Stemi
Reading File
Finding Sources
Searching PubMed
"ST-elevation myocardial infarction" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have extensive material to compile a comprehensive response. Let me put it all together.
ST-Elevation Myocardial Infarction (STEMI)
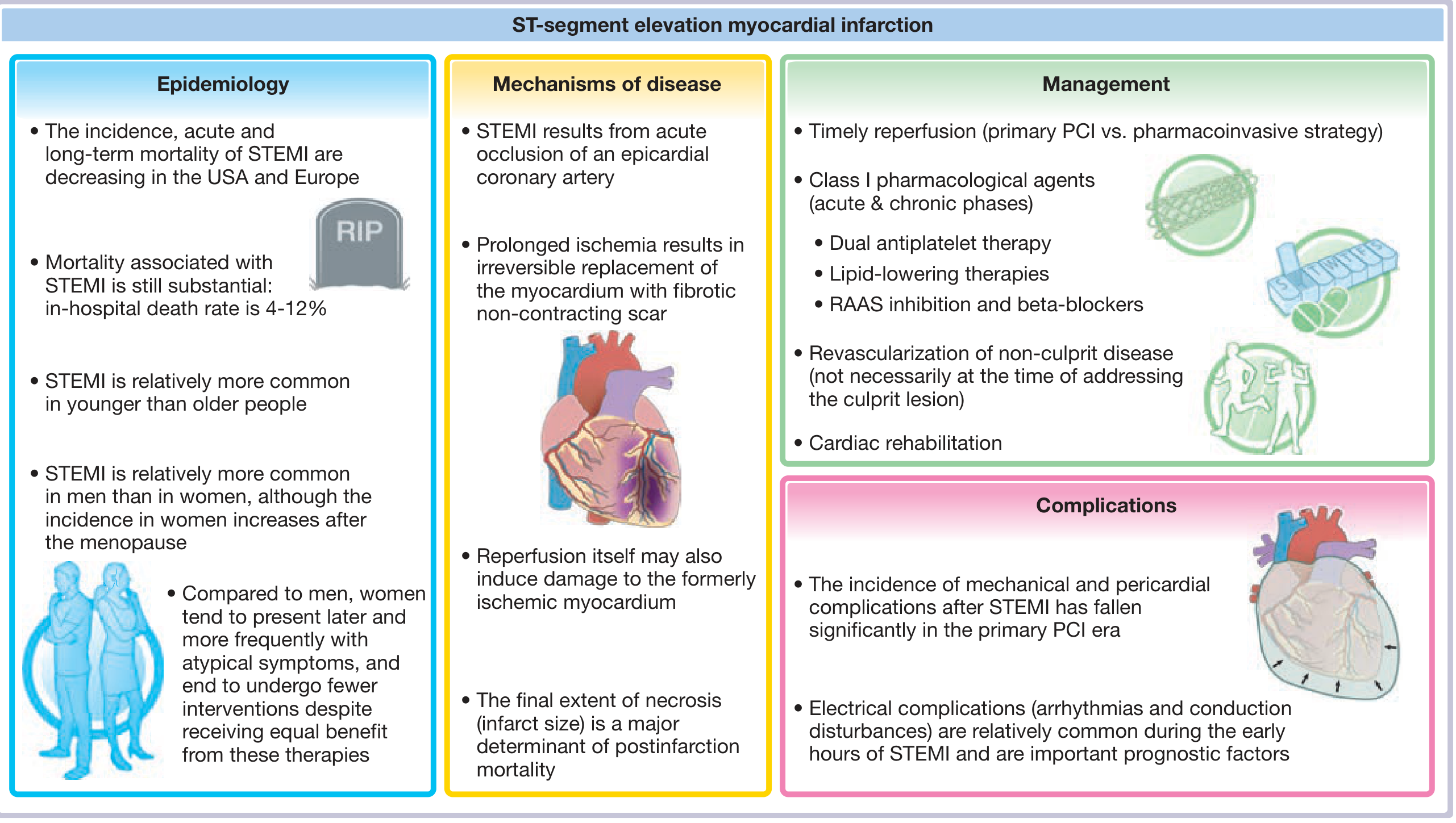
Definition and Pathophysiology
STEMI is an acute MI caused by complete occlusion of an epicardial coronary artery, producing transmural (full-thickness) ischemia. The most common mechanism is rupture of an atherosclerotic plaque, triggering thrombosis that blocks the vessel. Prolonged ischemia leads to irreversible replacement of myocardium with fibrotic, non-contracting scar. The final infarct size is a major determinant of post-infarction mortality.
- Symptom to Diagnosis: An Evidence Based Guide, p. 174
- Fuster and Hurst's The Heart, 15th Ed., p. 599
Classification of MI (Universal Definition)
| Type | Description |
|---|---|
| Type 1 | Spontaneous MI from primary coronary event (plaque rupture) |
| Type 2 | Secondary ischemia (increased O2 demand or decreased supply - spasm, anemia, arrhythmia) |
| Type 3 | Sudden cardiac death with ECG/angiographic/autopsy evidence |
| Type 4 | MI associated with PCI or stent thrombosis |
| Type 5 | MI associated with CABG |
STEMI vs NSTEMI:
- STEMI: Transmural ischemia, typically from complete occlusion
- NSTEMI: Subendocardial injury, typically from incomplete occlusion; carries a higher subsequent risk for STEMI than vice versa
ECG Diagnostic Criteria
ECG must be obtained and interpreted within 10 minutes of arrival when MI is suspected.
STEMI criteria (new or presumed new):
- ST elevation at the J-point in ≥2 contiguous leads > 1 mm (in all leads except V2-V3)
- In V2-V3: ≥2 mm in men <40 years, or ≥1.5 mm in women
- New (or presumed new) left bundle branch block (LBBB)
Reciprocal ST depression in opposite leads helps confirm the diagnosis.
Diagnostic yield of ECG findings in ED chest pain patients:
-
New ST elevation of 1 mm: ~80% probability of MI
-
New ST depression or T-wave inversion: ~20% probability
-
Symptom to Diagnosis: An Evidence Based Guide, pp. 173-174
Reperfusion - The Core of Management
Timely reperfusion has reduced in-hospital STEMI mortality from ~20% to 4-12% over three decades.
Primary PCI (pPCI) - Preferred Strategy
- Superior to fibrinolysis for reducing death, reinfarction, and stroke (meta-analysis of 23 RCTs)
- Time target: Symptom onset to wire crossing (culprit artery) ≤120 minutes to choose pPCI over fibrinolysis
- AHA/ACC target: "First medical contact to device" time ≤90 min at a PCI-capable hospital, or ≤120 min if transfer is required
- Each 30-minute delay in treatment increases morbidity and mortality
Fibrinolytic Therapy - When PCI is Not Available in Time
- Give within 30 minutes of ED arrival if PCI cannot be accomplished within the time targets
- Administer within 10 minutes of STEMI diagnosis (prehospital administration is feasible and safe)
- Fibrin-specific agents (alteplase, tenecteplase, reteplase) are preferred over streptokinase
- Efficacy decreases as time from symptom onset elapses (thrombi "mature" and become harder to lyse)
- Reperfusion is recommended for presentations within 12 hours of symptom onset; benefit is limited beyond 48 hours
Fibrinolytic Dosing (Selected Agents)
| Agent | Dose |
|---|---|
| Alteplase | 15 mg IV bolus → 0.75 mg/kg over 30 min → 0.5 mg/kg over 60 min |
| Tenecteplase | Weight-based: 30 mg (<60 kg) to 50 mg (≥90 kg) IV bolus |
| Reteplase | 10 units IV over 2 min, then 10 units 30 min later |
| Streptokinase | 1.5 million units over 60 min |
- Tintinalli's Emergency Medicine, p. 385; Fuster and Hurst's The Heart, 15th Ed., p. 605
Pharmacotherapy
Antiplatelets (DAPT - Dual Antiplatelet Therapy)
| Drug | Loading Dose | Maintenance |
|---|---|---|
| Aspirin | 162-325 mg | 75-100 mg daily (indefinitely) |
| Clopidogrel | 600 mg PO | 75 mg daily |
| Ticagrelor | 180 mg PO | 90 mg twice daily |
| Prasugrel | 60 mg PO (at time of PCI, once anatomy defined) | 10 mg daily |
DAPT (aspirin + a P2Y12 antagonist) is recommended for 12 months after STEMI, absent high bleeding risk. Ticagrelor and prasugrel are preferred over clopidogrel for most patients. - Harrison's Principles of Internal Medicine, 22nd Ed., p. 1494
Anticoagulants
| Drug | Dose |
|---|---|
| Unfractionated heparin (UFH) | 60 units/kg IV bolus (max 4000 U), then 12 units/kg/h, titrate aPTT to 1.5-2.5x control |
| Enoxaparin | 30 mg IV bolus + 1 mg/kg SC q12h |
| Fondaparinux | 2.5 mg SC daily |
| Bivalirudin | Acceptable alternative to UFH at time of PCI |
Other Pharmacological Agents
- Beta-blockers: Start early unless risk for cardiogenic shock (heart failure signs, BP <120, HR >110 or <60, AV block, active asthma). Hold if any risk factors present.
- RAAS inhibition (ACE inhibitor or ARB): Initiate especially with reduced LVEF, anterior MI, or heart failure
- Statins (high-intensity): Initiate early for all STEMI patients
- Nitrates: Sublingual 0.4 mg q5 min x3 PRN pain; IV nitroglycerin for ongoing ischemia/hypertension
- Morphine: 2-5 mg IV q5-15 min PRN pain
Multivessel Disease
- In hemodynamically stable STEMI, complete revascularization of non-culprit lesions is recommended (though not necessarily at the time of primary PCI)
- In STEMI with cardiogenic shock, multivessel PCI at the time of the index procedure generally does not improve outcomes compared to culprit-only PCI
Complications
Pericarditis
- Early pericarditis: Pleuritic chest pain, pericardial rub, typical ECG changes after STEMI - treat with aspirin (650 mg QID) + colchicine
- Dressler syndrome (late, immune-mediated): Occurs 1-2 weeks post-STEMI; same treatment
- Anticoagulants should be avoided with active pericarditis (risk of tamponade)
Mechanical Complications (Free wall rupture, VSD, Papillary muscle rupture)
- Incidence ~0.27% in the pPCI era but 42% mortality
- Suspect with: sudden hypotension, recurrent chest pain, new systolic murmur, pulmonary congestion, JVD
- Require urgent surgical intervention
Electrical Complications
- Atrial fibrillation: Up to 21% of STEMI patients; treat with beta-blocker or amiodarone for rate/rhythm control + anticoagulation
- VT/VF: 6-8% of patients; treat with reperfusion, cardioversion/defibrillation, beta-blockers, amiodarone (or lidocaine if amiodarone contraindicated)
- VT/VF within 48 hours: low long-term arrhythmic risk
- VT/VF after 48 hours (without recurrent ischemia): worse prognosis, evaluate for ICD
Thromboembolism
- Clinically apparent in ~10% (silent in 20% at autopsy); contributes to ~25% of in-hospital deaths
- LV mural thrombus (common with large anterior MIs): anticoagulate for 3-6 months if demonstrated
LV Aneurysm
- Complications: HF, arterial embolism, ventricular arrhythmias
- Pseudoaneurysm (contained rupture) should be surgically repaired when recognized
Post-Discharge and Secondary Prevention
- Continue DAPT for 12 months; consider de-escalation or shortening based on bleeding vs ischemic risk
- Dual-pathway inhibition (aspirin + low-dose rivaroxaban) for chronic phase in selected patients
- Beta-blocker, statin, ACE inhibitor/ARB continued long-term
- Cardiac rehabilitation
- Smoking cessation, blood pressure and glycaemic control
2025 ACC/AHA Guideline update: The 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of ACS (PMID 40013746) was published in June 2025 and represents the most current evidence-based recommendations for STEMI. Key updates address antithrombotic strategies, timing of revascularization, and post-discharge care.
Sources: Fuster and Hurst's The Heart, 15th Ed. | Tintinalli's Emergency Medicine | Harrison's Principles of Internal Medicine, 22nd Ed. | Symptom to Diagnosis, 4th Ed. | 2025 ACC/AHA ACS Guideline (PMID 40013746)
This is a shared conversation. Sign in to Orris to start your own chat.