Detailed note on mammady gland with diagram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the content needed to write a comprehensive, well-illustrated note. Let me compile everything.
Mammary Gland - Detailed Notes
1. Introduction and Embryology
The mammary gland is a modified apocrine sweat gland of ectodermal origin, unique to mammals, designed to synthesize and secrete milk (lactation) for neonatal nutrition.
Embryological development: Mammary glands develop as epidermal (ectodermal) invaginations along two ventral lines called the milk lines (mammary ridges), which run from the axillae to the groin. In humans, one pair of glands persists on each side of the chest; the rest of the milk-line tissue normally regresses. Failure of regression results in accessory/supernumerary nipples (polythelia) or accessory breasts (polymastia).
- Junqueira's Basic Histology, 17e
2. Gross Anatomy and Location
- Situated in the superficial fascia (subcutaneous tissue) overlying the pectoralis major muscle, between the 2nd and 6th ribs, from the sternum to the mid-axillary line
- The axillary (axillary tail of Spence) process extends superolaterally along the inferior border of pectoralis major into the axilla
- Surrounded by a fibrous capsule; Cooper's ligaments (suspensory ligaments) are condensations of fibrous tissue connecting the skin to the underlying fascia, giving the breast structural support
Diagram 1 - Mammary Gland Structure
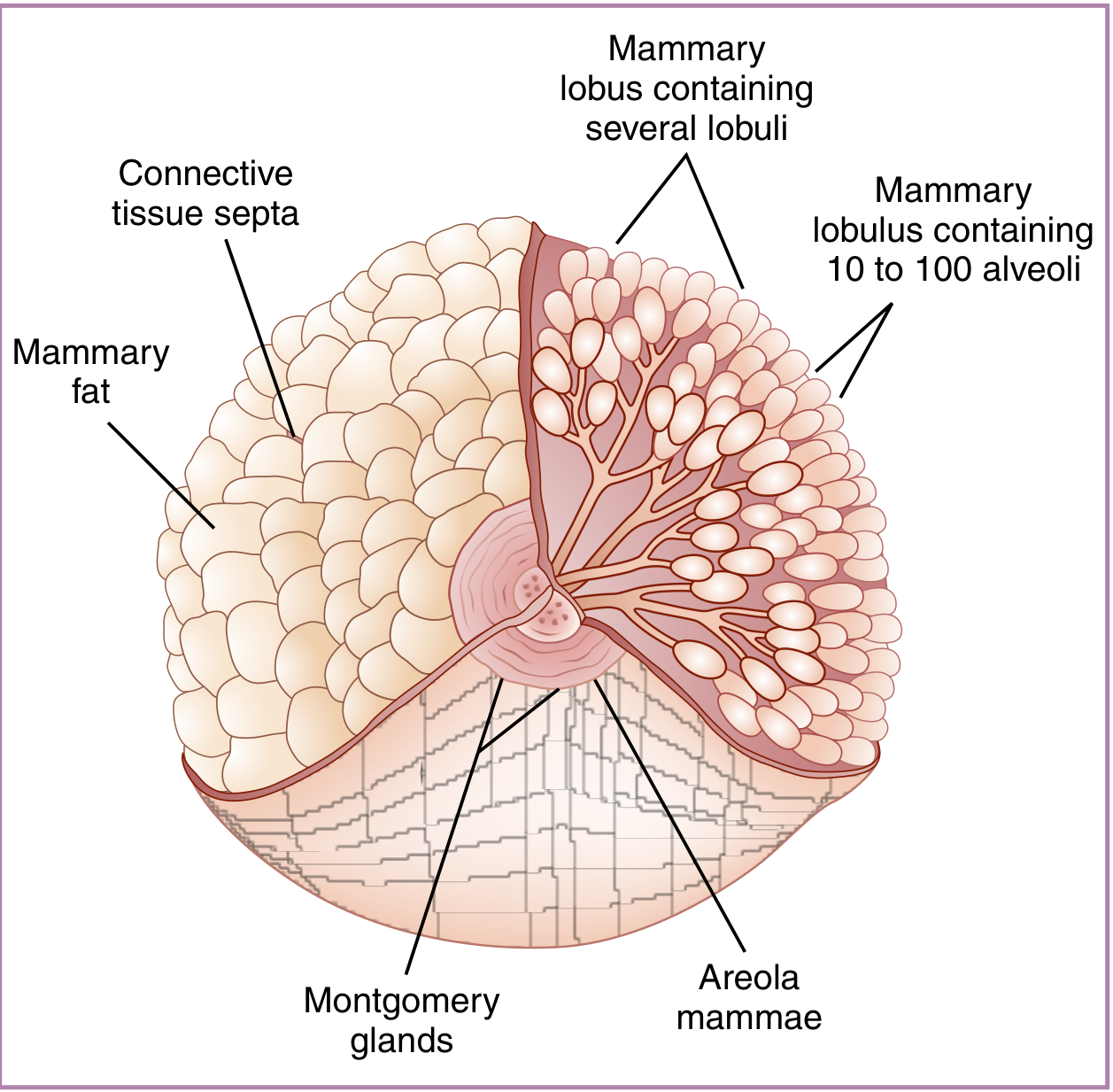
Figure: Morphology of the mature breast. The mammary lobus contains several lobuli, each containing 10-100 alveoli. Connective tissue septa separate the lobes, surrounded by mammary fat. Montgomery glands are visible on the areola mammae. (From Creasy & Resnik's Maternal-Fetal Medicine)
3. Structural Organization
Each mammary gland is a compound tubuloacinar gland made up of:
Lobes (15-20 per breast)
- Each lobe is a distinct gland separated from others by dense connective tissue and adipose tissue
- Each lobe drains into its own lactiferous duct (4-18 per nipple, 5-8 are main ducts)
- The lactiferous ducts converge at the nipple, each opening independently at the tip
Lobules (Terminal Duct Lobular Units - TDLUs)
- Each lobe is subdivided into smaller lobules (also called TDLUs)
- Each lobule contains several branching terminal ducts with attached secretory alveoli (acini)
- In the non-pregnant state, alveoli are small and undeveloped
- During lactation, each lobule may contain 10-100 active alveoli
Duct System (proximal to distal)
| Level | Lining | Notes |
|---|---|---|
| Lactiferous sinuses | Stratified cuboidal epithelium | Dilated beneath nipple |
| Lactiferous ducts | Simple cuboidal + myoepithelial cells | Major collecting ducts |
| Terminal ducts | Simple cuboidal + myoepithelial cells | Open into lobules |
| Alveoli (acini) | Simple cuboidal/columnar + myoepithelial cells | Secretory units |
- Histology: A Text and Atlas, Lippincott (9781975181512)
4. Nipple and Areola
-
Nipple: Contains 4-18 lactiferous duct openings; rich in smooth muscle fibers (causes erection) and abundant sensory nerves (branches of 4th-6th intercostal nerves). The connective tissue is rich in smooth muscle running parallel to the lactiferous sinuses.
-
Areola: Surrounding pigmented skin averaging 15-16 mm diameter (enlarges in pregnancy). Contains Montgomery glands - modified sebaceous/sweat glands that hypertrophy in pregnancy and secrete sebaceous material to lubricate and protect the nipple during suckling. The areola has less sensory innervation than the nipple.
-
Areolar keratinocytes contain more melanin than surrounding skin; they darken further during pregnancy.
-
Creasy & Resnik's Maternal-Fetal Medicine
5. Histology - Inactive (Resting) Gland
In the non-pregnant adult female:
- Parenchyma is sparse; largely duct elements with small, undeveloped alveoli
- Surrounded by loose intralobular connective tissue (contains fibroblasts, lymphocytes, plasma cells, mast cells)
- Separated from adjacent lobules by dense interlobular connective tissue containing adipocytes
- The entire gland is mostly composed of adipose tissue with limited glandular tissue
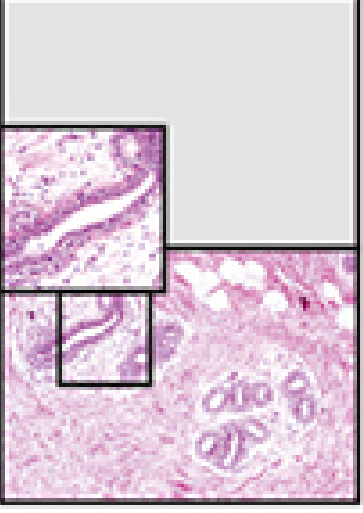
Figure: Inactive mammary gland - H&E section. Ducts (D) are visible within loose intralobular connective tissue (CT/L). Dense interlobular connective tissue (CT/D) contains adipocytes (A). Lymphocytes (L) and plasma cells (P) populate the loose connective tissue. (From Histology: A Text and Atlas, Lippincott)
6. Developmental Changes Across Life
Diagram 2 - Sequence of Changes with Pregnancy
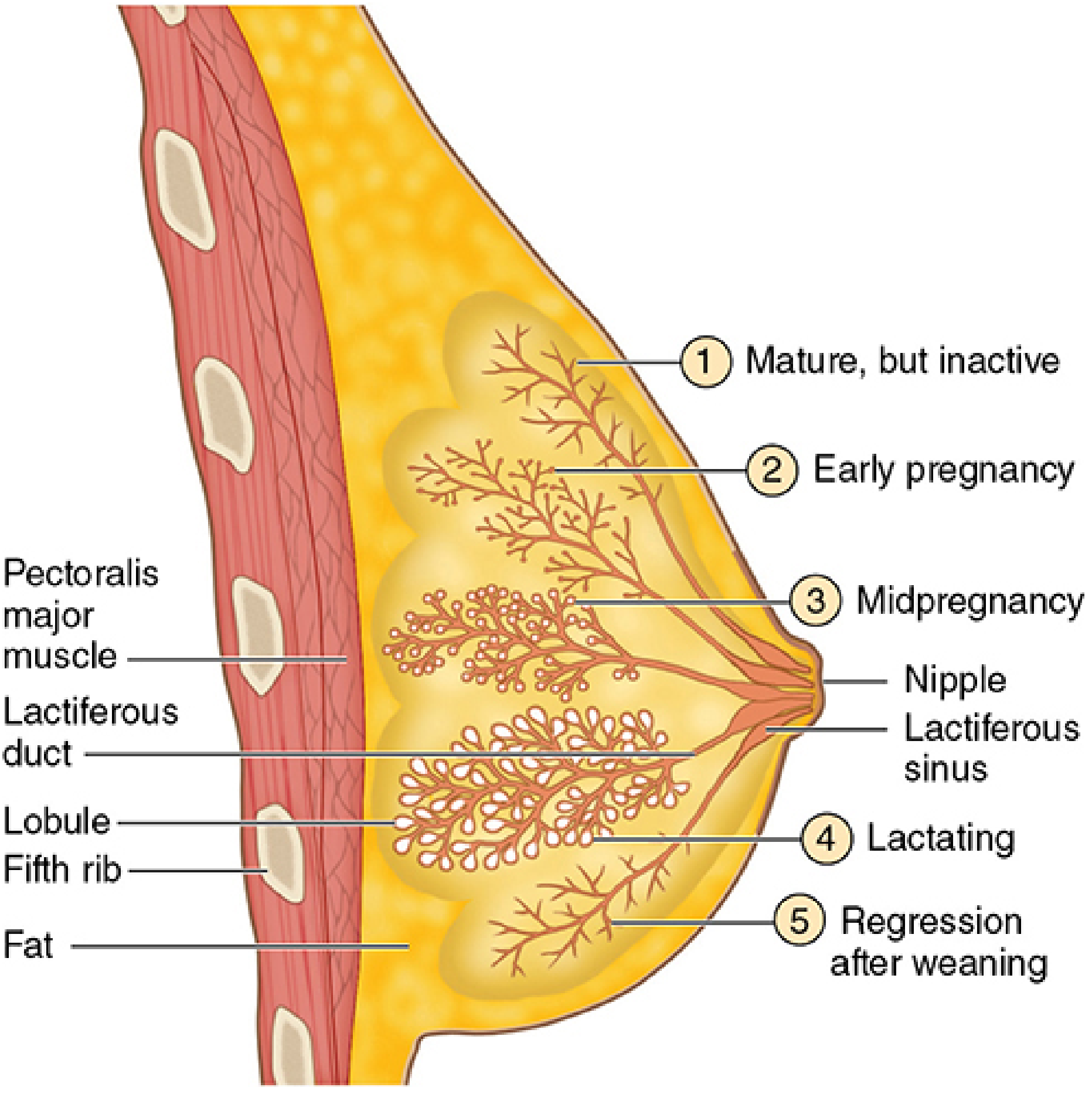
Figure: Changes in alveolar secretory units (TDLUs) before, during, and after pregnancy. 1 = Mature but inactive; 2 = Early pregnancy; 3 = Midpregnancy; 4 = Lactating; 5 = Regression after weaning. (From Junqueira's Basic Histology, 17e)
Before Puberty
- Both sexes: only lactiferous sinuses near the nipple with small branching ducts
- Glandular tissue is minimal
At Puberty (Female)
- Estrogen stimulates: accumulation of new adipocytes, elongation of the duct system
- Lobules form with branching ducts and small, rudimentary acinar secretory units
- The TDLU becomes the functional unit
Non-pregnant Adult
- Gland inactive; slight cyclic changes parallel the menstrual cycle:
- Follicular phase: Estrogen stimulates lactiferous duct proliferation
- Luteal phase: Progesterone stimulates alveolar growth; intralobular stroma becomes edematous (causing breast tenderness/fullness premenstrually)
During Pregnancy
Synergistic action of estrogen, progesterone, prolactin (PRL), and human chorionic somatomammotropin (hCS/placental lactogen):
- Massive proliferation of TDLUs
- Alveoli develop extensive dilated lumens
- Glandular tissue replaces much of the adipose tissue
- Alveolar epithelium prepares for secretory activity
Lactation
- Alveoli maximally dilated and active
- Colostrum is secreted in the first few days post-partum: alkaline, yellowish, protein-rich, contains secretory IgA providing passive immunity to the newborn; lower in fat than mature milk
- After colostrum, lipid-rich milk is produced
After Menopause
- Without ovarian hormones, secretory cells of TDLUs degenerate and disappear
- Leaves only ducts - resembles the male breast histologically
- Connective tissue degenerates: reduced fibroblasts, collagen, elastic fibers
7. Secretory Mechanisms
Mammary epithelial cells use two secretory pathways:
| Pathway | Component Secreted | Mechanism |
|---|---|---|
| Merocrine (exocytosis) | Proteins (caseins, whey proteins) | Synthesized in rER → packaged in Golgi vesicles → exocytosed at apical surface |
| Apocrine secretion | Lipids (fat droplets) | Lipid droplets accumulate in cytoplasm → migrate to apex → bud off invested in a plasma membrane envelope |
- Histology: A Text and Atlas, Lippincott
8. Milk Ejection Reflex (Neuroendocrine)
Suckling → sensory impulses from nipple → hypothalamus:
- Inhibits dopamine (prolactin-inhibiting factor) → anterior pituitary releases Prolactin (PRL) → stimulates milk synthesis
- Releases Oxytocin from posterior pituitary → stimulates myoepithelial cells surrounding alveoli and ducts → contraction → milk ejection ("let-down reflex")
In the absence of suckling, milk secretion ceases and the gland regresses.
Lactational amenorrhea: High PRL suppresses pulsatile GnRH, which suppresses LH, inhibiting ovulation. Approximately 50% of exclusively breastfeeding females experience this effect, typically for up to 6 months.
9. Blood Supply
| Vessel | Territory |
|---|---|
| Internal thoracic artery (internal mammary) | Medial breast (major supply) |
| Lateral thoracic artery | Lateral breast (major supply) |
| Anterior intercostal arteries | Additional supply |
| Thoracic branches of axillary artery | Upper breast |
Veins follow the arteries, draining to axillary and internal thoracic veins.
10. Lymphatic Drainage (Clinically Important)
- Axillary lymph nodes - drain the lateral, upper outer, and lower outer quadrants (majority of lymph, ~75%)
- Parasternal (internal mammary) nodes - drain medial quadrants along the internal thoracic artery within the thorax
- Supraclavicular nodes - less common pathway
Clinical note: Lymphatic drainage is critical in breast cancer staging. Sentinel lymph node biopsy assesses axillary node involvement. Axillary node clearance or radiotherapy can disrupt lymphatic drainage of the upper limb, causing lymphedema. - Gray's Anatomy for Students
11. Nerve Supply
- Anterior and lateral cutaneous branches of intercostal nerves 2-6 supply the breast
- 4th intercostal nerve provides the principal sensory supply to the nipple and areola
- Autonomic (sympathetic adrenergic) fibers travel with arteries; no parasympathetic or cholinergic fibers supply any part of the breast
- The secretory function of the gland is primarily under hormonal control; afferent impulses from suckling trigger the PRL/oxytocin reflex arcs
- Myoepithelial cells have no direct innervation; they respond to oxytocin
12. Hormonal Regulation Summary
| Hormone | Source | Effect on Mammary Gland |
|---|---|---|
| Estrogen | Ovary/Placenta | Duct proliferation and elongation |
| Progesterone | Corpus luteum/Placenta | Lobular/alveolar growth |
| Prolactin (PRL) | Anterior pituitary | Milk synthesis; required for gland growth |
| hCS (placental lactogen) | Placenta | Assists PRL in gland growth during pregnancy |
| Oxytocin | Posterior pituitary | Myoepithelial contraction → milk ejection |
| Glucocorticoids | Adrenal cortex | Permissive role in gland development |
| GH | Anterior pituitary | Supports overall breast growth |
13. Male Mammary Gland
- Present but vestigial
- Develops at puberty to a limited, stabilized state
- Consists mainly of duct elements without developed lobular/alveolar units
- Gynecomastia = abnormal male breast enlargement due to excess estrogen relative to androgens (e.g., liver disease, medications, Klinefelter syndrome)
Summary Table
| Feature | Details |
|---|---|
| Type | Modified apocrine sweat gland; compound tubuloacinar |
| Origin | Ectoderm (epidermis), milk lines |
| Number of lobes | 15-20 per breast |
| Functional unit | Terminal Duct Lobular Unit (TDLU) |
| Secretory cell type | Simple cuboidal/columnar epithelium |
| Supporting cell | Myoepithelial cells (surround alveoli and ducts) |
| Secretory mechanism | Merocrine (protein) + Apocrine (lipid) |
| Main blood supply | Internal thoracic artery + lateral thoracic artery |
| Lymph drainage | Axillary nodes (75%) + parasternal nodes |
| Nerve supply | 2nd-6th intercostal nerve branches |
| Milk ejection trigger | Oxytocin (posterior pituitary) via suckling reflex |
| Milk production trigger | Prolactin (anterior pituitary) |
Sources:
- Junqueira's Basic Histology, 17e - Chapter 22 (MAMMARY GLANDS)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Lippincott) - Plates 23.11 & 23.12; Hormonal Regulation section
- Creasy & Resnik's Maternal-Fetal Medicine - Chapter 11 (Nipple, Areola, and Breast Morphology)
- Gray's Anatomy for Students - Axillary process and lymphatic drainage
Retailed anatomy on mammary gland with 2-3 diagrams
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have three excellent diagrams and comprehensive anatomy content from multiple authoritative sources. Here is the detailed anatomical note:
Detailed Anatomy of the Mammary Gland
1. Position and Surface Anatomy
The mammary gland (breast) is located in the pectoral region on each side of the anterior thoracic wall, lying within the superficial fascia (subcutaneous tissue). Key surface landmarks:
- Vertical extent: 2nd to 6th rib
- Horizontal extent: Lateral border of the sternum to the mid-axillary line
- The base (attached surface) rests on deep fascia overlying the pectoralis major (mainly), with smaller areas over serratus anterior and the external oblique
- The axillary tail (tail of Spence) - the superolateral extension of the gland passes along the inferior border of pectoralis major and may penetrate deep fascia to enter the axilla
The breast is a modified apocrine sweat gland of ectodermal origin - a compound tubuloacinar gland.
- Gray's Anatomy for Students
2. Fascial Relations
Diagram 1 - Cutaway Anatomy of the Mature Breast
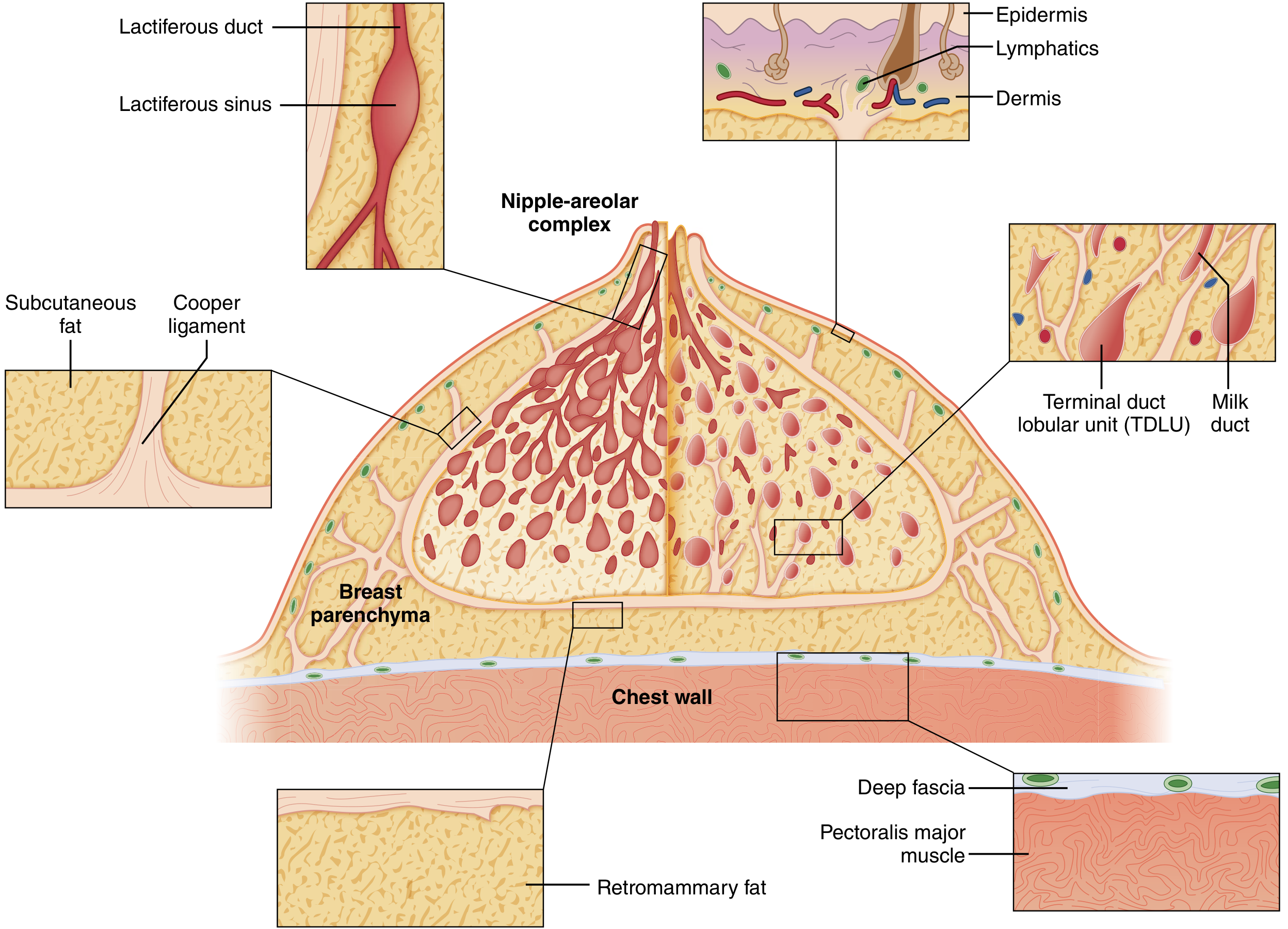
Figure 68.1: Cutaway diagram of a mature resting breast. The breast lies cushioned in fat between the overlying skin and pectoralis major muscle. Cooper ligaments fuse with the superficial fascia just under the dermis, coalesce as interlobular fascia in the breast parenchyma, and join the deep fascia over pectoralis muscle. The duct system resembles an inverted tree, largest just under the nipple, successively smaller toward the periphery, ending in the terminal duct lobular units. (Sabiston Textbook of Surgery, 21e)
The breast has three layers from anterior to posterior:
| Layer | Contents |
|---|---|
| Skin + subcutaneous fat | Epidermis, dermis, subdermal lymphatics, subcutaneous fat |
| Breast parenchyma (in superficial fascia) | Glandular tissue (15-20 lobes), fibrous stroma, Cooper's ligaments, adipose tissue, blood vessels, lymphatics |
| Retromammary space | Loose areolar connective tissue (allows breast mobility over deep fascia) |
| Deep fascia | Investing fascia of pectoralis major below |
Cooper's Ligaments (Suspensory Ligaments of the Breast)
-
Fibrous condensations of connective tissue that pass from the overlying skin dermis through the breast parenchyma to the deep fascia
-
They fuse with the superficial fascia just under the dermis, coalesce as interlobular fascia within the parenchyma, and join the deep fascia over pectoralis major
-
They support the breast against gravity and maintain its shape
-
Clinical significance: Breast carcinoma invading Cooper's ligaments causes contraction → characteristic skin dimpling/pitting - a sign of malignancy. Blockage of superficial lymphatics by carcinoma cells gives the "peau d'orange" (orange-peel) appearance.
-
Sabiston Textbook of Surgery; Gray's Anatomy for Students
3. Structural Organization of the Glandular Tissue
Diagram 2 - Lobular Architecture and Surface Anatomy
Figure: Anterior view of the mature breast. Each mammary lobus contains several lobuli; each lobulus contains 10-100 alveoli. Connective tissue septa separate the lobes, surrounded by mammary fat. Montgomery glands are visible on the areola mammae. (From Creasy & Resnik's Maternal-Fetal Medicine)
The mature breast is composed of three principal tissue types:
- Glandular epithelium - ducts and secretory lobules
- Fibrous stroma - interlobular (dense) and intralobular (loose, specialized)
- Adipose tissue - constitutes the majority of the breast volume in non-lactating women
Lobes (15-20)
- Each lobe is a functionally independent gland separated from others by dense interlobular connective tissue and adipose tissue
- Each lobe drains into one lactiferous duct that opens independently at the nipple tip
- Lobes are arranged in a radial pattern spreading outward from the nipple-areolar complex (NAC)
- There is no cross-communication between independent duct systems
Lobules / Terminal Duct Lobular Units (TDLUs)
- The functional unit of the breast
- Each lobe is subdivided into multiple lobules (TDLUs)
- Each TDLU consists of multiple branching terminal ductules, each ending blindly in an acinus (alveolus) - the milk-forming gland
- Each lobule contains 10-100 alveoli (active during lactation)
- TDLUs are surrounded by specialized loose intralobular stroma containing capillaries, lymphocytes, and plasma cells - clearly distinct from the denser, less cellular interlobular stroma
Duct System - "Inverted Tree" Architecture
| Level | Structure | Lining |
|---|---|---|
| Most distal | Acini (secretory alveoli) | Simple cuboidal/columnar + myoepithelial cells |
| Terminal ductules | Intralobular ducts | Simple cuboidal + myoepithelial cells |
| Segmental ducts | Extralobular ducts | Simple cuboidal + myoepithelial cells |
| Lactiferous ducts | Main collecting ducts | Simple cuboidal + myoepithelial cells |
| Lactiferous sinuses | Dilated ampullae below NAC | Stratified cuboidal epithelium |
| Nipple orifices | 4-18 openings at nipple tip | Stratified squamous |
The entire ductal system is lined by epithelial cells surrounded by myoepithelial cells, with an outer continuous basement membrane containing laminin, type IV collagen, and proteoglycans. Invasion through this basement membrane by tumor cells converts DCIS to invasive carcinoma.
4. Nipple and Areola (Nipple-Areolar Complex, NAC)
- Nipple: Conical projection at the center of the areola; contains openings of 4-18 lactiferous ducts (5-8 are main ducts). Rich in smooth muscle fibers (circular and longitudinal - cause erection on stimulation), abundant sensory nerve endings, and dense connective tissue
- Areola: Circular pigmented skin surrounding the nipple; average diameter 15-16 mm (enlarges significantly during pregnancy). Contains Montgomery glands (tubercles of Montgomery) - specialized sebaceous/sweat hybrid glands that enlarge during pregnancy and secrete sebaceous fluid to lubricate the nipple during breastfeeding
- The areola contains less sensory innervation than the nipple itself
- Areolar keratinocytes have more melanin than adjacent skin and darken further during pregnancy
5. Blood Supply
Diagram 3 - Neurovascular Supply and Lymphatic Drainage
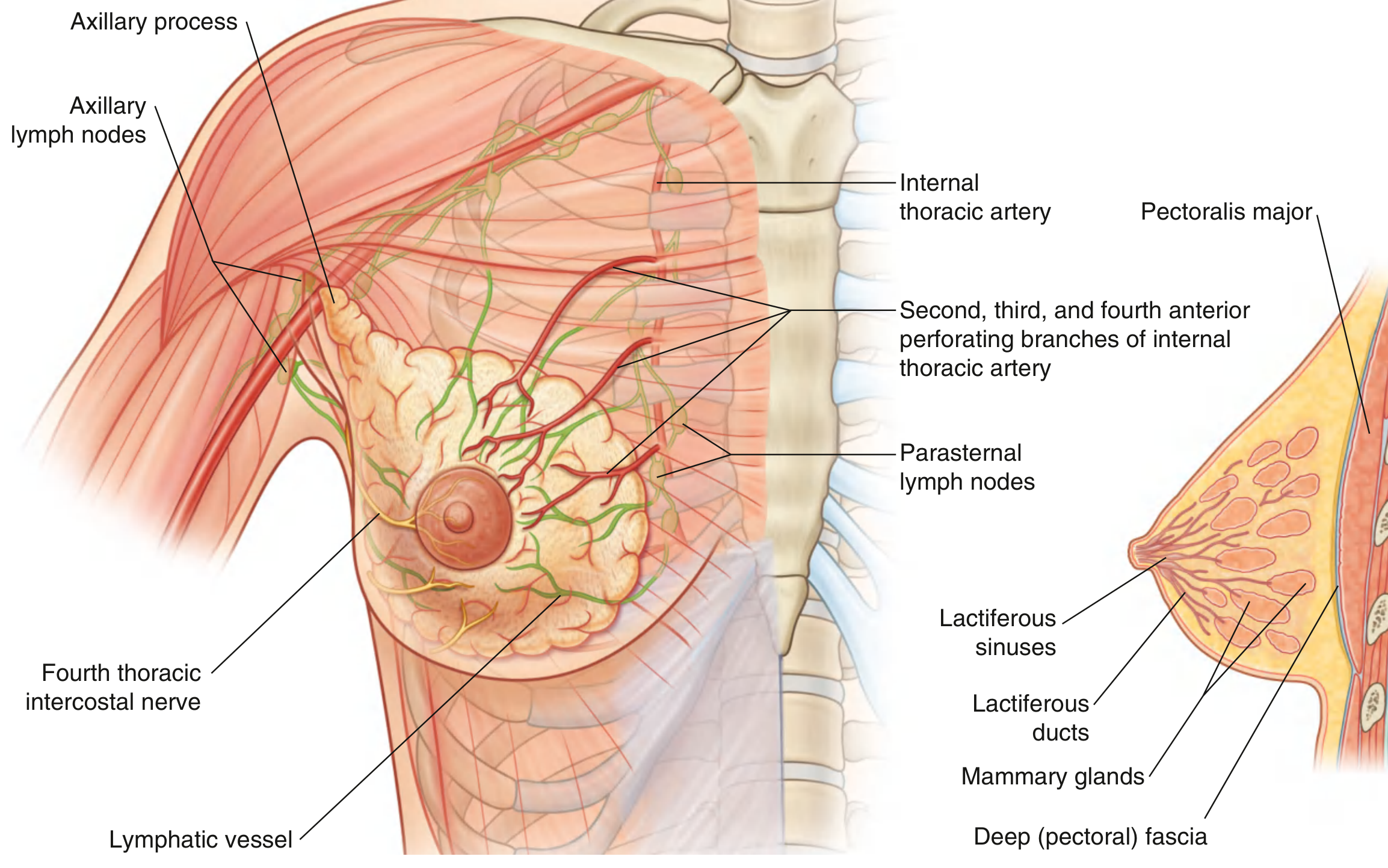
Fig. 3.9: Right breast anatomy showing arterial supply (internal thoracic artery and its perforating branches), lymphatic drainage to axillary and parasternal nodes, and nerve supply from the 4th intercostal nerve. Cross-section shows internal structure from pectoralis major through the duct system to the nipple. (Gray's Anatomy for Students)
The breast receives blood from three main sources:
| Artery | Territory Supplied |
|---|---|
| Internal thoracic artery (internal mammary) | Medial breast via 2nd-4th anterior perforating branches (major supply) |
| Lateral thoracic artery (branch of axillary) | Lateral and upper breast (major supply) |
| Thoraco-acromial artery (branch of axillary) | Upper breast |
| Subscapular artery (branch of axillary) | Variable |
| 2nd-4th intercostal arteries | Posterior perforating branches |
Vessels run primarily along the paths of the alveolar ducts, reaching capillary beds around the alveoli.
Venous drainage: Veins parallel the arteries, draining into:
- Axillary vein
- Internal thoracic vein
- Intercostal veins
6. Lymphatic Drainage (Critical Clinically)
Lymphatic channels are abundant in both the breast parenchyma and dermis. The Sappey's subareolar plexus collects lymphatics from the skin/nipple area; lymph flows from skin → subareolar plexus → interlobular lymphatics of parenchyma.
| Pathway | Proportion | Destination |
|---|---|---|
| Axillary nodes (main pathway) | 70-80% | Lateral, upper, and lower outer quadrants drain here |
| Internal mammary (parasternal) nodes | ~20% (secondary); 2-3% primary | Medial quadrants; along internal thoracic artery |
| Interpectoral nodes (Rotter's nodes) | Small % | Through pectoralis muscle to deeper nodes |
| Supraclavicular nodes | Terminal drainage | Beyond level III axillary nodes |
| Intercostal nodes | Minor | Via lateral intercostal branches |
Axillary Lymph Node Levels (defined by relation to pectoralis minor)
| Level | Location | Clinical Note |
|---|---|---|
| Level I | Lateral to lateral border of pectoralis minor | First station in sentinel node biopsy |
| Level II | Posterior to pectoralis minor + Rotter's (interpectoral) nodes | |
| Level III | Medial to pectoralis minor; infraclavicular nodes | Clearance to here = full axillary dissection |
Clinical significance: Axillary node clearance or radiotherapy (for breast cancer) damages lymphatics of the upper limb → lymphedema of the arm. Sentinel lymph node biopsy identifies the first draining node to assess spread with minimal disruption.
7. Nerve Supply
- Anterior and lateral cutaneous branches of intercostal nerves 2-6 - provide general somatic sensation to the breast skin
- 4th intercostal nerve - principal sensory supply to the nipple and areola (most important nerve for nipple sensation)
- Autonomic (sympathetic adrenergic) efferents - travel with arteries; supply blood vessels and smooth muscle of the nipple. No parasympathetic supply to any part of the breast
- Myoepithelial cells have no direct innervation; they respond to circulating oxytocin during the milk ejection reflex
- Secretory function of the gland is under hormonal (not neural) control; suckling triggers the neuroendocrine oxytocin/prolactin reflex arcs via afferent impulses through the 4th intercostal nerve
8. Structural Summary Table
| Feature | Details |
|---|---|
| Location | Superficial fascia, 2nd-6th rib, sternum to mid-axillary line |
| Underlying muscle | Pectoralis major (mainly); serratus anterior, external oblique |
| Fascial plane | Retromammary space (loose CT) separates breast from deep fascia |
| Type | Compound tubuloacinar; modified apocrine sweat gland |
| Lobes | 15-20 per breast; each drains via 1 lactiferous duct |
| Functional unit | TDLU (terminal duct lobular unit / lobule) |
| Alveoli per lobule | 10-100 |
| Supportive ligaments | Cooper's ligaments (superficial fascia to deep fascia) |
| Nipple orifices | 4-18 lactiferous ducts (5-8 main) |
| Arterial supply | Internal thoracic + lateral thoracic arteries (main) |
| Lymph drainage | 70-80% axillary; ~20% internal mammary nodes |
| Axillary node levels | I (lateral), II (posterior/Rotter's), III (medial/infraclavicular) |
| Nerve supply | Intercostal nerves 2-6; 4th = nipple/areola |
| Autonomic | Sympathetic adrenergic only; no parasympathetic |
Sources:
- Gray's Anatomy for Students - Chapter 3 (Breast anatomy, Fig. 3.9, 3.16)
- Sabiston Textbook of Surgery, 21e - Chapter 68 (Breast Anatomy, Figs. 68.1-68.4)
- Creasy & Resnik's Maternal-Fetal Medicine - Chapter 11 (Breast morphology)
- Histology: A Text and Atlas (Lippincott) - Chapter 23 (Mammary gland plates)
This is a shared conversation. Sign in to Orris to start your own chat.