DEFINE DYPNOEA. DIFFERENTIATE BETWEEN CARDIAC AND RESPIRATORY ORIGIN OF DYSPNOEA
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
I have more than enough high-quality textbook content to give a thorough answer. Let me now compose the comprehensive response.
Definition of Dyspnoea
Dyspnoea (also spelled dyspnea) is defined as an uncomfortable awareness of breathing - a subjective sensation of difficult, laboured, or inadequate breathing. It is not a single sensation but a family of qualitatively distinct experiences that differ in intensity. Patients describe it variously as "tightness," "choking," "feeling unable to take a deep breath," "suffocating," "feeling unable to get enough air," or "feeling tired in the chest."
"Dyspnea, which is an uncomfortable awareness of breathing, is commonly caused by cardiovascular or pulmonary disease."
- Goldman-Cecil Medicine
Key points about the definition:
- It is subjective - there are no specific receptors or single neural pathways identified for it (unlike pain or cough)
- It is not synonymous with tachypnoea (increased rate) or hyperpnoea (increased depth); a patient can have rapid breathing without dyspnoea, and vice versa
- When the sensation is abnormal (i.e., occurring at rest or at activity levels that should not produce it), it is pathological
Special Forms of Dyspnoea
| Term | Definition |
|---|---|
| Orthopnoea | Dyspnoea that occurs or worsens on assuming the supine position |
| Paroxysmal Nocturnal Dyspnoea (PND) | Acute, severe dyspnoea awakening the patient from sleep, typically 1-2 hours after lying down |
| Bendopnea | Dyspnoea that occurs when bending forward |
| Platypnea | Dyspnoea in the upright position (suggests pulmonary vascular shunting) |
| Trepopnea | Dyspnoea in one lateral decubitus position only |
| Exertional dyspnoea | Dyspnoea triggered by physical activity |
Mechanism of Dyspnoea Pathway in Cardiac Disease
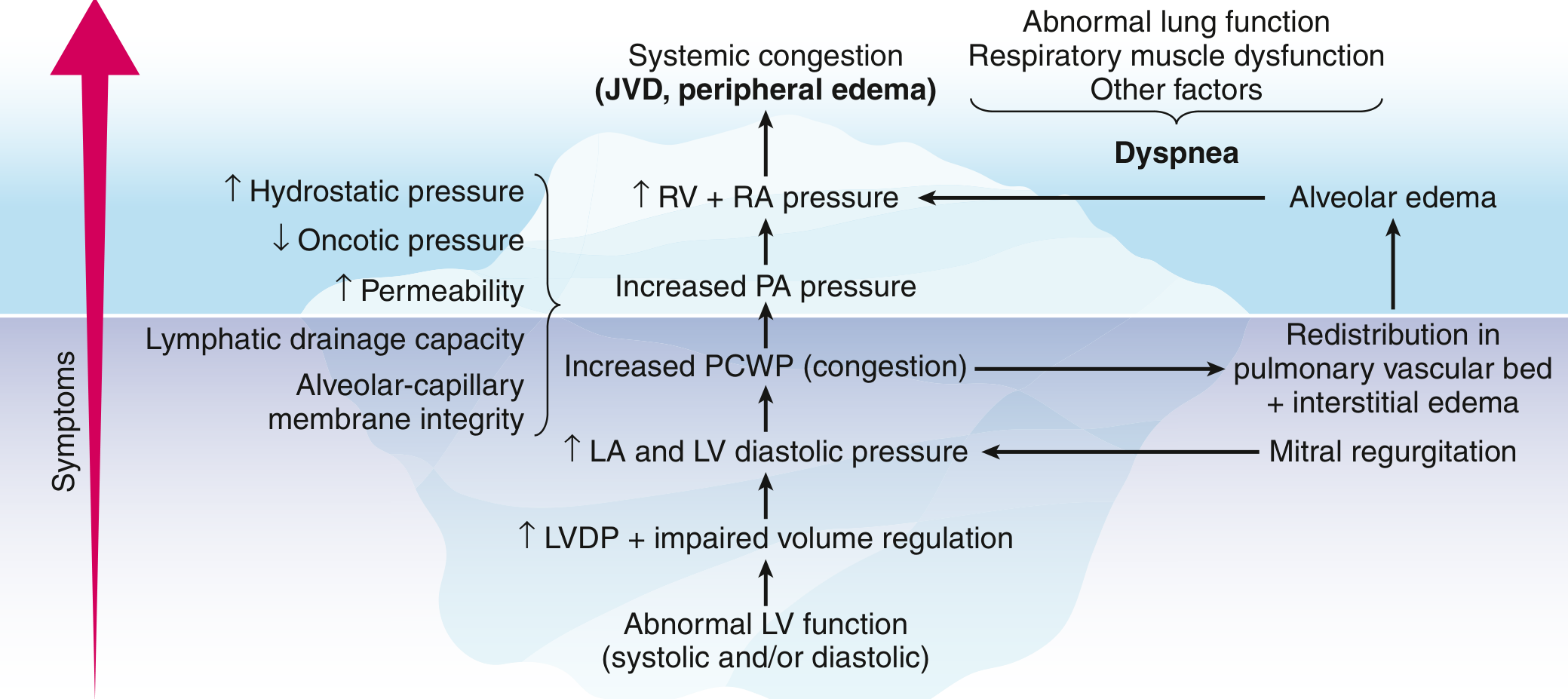
Pathway from abnormal LV function to dyspnoea in heart failure (Goldman-Cecil Medicine)
Differentiation: Cardiac vs Respiratory Dyspnoea
1. Aetiology / Underlying Causes
| Feature | Cardiac Origin | Respiratory Origin |
|---|---|---|
| Common causes | Heart failure (systolic/diastolic), ischemic heart disease, valvular disease (aortic stenosis, mitral regurgitation), arrhythmias, pericardial tamponade, hypertensive crisis | COPD, asthma, pneumonia, pulmonary embolism, pneumothorax, pleural effusion, interstitial lung disease, upper airway obstruction |
| Acute causes | Myocardial ischemia/infarction, acute pulmonary oedema, pericardial tamponade | Acute asthma, pneumothorax, massive PE |
2. History and Symptom Characteristics
| Feature | Cardiac | Respiratory |
|---|---|---|
| Quality | "Hunger for air," urge to breathe; patients describe air hunger | "Chest tightness," increased work of breathing; effort-type dyspnoea |
| Onset | Often gradual in chronic HF; may be acute with MI or acute decompensation | May be acute (asthma attack, pneumothorax) or gradual (COPD) |
| Orthopnoea | Classic and prominent - due to increased venous return raising pulmonary capillary wedge pressure (PCWP) | Present but less dominant; may occur in COPD due to secretion pooling or gravity-induced reduction in lung volumes |
| PND | Highly specific - almost always represents severe heart failure; associated with increased mortality | Can occur in chronic lung disease due to nocturnal secretion pooling or increased airflow resistance during sleep |
| Positional variation | Worse lying flat (orthopnoea); better sitting up | Less consistently positional, though tripod positioning (leaning forward) relieves work of breathing in COPD/asthma |
| Precipitants | Exertion, salt/fluid intake, non-compliance with medications | Allergens, cold air, smoke, infections, dusts, perfumes |
| Associated cough | Non-productive, dry cough or frothy pink sputum (pulmonary oedema) | Productive cough, purulent sputum in COPD/pneumonia; dry in asthma/ILD |
| Wheezing | May occur in "cardiac asthma" (pulmonary oedema mimicking asthma) | Prominent in asthma and COPD (expiratory wheeze) |
| Diurnal variation | Less prominent; can worsen at night | Asthma worse in early morning; COPD worse in morning (mucus accumulation) |
| Response to bronchodilators | Little or no relief | Significant relief in asthma and COPD |
| Response to diuretics/nitrates | Rapid and marked relief | No response |
3. Associated Symptoms
| Feature | Cardiac | Respiratory |
|---|---|---|
| Ankle oedema | Common (right heart failure) | Less common; may occur in cor pulmonale |
| Palpitations | Common (arrhythmias, tachycardia) | Less common |
| Chest pain | Angina or ischemic-type chest pain | Pleuritic chest pain (pneumonia, PE, pneumothorax) |
| Haemoptysis | Frothy pink (acute pulmonary oedema); frank in mitral stenosis | Frank haemoptysis in bronchiectasis, lung cancer, TB |
| Cyanosis | Central, peripheral (low output) | Central (hypoxaemia from V/Q mismatch) |
| Fatigue | Very prominent (>90% in HF) | Less dominant unless end-stage |
4. Physical Examination Findings
| Sign | Cardiac | Respiratory |
|---|---|---|
| Trachea | Central | Deviated in pneumothorax, tension pneumothorax |
| JVP | Elevated (right heart failure) | Elevated only if cor pulmonale develops |
| Apex beat | Displaced laterally (LV enlargement) | Normal or hyperinflated (barrel chest) |
| Heart sounds | S3 gallop (heart failure), murmurs (valvular disease), muffled (tamponade) | Normal or obscured by transmitted sounds |
| Lung auscultation | Fine bibasal crepitations (pulmonary oedema), wheeze (cardiac asthma) | Diffuse wheeze (asthma/COPD), bronchial breathing (consolidation), absent breath sounds (pneumothorax) |
| Peripheral oedema | Pitting oedema (bilateral) | Absent unless cor pulmonale |
| Clubbing | In congenital cyanotic heart disease | In bronchiectasis, lung cancer, ILD |
| Pursed lip breathing / use of accessory muscles | Not typical | Classic in COPD, severe asthma |
| Barrel chest | Absent | Present in emphysema |
5. Investigations
| Investigation | Cardiac Findings | Respiratory Findings |
|---|---|---|
| ECG | LVH, ischemic changes, arrhythmias, conduction blocks | Sinus tachycardia, right heart strain (S1Q3T3 in PE), cor pulmonale pattern |
| Chest X-ray | Cardiomegaly, upper lobe diversion, Kerley B lines, bilateral effusions, bat-wing infiltrates (pulmonary oedema) | Hyperinflation, pneumothorax, consolidation, pleural effusion, reticular-nodular pattern (ILD) |
| Echocardiogram | Reduced EF, wall motion abnormalities, valvular pathology, pericardial effusion | Normal cardiac function (unless cor pulmonale) |
| BNP/NT-proBNP | Markedly elevated - highly sensitive/specific for heart failure | Normal or mildly elevated |
| Spirometry/PFTs | Normal (unless secondary to pulmonary congestion) | Obstructive pattern (COPD, asthma) or restrictive (ILD, effusions) |
| Arterial Blood Gas | Hypoxaemia; may have respiratory alkalosis early; metabolic acidosis late | Hypoxaemia +/- hypercapnia (COPD, severe asthma); respiratory alkalosis (hyperventilation) |
| SpO2 | Reduced; improves with oxygen + diuresis | Reduces with exertion; response to oxygen varies by diagnosis |
6. Pathophysiology Summary
Cardiac Dyspnoea Mechanism:
Abnormal LV function → elevated LV diastolic pressure → increased left atrial pressure → increased pulmonary capillary wedge pressure (PCWP) → pulmonary venous hypertension → redistribution of blood in pulmonary vascular bed + interstitial oedema → reduced lung compliance → increased work of breathing → alveolar oedema → dyspnoea
- In heart failure: "The most important cause of dyspnoea is pulmonary congestion that increases the accumulation of interstitial or intra-alveolar fluid, reduces lung compliance, and increases the work of breathing." (Goldman-Cecil Medicine)
- Orthopnoea mechanism: Supine position increases venous return from extremities and splanchnic bed → raises preload → worsens PCWP
- PND mechanism: Fluid redistribution from dependent tissues back to central circulation during sleep, accumulation of alveolar oedema over 1-2 hours
Respiratory Dyspnoea Mechanism:
Airflow obstruction (bronchospasm, mucus) or parenchymal damage → increased airway resistance or reduced lung compliance → increased work of breathing + V/Q mismatch → hypoxaemia + hypercapnia → stimulation of peripheral and central chemoreceptors + mechanoreceptors in airways/lung parenchyma → dyspnoea
- The sensation of "chest tightness or constriction during breathing is typical of bronchoconstriction" (Goldman-Cecil Medicine)
- "The feeling that breathing requires increased work or effort is more typical of airway obstruction or neuromuscular disease" (Goldman-Cecil Medicine)
Quick Reference Summary Table
| Parameter | Cardiac Dyspnoea | Respiratory Dyspnoea |
|---|---|---|
| Key mechanism | Pulmonary venous congestion / raised PCWP | Airflow obstruction / V-Q mismatch |
| Orthopnoea | Very prominent | Less prominent |
| PND | Highly specific (severe HF) | Can occur (less specific) |
| Sputum | Frothy pink (oedema) or dry | Purulent (COPD/infection), dry |
| Wheeze | Cardiac asthma (soft, variable) | Loud, expiratory (asthma/COPD) |
| JVP | Raised | Normal unless cor pulmonale |
| S3 / gallop | Present | Absent |
| BNP | Markedly elevated | Normal |
| CXR | Cardiomegaly + pulmonary oedema | Hyperinflation / consolidation |
| Response to diuretics | Rapid relief | No relief |
| Response to bronchodilators | Partial (cardiac asthma) | Marked relief |
Sources: Goldman-Cecil Medicine, 26th ed. | Murray & Nadel's Textbook of Respiratory Medicine | Frameworks for Internal Medicine | Goldman-Cecil Medicine (Heart Failure Chapter, Chapter 45)
DEFINE ELDERLY. WHAT ARE THE AIRWAY CONCERNS IN ELDERLY PATIENTS
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
I have reached the query_library_db limit. I have sufficient high-quality content from the textbooks to compose a thorough answer. Let me now write the comprehensive response.
Definition of the Elderly
The elderly (also called the geriatric population) is conventionally defined by chronological age ≥ 65 years. This is the internationally accepted threshold used by the WHO and most Western healthcare systems.
However, a purely age-based definition is recognised as insufficient. As noted in Rockwood and Green's Fractures in Adults:
"While the chronological definition of a 'geriatric' or 'elderly' patient is typically 65 years of age or older, an age-only distinction does not necessarily correlate with a patient's physiology."
Sub-classification of the Elderly
| Category | Age |
|---|---|
| Young-old | 65 - 74 years |
| Middle-old | 75 - 84 years |
| Oldest-old (very elderly) | ≥ 85 years |
A more physiologically meaningful definition considers frailty, functional reserve, comorbidity burden, and biological age rather than chronological age alone. Injured patients over 74 years carry considerably higher mortality risk, even with equivalent injury severity scores compared to younger adults.
Airway Concerns in Elderly Patients
Ageing produces a constellation of anatomical, physiological, and pharmacological changes that collectively make airway management in the elderly more challenging and higher risk. These can be grouped as follows:
1. Anatomical Changes Affecting the Airway
a) Dentition - Edentulousness
- Tooth loss is common in the elderly
- Edentulous patients are notoriously difficult to mask ventilate - the loss of teeth causes the cheeks to collapse inward, making it nearly impossible to achieve an airtight seal with a face mask
- Conversely, dentures, if present, may loosen during airway manipulation and obstruct the airway - they must be removed before intubation but kept in place during mask ventilation to maintain facial contour
"Elderly patients may not have teeth or dentures to help maintain airway patency; edentulous patients are often difficult to mask ventilate, and dentures may loosen and obstruct the airway." - Miller's Anesthesia, 10e
b) Cervical Spine Degeneration and Kyphosis
- Degenerative changes of the cervical spine (spondylosis, osteophytes, reduced disc height) severely restrict neck extension
- Kyphoscoliosis and reduced cervical mobility impair the ability to achieve the "sniffing position" needed for optimal laryngoscopy
- This directly increases the difficulty of direct laryngoscopy and intubation
- Forced neck extension in a patient with severe cervical spondylosis risks spinal cord injury
"Degenerative spine changes and kyphoscoliosis may complicate intubation." - Miller's Anesthesia, 10e
c) Chest Wall Stiffness
- Calcification of costal cartilages and rib joints leads to reduced chest wall compliance
- Decreased intervertebral space height and kyphosis cause a reduction in the FEV1/FVC ratio
- These changes limit ventilatory reserve and make bag-mask ventilation more effortful
d) Reduced Muscle Mass (Sarcopenia)
- Intercostal and diaphragmatic muscle strength decreases with age
- Reduced respiratory muscle strength limits the ability to generate effective coughs and deep breaths
- This predisposes to atelectasis, secretion retention, and postoperative pneumonia
2. Physiological Changes Affecting Airway and Respiratory Function
a) Reduced Lung Elasticity and Compliance
- Loss of elastin fibres in the lung parenchyma results in increased lung compliance (floppier lungs) but loss of elastic recoil
- This leads to early airway closure during expiration, air trapping, and emphysema-like changes even in non-smokers
- Dynamic airway collapse during forced expiration worsens V/Q mismatch
b) Altered Lung Volumes
| Parameter | Change with Ageing |
|---|---|
| Residual Volume (RV) | Increased |
| Functional Residual Capacity (FRC) | Increased |
| Vital Capacity (VC) | Decreased |
| FEV1 | Decreased |
| Total Lung Capacity (TLC) | Minimally changed |
- The increase in RV at the expense of VC means the elderly have less usable oxygen reserve
- Reduced FRC means the closing capacity approaches or exceeds FRC, especially in the supine position, causing dependent airway closure even during tidal breathing - this accelerates desaturation during apnoea
c) Impaired Gas Exchange
- Increased V/Q mismatch due to loss of alveolar surface area and capillary bed
- Decreased diffusion capacity (DLCO) across the alveolar-capillary membrane
- Baseline PaO2 is lower in the elderly (estimated as: PaO2 = 100 - [age/4] mmHg)
- These factors mean elderly patients desaturate faster and more severely during apnoea, difficult intubation, or any period of hypoventilation
d) Blunted Chemo-receptor Response
- The ventilatory response to hypoxaemia is reduced by ~50% in healthy elderly individuals
- The ventilatory response to hypercapnia is also diminished
- This is particularly dangerous because patients may not mount a compensatory hyperventilation when hypoxic or hypercapnic, masking impending respiratory failure
"Due to deranged respiratory drive seen with aging, elderly patients will have a diminished physiologic response to both hypoxaemia and hypercapnia." - Mulholland & Greenfield's Surgery
e) Impaired Mucociliary Clearance
- Dysfunction of the mucociliary escalator with age leads to retained secretions in the airways
- This predisposes to aspiration pneumonitis and hospital-acquired pneumonia
- Combined with reduced cough effectiveness (weakened respiratory muscles), secretion clearance is markedly impaired
3. Protective Reflex Impairment
- Upper airway protective reflexes (gag, cough, swallow) are diminished with ageing
- Pharyngeal muscle tone decreases, increasing the risk of oropharyngeal obstruction and obstructive sleep apnoea
- Aspiration risk is significantly higher - reduced laryngeal sensitivity, impaired swallowing coordination (dysphagia), and delayed gastric emptying all contribute
- Gastro-oesophageal reflux is more prevalent in the elderly, further increasing aspiration risk
4. Pharmacological Considerations in Airway Management
- Elderly patients have reduced drug requirements for sedatives, induction agents, and opioids due to:
- Decreased hepatic blood flow and Phase I metabolism
- Reduced renal clearance
- Increased body fat-to-lean ratio (altered drug distribution)
- Decreased plasma proteins (higher free drug fraction)
- Neuromuscular blockade: Normal changes at the neuromuscular junction with ageing alter the pharmacodynamics of blocking agents - onset may be slower but duration prolonged
- Polypharmacy (beta-blockers, anticoagulants, antihypertensives) blunts compensatory responses and increases haemodynamic lability during airway manipulation
5. Comorbidities Adding to Airway Difficulty
| Comorbidity | Specific Airway Impact |
|---|---|
| COPD | Air trapping, bullae, risk of pneumothorax with PPV |
| Obstructive Sleep Apnoea | Difficult mask ventilation, difficult intubation, sensitive to sedation |
| Rheumatoid arthritis | Atlanto-axial subluxation, restricted mouth opening (TMJ) |
| Ankylosing spondylitis | Fixed flexed cervical spine - very difficult intubation |
| Obesity (common in elderly) | Reduced FRC, rapid desaturation |
| Dementia/agitation | Poor cooperation during awake procedures |
6. Clinical Implications for Practice
| Concern | Management Strategy |
|---|---|
| Difficult mask ventilation (edentulous) | Keep dentures in for preoxygenation and mask ventilation; use two-handed technique, oropharyngeal airway |
| Restricted neck extension | Pre-position with careful padding; consider video laryngoscopy as first-line; fibreoptic intubation for severely restricted necks |
| Rapid desaturation | Meticulous pre-oxygenation (3-5 min of 100% O2); apnoeic oxygenation (high-flow nasal O2) |
| Aspiration risk | Rapid sequence induction; avoid prolonged supine positioning; head-up positioning |
| Blunted hypoxic drive | Monitor SpO2 continuously; do not assume patient will "compensate" |
| Drug sensitivity | Reduce doses of induction agents by 30-50%; titrate carefully |
| Secretion retention | Chest physiotherapy, incentive spirometry, early mobilisation post-procedure |
Summary
The elderly patient presents a cluster of airway challenges that arise from the combined effects of anatomical deformation (edentulousness, kyphosis, cervical spondylosis), physiological decline (reduced FRC, impaired gas exchange, blunted chemo-reflexes, weakened respiratory muscles), and loss of protective reflexes (aspiration risk, obstructive apnoea). These changes are compounded by common comorbidities and polypharmacy. The result is a population that tolerates apnoea poorly, is difficult to intubate and ventilate, and is highly susceptible to post-procedural pulmonary complications.
Sources: Miller's Anesthesia, 10e | Mulholland & Greenfield's Surgery, 7e | Rockwood & Green's Fractures in Adults, 10e | Fitzpatrick's Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.