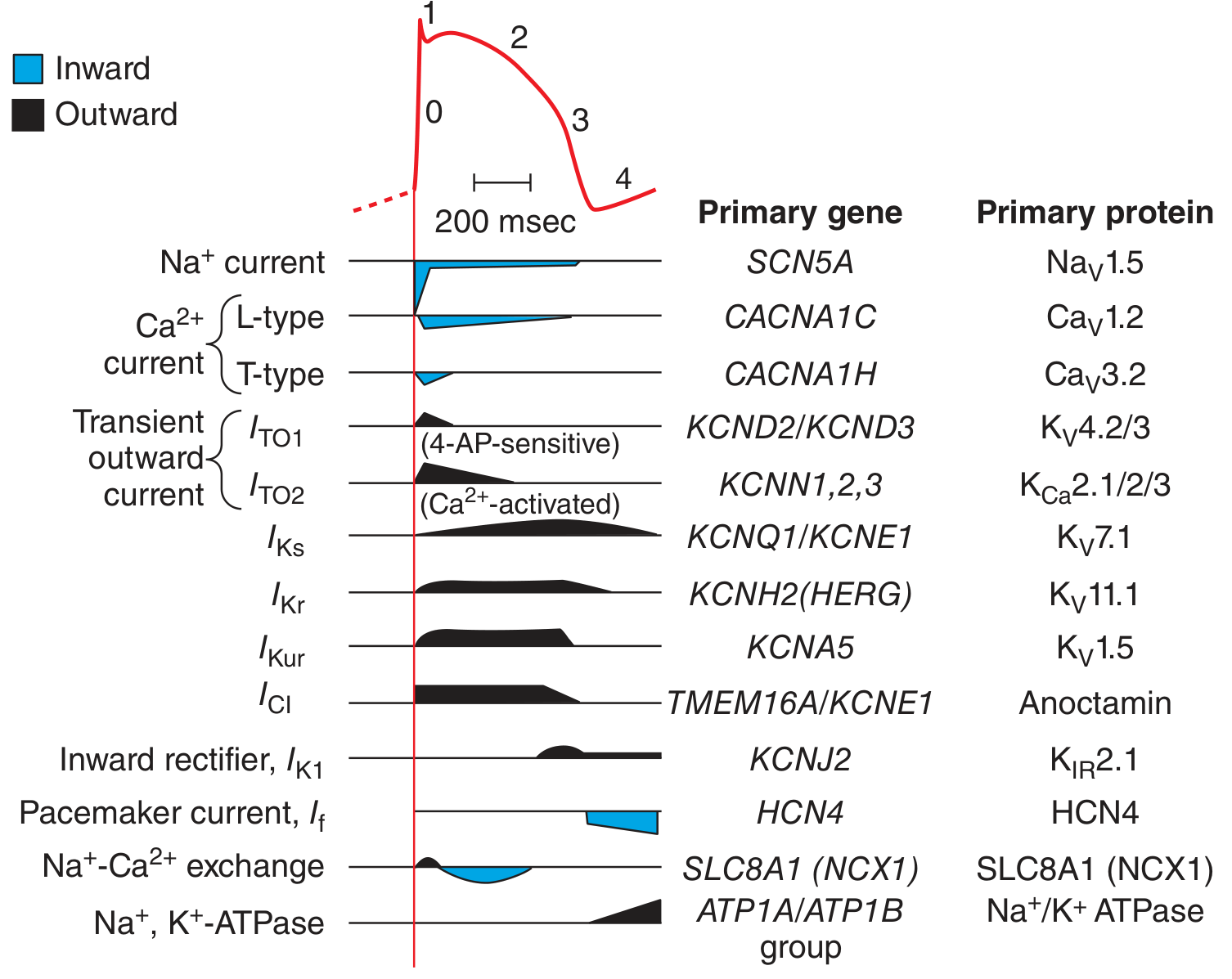
Phase 0 - Rapid Depolarization (Upstroke)
- Ion: Na+ (massive inward current)
- Channel/Gene: Na_V1.5 / SCN5A
- The resting membrane potential of working myocytes is approximately -80 to -90 mV. On reaching threshold, Na_V1.5 channels snap from closed -> open, allowing up to 10^7 Na+ ions/sec to enter.
- The maximal upstroke slope (dV/dt_max or V_max) reflects Na+ current magnitude and is the primary determinant of conduction velocity.
- Na+ channels then rapidly inactivate (~1 ms), ending phase 0.
- A small "late Na+ current" (I_NaL) persists into the plateau in some cells, contributing inward depolarizing current.
Phase 1 - Early Rapid Repolarization ("Notch")
- Ion: K+ (outward, repolarizing)
- Channels: Transient outward K+ channels - I_to1 (K_V4.2/4.3, genes KCND2/KCND3, 4-AP-sensitive) and I_to2 (Ca2+-activated, K_Ca2.1/2.2/2.3, genes KCNN1,2,3)
- At the end of phase 0, membrane potential is positive to E_K, so K+ rushes out, producing a brief downward notch.
- The notch is more prominent in epicardium than endocardium, contributing to transmural repolarization gradients.
- Phase 1 sets the voltage level for the subsequent plateau.
Phase 2 - Plateau
- Balance of inward and outward currents - the most distinctive feature of the cardiac AP
- Inward (depolarizing): L-type Ca2+ current (I_CaL, Ca_V1.2, CACNA1C) - the dominant inward current; also T-type Ca2+ (Ca_V3.2, CACNA1H)
- Outward (repolarizing): Delayed rectifier K+ currents - I_Ks (K_V7.1, KCNQ1/KCNE1), I_Kr (K_V11.1, KCNH2/HERG), I_Kur (K_V1.5, KCNA5, mainly atrial)
- The inward Ca2+ entry during phase 2 triggers calcium-induced calcium release (CICR) from the sarcoplasmic reticulum - this is the mechanism of electromechanical coupling and cellular contraction.
- As Ca2+ channels inactivate and K+ currents (especially I_Kr) build up, the balance tips toward repolarization.
Key pharmacological note: I_Kr (encoded by KCNH2/HERG) has a unique pore structure with aromatic residues that makes it unusually susceptible to drug block. Many drugs that prolong the APD (and QT interval) do so by blocking I_Kr - this is a major concern in drug development.
Phase 3 - Final Rapid Repolarization
- Ion: K+ (large outward current)
- Channels: Continued I_Kr and I_Ks, plus inward rectifier I_K1 (K_IR2.1, KCNJ2)
- Delayed rectifier K+ currents have fully activated; Ca2+ channels have inactivated - net current becomes strongly outward.
- Membrane potential returns to resting level (~-80 to -90 mV).
- Refractory period: From phase 0 until repolarization to approximately -60 mV in phase 3, the cell cannot be re-excited. This is the effective refractory period (ERP) and is closely tied to APD.
Phase 4 - Resting Membrane Potential / Diastolic Depolarization
- Ion: K+ (I_K1 - inward rectifier, outward at rest, sets resting potential)
- In working myocytes (ventricle, atria, His-Purkinje): stable resting potential of -80 to -90 mV, maintained by I_K1.
- In pacemaker cells (SA node, AV node): there is no stable phase 4 - instead, a slow spontaneous diastolic depolarization driven by I_f (the "funny current," HCN4, HCN4), which brings the cell back up to threshold for the next AP. This is the mechanism of automaticity.
SA/AV Node: "Slow Response" APs
The SA and AV nodes are distinct:
- Resting potential: only -50 to -65 mV (less negative)
- No fast Na+ current (inactivated at this voltage range)
- Phase 0 upstroke is slow, driven by L-type Ca2+ (not Na+)
- Automatic diastolic depolarization in phase 4 via I_f (pacemaker current)
- Much slower conduction velocity compared to His-Purkinje system
Summary Table
| Phase | Name | Key Current(s) | Ion Movement | Channel/Gene |
|---|---|---|---|---|
| 0 | Rapid depolarization | I_Na | Na+ in | Na_V1.5 / SCN5A |
| 1 | Early repolarization (notch) | I_to | K+ out | K_V4.2/4.3 / KCND2/3 |
| 2 | Plateau | I_CaL (in), I_Kr/I_Ks (out) | Ca2+ in, K+ out | Ca_V1.2 / CACNA1C; K_V11.1 / KCNH2 |
| 3 | Final repolarization | I_Kr, I_Ks, I_K1 | K+ out | KCNH2, KCNQ1, KCNJ2 |
| 4 | Resting (or pacemaker) | I_K1 (working cells); I_f (nodal) | K+ in/out; mixed | K_IR2.1 / KCNJ2; HCN4 |
Sources:
- Braunwald's Heart Disease (10th/12th ed.), Chapter 62: "The Cardiac Action Potential" and "Phases of the Cardiac Action Potential"
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 34: "The Cardiac Action Potential"
This is a shared conversation. Sign in to Orris to start your own chat.