Hiv Refer to apurba s sastry
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Note: Apurba S. Sastry's Essentials of Medical Microbiology is not available in this digital library. The notes below are sourced from Jawetz, Melnick & Adelberg's Medical Microbiology (28th ed.) - the primary international reference on which Apurba Sastry's text is closely based, covering all topics Sastry addresses.
HIV (Human Immunodeficiency Virus) - Complete Notes
1. INTRODUCTION & CLASSIFICATION
- HIV = etiologic agent of Acquired Immune Deficiency Syndrome (AIDS)
- AIDS first described in 1981 (homosexual men, USA); HIV-1 isolated by 1983
- Classification:
- Family: Retroviridae
- Genus: Lentivirus ("slow virus" - long incubation)
- Two types:
- HIV-1 - causes most AIDS worldwide; multiple subtypes
- HIV-2 - less virulent, slower progression, mainly West Africa
- HIV-1 Group M subtypes: Subtype C dominant in India & southern Africa; Subtype B in USA/Europe
2. STRUCTURE & COMPOSITION
Morphology
- Enveloped, spherical, ~100-120 nm
- Unique: cylindrical (bar-shaped/cone-shaped) nucleoid - seen on electron microscopy
Genome (9 genes)
The RNA genome is more complex than simple retroviruses:
| Gene | Protein | Function |
|---|---|---|
| gag | p17 (MA), p24 (CA), p7 (NC) | Core/capsid; p24 = major capsid antigen, used in diagnostics |
| pol | RT (p66), Integrase, Protease | Enzymes for replication |
| env | gp160 → gp120 (SU) + gp41 (TM) | Receptor binding & fusion |
| tat | Tat | Transactivation of viral genes; amplifies viral replication |
| rev | Rev | Exports unspliced mRNA from nucleus (needed for structural proteins) |
| nef | Nef | Downregulates CD4 & MHC-I; increases infectivity; activates resting T cells |
| vpr | Vpr | Nuclear import of preintegration complex; G2 arrest |
| vpu | Vpu | Degrades CD4; promotes virion release (HIV-1 only; HIV-2 has vpx) |
| vif | Vif | Overcomes host restriction factor APOBEC3G |
Surface Proteins
- gp120 - binds CD4; has 5 hypervariable regions (V1-V5); greatest genetic diversity here
- gp41 - transmembrane; mediates viral-cell membrane fusion
- p24 - major capsid antigen; detected in 4th generation tests
Host Restriction Factors (countered by HIV)
- APOBEC3G (countered by Vif) - deaminase that inhibits HIV
- TRIM5α - directs incoming viral particles to proteasomal degradation
3. REPLICATION CYCLE / LIFE CYCLE
This is the basis of all ARV drug targets:
| Step | Event | Drug Target |
|---|---|---|
| 1. Attachment | gp120 binds CD4 receptor | - |
| 2. Co-receptor binding | gp120 binds CCR5 (early/M-tropic) or CXCR4 (late/T-tropic) | CCR5 antagonists (Maraviroc) |
| 3. Fusion | gp41 conformational change → membrane fusion | Fusion inhibitors (Enfuvirtide) |
| 4. Reverse Transcription | RT converts ssRNA → dsDNA; high error rate → mutations | NRTIs, NNRTIs |
| 5. Integration | Integrase inserts viral DNA into host chromosome → provirus | INSTIs (Dolutegravir) |
| 6. Transcription | Host RNA pol + Tat amplification | - |
| 7. Translation | Structural proteins made as polyprotein precursors | - |
| 8. Maturation | Protease cleaves polyproteins → infectious virion | Protease Inhibitors |
Key: Individuals with homozygous CCR5-Δ32 deletion are highly resistant to HIV infection
4. PATHOGENESIS
Primary Target: CD4+ T Lymphocytes
- Normal CD4 count: ~1000 cells/μL
- Macrophages & monocytes: reservoir (not killed, harbor virus)
- DC-SIGN on dendritic cells: binds HIV, transports to lymph nodes (does not mediate direct entry)
Three Stages of Untreated HIV Infection
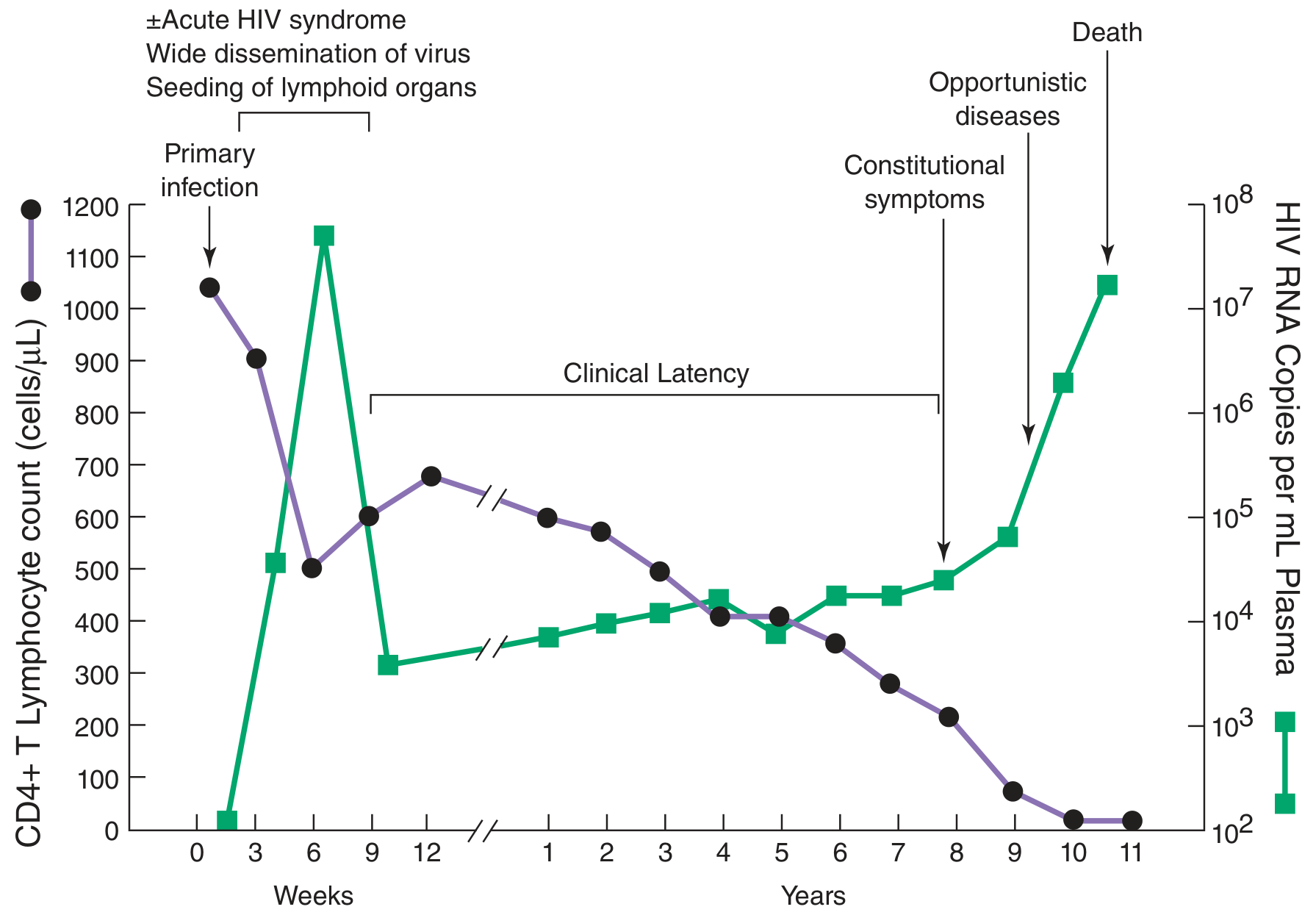
Stage 1 - Acute (Primary) HIV:
- Incubation: 4-11 days (mucosal infection → viremia)
- Viremia peaks, then detected for 8-12 weeks
- Acute mononucleosis-like syndrome in 50-75% (at 3-6 weeks): fever, rash, headache, pharyngitis, lymphadenopathy, night sweats
- Sharp drop in CD4 count
- Immune response at 1 week-3 months → viremia falls, CD4 rebounds
- But virus persists in lymphoid organs - infection is lifelong
Stage 2 - Clinical Latency (Chronic Asymptomatic):
- Lasts 8-10 years average without treatment
- Apparent latency but massive ongoing replication:
- ~10 billion particles produced & destroyed daily
- Plasma HIV half-life: 6 hours
- Infected CD4 half-life: 1.6 days
- Viral set point established - higher set point = faster progression to AIDS
- Gradual CD4 decline throughout
- Lymphoid organs = main replication site
Stage 3 - AIDS:
- CD4 falls to <200 cells/μL
- Prodrome = "diarrhea and dwindling": weight loss, fever, fatigue, chronic diarrhea, oral candidiasis (hairy leukoplakia), lymphadenopathy
- Opportunistic infections & AIDS-defining malignancies
- Death ~2 years after symptom onset (untreated)
5. OPPORTUNISTIC INFECTIONS (OI) IN AIDS
Occur when CD4 < 200 cells/μL:
| Category | Key Organisms |
|---|---|
| Protozoa | Toxoplasma gondii, Cryptosporidium spp., Isospora belli |
| Fungi | Candida (oral/esophageal), Cryptococcus neoformans, PCP (Pneumocystis jiroveci), Histoplasma, Coccidioides |
| Bacteria | M. avium-intracellulare (MAC), M. tuberculosis, Listeria, Nocardia, Salmonella |
| Viruses | CMV (CMV retinitis = most common severe eye complication), HSV, VZV, JC virus (→ PML), HBV, HCV |
- HIV + TB: HIV increases TB risk 20-fold; active TB dramatically increases HIV viremia
6. AIDS-DEFINING CANCERS
| Cancer | Viral Co-factor | Key Fact |
|---|---|---|
| Kaposi Sarcoma | HHV-8 | 20,000× more common in AIDS; vascular tumor of endothelial origin |
| Non-Hodgkin Lymphoma (Burkitt) | EBV | 1000× more common in AIDS |
| CNS Lymphoma | EBV | |
| Cervical Cancer | HPV | AIDS-defining in women |
| Anogenital Cancer | HPV |
7. DIAGNOSIS
Window Period
- Mean seroconversion: 3-4 weeks
- Most seropositive by: 6-12 weeks
- Virtually all positive by: 6 months
Tests
| Test | What It Detects | Use |
|---|---|---|
| 3rd Gen ELISA | HIV-1 & HIV-2 IgG + IgM antibodies | Screening |
| 4th Gen ELISA | HIV Ab + p24 antigen | Standard screening; shorter window period |
| 5th Gen test | HIV-1 Ab, HIV-2 Ab, p24 Ag (simultaneously differentiated) | Most advanced |
| Western Blot | Antibodies to specific bands (gp41, gp120, gp160 persist longest; p24 Ab declines with progression) | Confirmatory |
| RT-PCR / viral load | HIV RNA (quantitative) | Viral load monitoring, acute HIV, window period diagnosis |
| DNA PCR | Proviral DNA | Diagnosis in infants (maternal Ab makes serology useless) |
| Rapid tests | HIV antibodies (blood or oral fluid) | Field/resource-limited settings |
| HIV Genotyping | Mutations in RT & protease genes | Resistance testing before ART |
p24 antigen declines after antibodies develop (complexed with anti-p24); reappearance of p24 = poor prognosis
CD4 Count Thresholds
| CD4 Count | Action |
|---|---|
| <500 (old guideline) | Start ART |
| <350 | Prophylaxis for Toxoplasma |
| <200 | AIDS diagnosis; PCP prophylaxis with co-trimoxazole |
| <50 | MAC prophylaxis with azithromycin/clarithromycin |
8. ANTIRETROVIRAL THERAPY (ART / HAART)
Principle: Combination therapy at multiple steps prevents drug resistance
| Drug Class | Mechanism | Examples |
|---|---|---|
| NRTIs | Chain terminators (lack 3'-OH) → block RT | Zidovudine (AZT), Lamivudine (3TC), Tenofovir (TDF), Abacavir, Emtricitabine (FTC) |
| NNRTIs | Allosteric (non-competitive) RT inhibitors | Nevirapine, Efavirenz, Rilpivirine |
| PIs | Block viral protease → immature, non-infectious virions | Lopinavir, Atazanavir, Ritonavir (booster), Darunavir |
| INSTIs | Block integration of proviral DNA | Raltegravir, Dolutegravir (preferred), Bictegravir |
| Fusion inhibitors | Block gp41-mediated fusion | Enfuvirtide (T-20) |
| CCR5 antagonists | Block CCR5 co-receptor (requires tropism testing) | Maraviroc |
First-line ART: 2 NRTIs + 1 INSTI (current preferred regimen)
PEP (Post-Exposure Prophylaxis): Start within 72 hours, continue for 28 days
PrEP (Pre-Exposure Prophylaxis): Tenofovir/Emtricitabine daily for high-risk individuals
9. EPIDEMIOLOGY & TRANSMISSION
Routes
- Sexual (anal > vaginal > oral) - most common globally
- Blood - IV drug use, transfusions, needle-stick
- Vertical (Mother to Child) - transplacental, delivery, breastfeeding
- NOT transmitted by: casual contact, sneezing, coughing, food, toilet sharing
Global
-
35 million living with HIV/AIDS
- Sub-Saharan Africa most affected; some cities - 1 in 3 adults infected
- HIV-2 confined to West Africa
- India: Subtype C predominates
10. PREVENTION & VACCINES
- Condoms, needle exchange, PrEP, PEP, PMTCT (ART in pregnancy)
- Blood donor screening with NAT
- Vaginal tenofovir gel microbicide: reduces transmission by ~39%
- No effective vaccine available
- Challenges: rapid mutation, envelope variability, lack of animal model, unknown correlates of protective immunity
- Chimpanzees susceptible to HIV but do not develop immunodeficiency
QUICK REVISION TABLE
| Topic | Key Fact |
|---|---|
| Family / Genus | Retroviridae / Lentivirus |
| Unique morphology | Cylindrical/bar-shaped nucleoid on EM |
| Primary receptor | CD4 |
| Co-receptors | CCR5 (early) and CXCR4 (late) |
| Natural resistance | Homozygous CCR5-Δ32 deletion |
| HIV-1 vs HIV-2 gene difference | HIV-1 = vpu; HIV-2 = vpx |
| Accessory protein that fights APOBEC3G | Vif |
| Transactivation protein | Tat |
| mRNA export protein | Rev |
| MHC-I & CD4 downregulator | Nef |
| Clinical latency duration | Average 8-10 years |
| AIDS-defining CD4 cut-off | <200 cells/μL |
| Daily viral production | ~10 billion particles |
| Most common severe eye OI | CMV retinitis |
| Kaposi Sarcoma cofactor | HHV-8 |
| Anti-HIV Ab that persists longest | Anti-gp120/gp41/gp160 (envelope) |
| Anti-HIV Ab that declines with progression | Anti-p24 |
| Best prognostic marker | Plasma viral load |
| Resistance testing method | HIV genotyping (RT + protease sequencing) |
| Window period | ~3-4 weeks (seroconversion); most +ve by 6-12 weeks |
| Mechanism of AZT | NRTI - chain terminator |
| Preferred 1st-line ART backbone | 2 NRTIs + INSTI |
| HIV-TB risk increase | 20-fold |
| Vaccine status | No effective vaccine |
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology 28th ed. (Chapter 44) - aligned with Apurba S. Sastry's Essentials of Medical Microbiology
This is a shared conversation. Sign in to Orris to start your own chat.