Physics in vessel physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content to deliver a thorough answer. Let me compile it.
Physics in Vessel Physiology
Vascular physiology is governed by a small set of physical laws that explain how blood flows, how vessels resist or accommodate that flow, and how vessel walls bear the mechanical loads imposed by pressure. Below is a structured breakdown of each core principle.
1. The Fundamental Flow Equation
Blood flow (Q) through any vessel follows the same logic as Ohm's law in electrical circuits:
Q = ΔP / R
- Q = flow (mL/min)
- ΔP = pressure gradient (driving pressure; difference between upstream and downstream pressure)
- R = resistance
Flow is directly proportional to the pressure gradient and inversely proportional to resistance. The direction of flow always moves from high to low pressure - left ventricle to aorta during systole, vena cava to right atrium at all times.
Total peripheral resistance (TPR/SVR) is calculated by substituting cardiac output for Q and the aorta-to-vena cava pressure difference for ΔP. The primary mechanism by which the body controls blood flow is by changing arteriolar resistance.
- Costanzo Physiology 7th Edition, p. 128-129
2. Poiseuille's Law - Resistance to Flow
The physical determinants of resistance are captured in the Poiseuille equation:
$$R = \frac{8\eta l}{\pi r^4}$$
| Variable | Meaning |
|---|---|
| η | Viscosity of blood |
| l | Length of the vessel |
| r | Radius (raised to the 4th power) |
The most important concept: the r⁴ relationship. A 50% reduction in radius does not double resistance - it increases it by 16-fold (2⁴). A 75% reduction in radius (radius cut to 1/4 of original) increases resistance by 256-fold (4⁴), reducing flow to less than 0.4% of baseline. This is why partial arterial occlusion (e.g., carotid stenosis, coronary artery disease) produces catastrophic changes in flow.
Blood viscosity (η) is determined largely by hematocrit. Polycythemia raises viscosity and therefore resistance; severe anemia lowers viscosity. Viscosity also rises at very low flow rates (non-Newtonian behavior of blood).
- Costanzo Physiology 7th Edition, p. 129-130
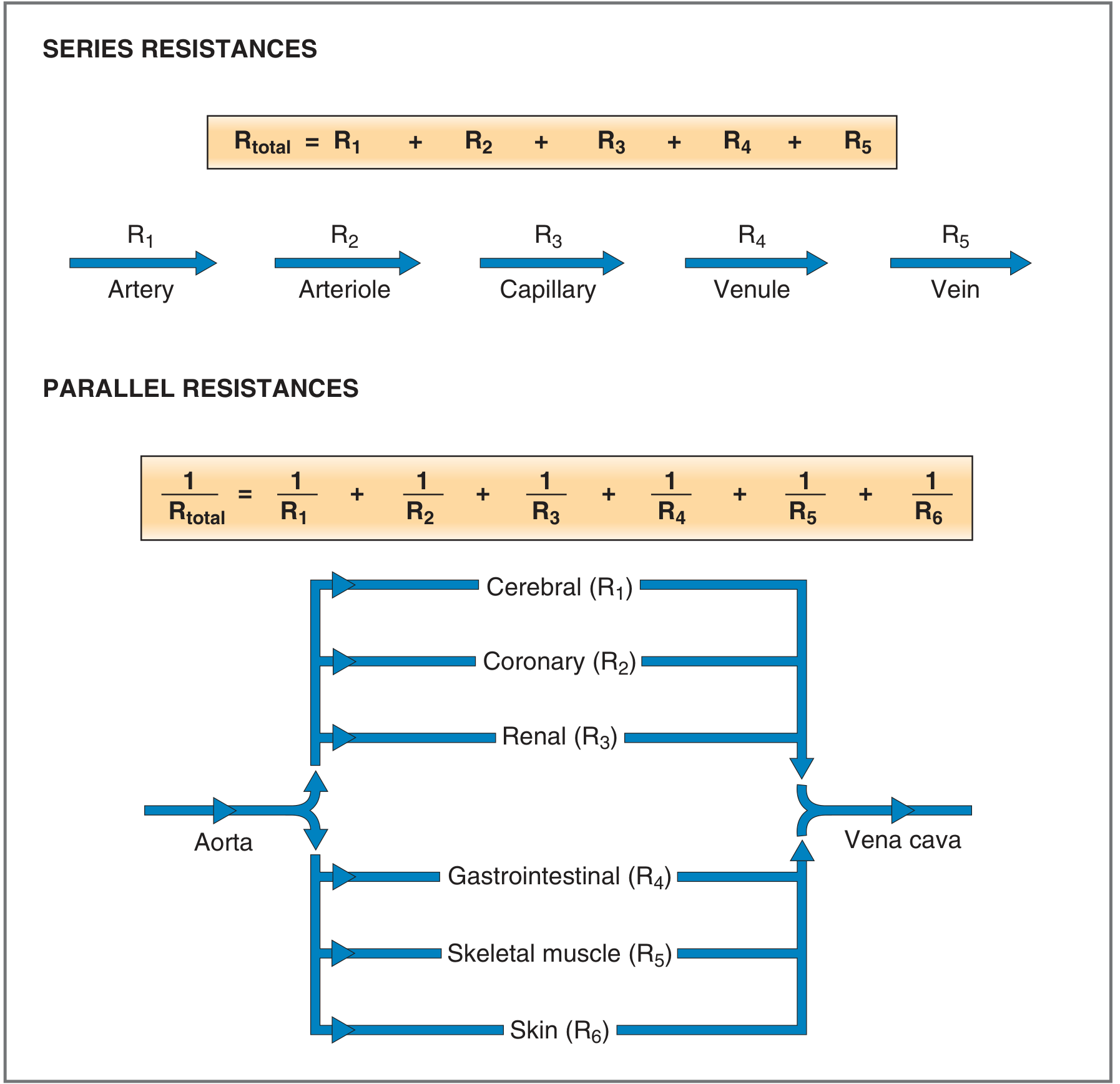
3. Series vs. Parallel Resistance
The arrangement of vessels determines total resistance:
Series Resistance (within one organ)
Blood flows sequentially: artery → arteriole → capillary → venule → vein
$$R_{total} = R_{artery} + R_{arterioles} + R_{capillaries} + R_{venules} + R_{vein}$$
- Total resistance is the sum of all individual resistances
- Arterioles contribute the largest portion - hence the greatest pressure drop occurs here
- Total flow is equal at every level in series
Parallel Resistance (between organs)
Cardiac output distributes simultaneously among cerebral, coronary, renal, GI, skeletal muscle, and skin circulations:
$$\frac{1}{R_{total}} = \frac{1}{R_1} + \frac{1}{R_2} + \frac{1}{R_3} + ...$$
- Total resistance is less than any single component resistance
- Adding more parallel vessels lowers overall resistance - this is why the systemic vasculature can distribute large volumes of blood
- Costanzo Physiology 7th Edition, p. 130
4. Laminar Flow and the Reynolds Number
Under normal conditions, blood flow is laminar (streamlined):
- A parabolic velocity profile develops: velocity = 0 at the vessel wall (blood adheres to wall), and is maximal at the center
- Layers of blood slide past each other in concentric "sheets" with no mixing between layers
- Laminar flow is silent
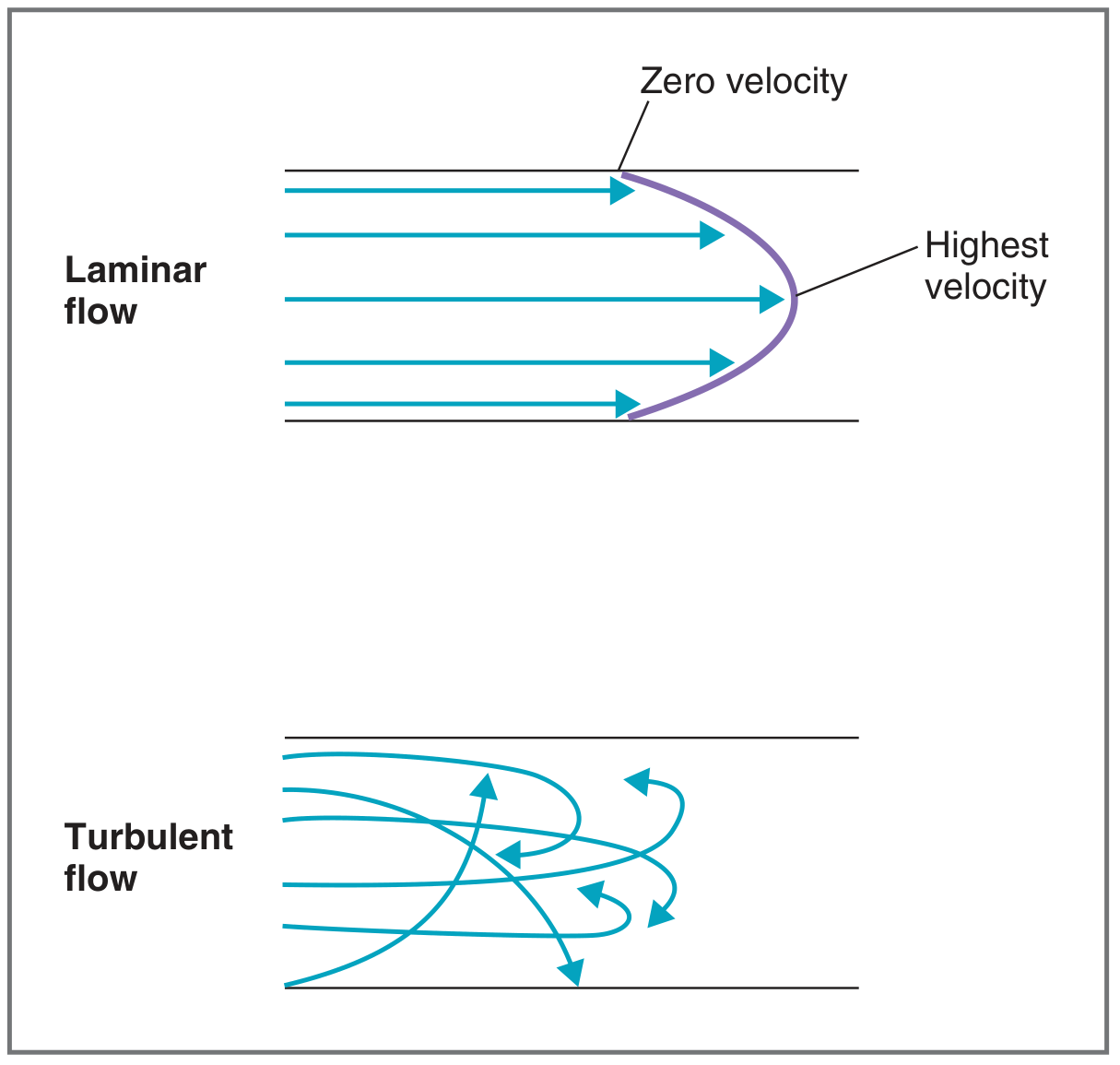
When the flow pattern is disrupted (at valves, stenotic segments, branch points), flow becomes turbulent:
- Blood streams mix radially and axially
- Kinetic energy is wasted in radial and axial motion, so more driving pressure is needed to maintain the same flow
- Turbulent flow produces audible sounds - the physiological basis of Korotkoff sounds (blood pressure measurement) and cardiac/vascular murmurs
The Reynolds number (N_R) predicts whether flow will be laminar or turbulent:
$$N_R = \frac{\rho \cdot d \cdot v}{\eta}$$
| Variable | Meaning |
|---|---|
| ρ | Density of blood |
| d | Vessel diameter |
| v | Mean velocity of flow |
| η | Viscosity |
- N_R < 2000 → laminar flow
- N_R > 2000 → increasing probability of turbulence
- N_R > 3000 → turbulent flow always occurs
Key triggers for turbulence in clinical practice:
- Decreased viscosity (anemia, low hematocrit) - raises N_R
- High-velocity flow at stenotic segments - even though diameter is smaller, the velocity increase predominates and raises N_R
- This explains why anemia produces "flow murmurs" and why stenotic vessels create audible bruits
- Costanzo Physiology 7th Edition, p. 131-132
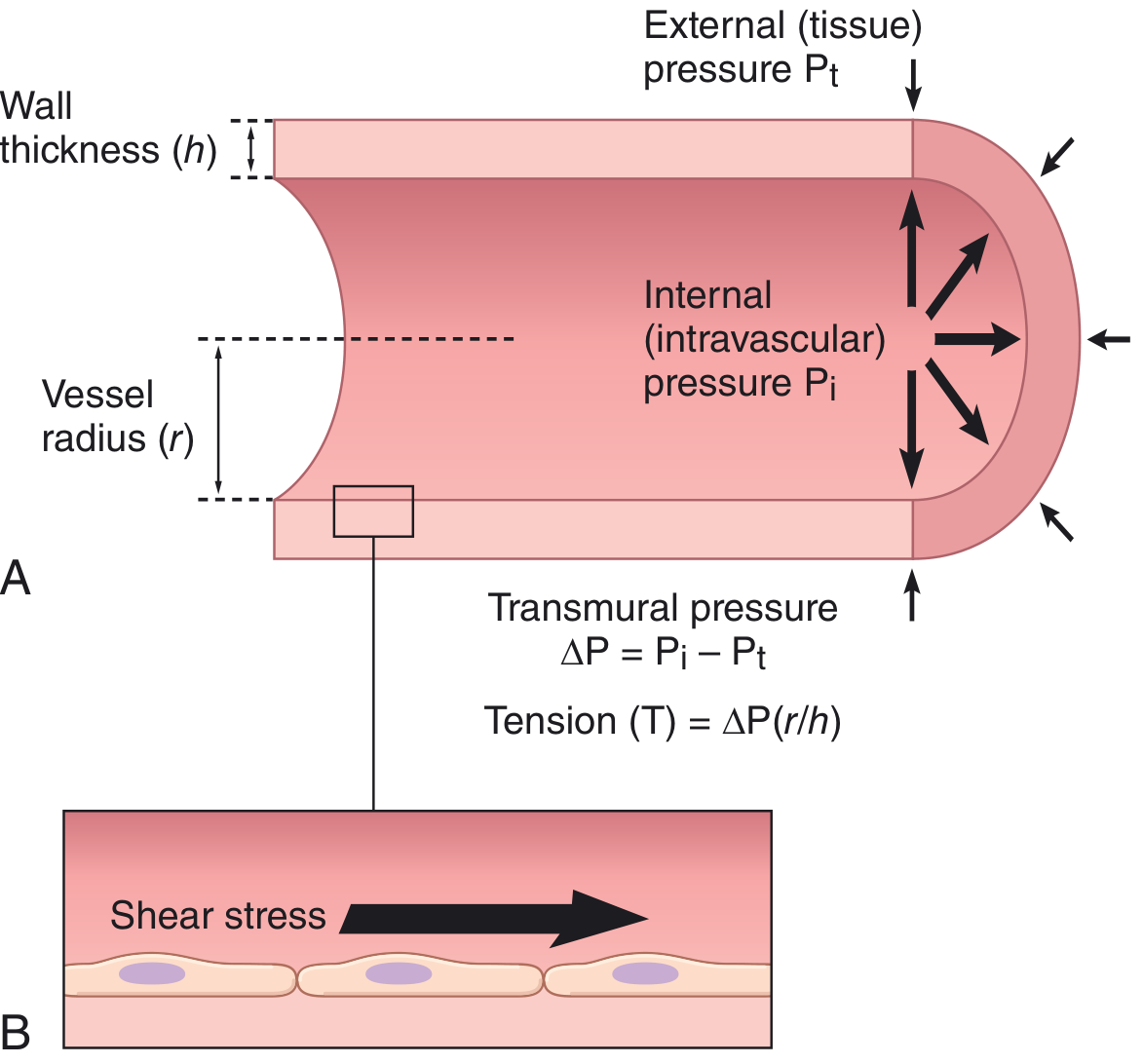
5. Law of Laplace - Wall Tension
A vessel wall must withstand the outward force of intravascular pressure. The Law of Laplace (Young-Laplace, early 1800s) describes this relationship:
$$T = \Delta P \cdot r$$
Or, for thick-walled vessels (incorporating wall thickness h):
$$T = \Delta P \cdot \frac{r}{h}$$
Where:
- T = wall tension (force per unit length, dynes/cm)
- ΔP = transmural pressure (intravascular minus extravascular)
- r = vessel radius
- h = wall thickness
Clinical implications of Laplace's Law:
| Vessel | Radius | Pressure | Wall Tension | Structural adaptation |
|---|---|---|---|---|
| Aorta | Large | ~100 mmHg | Very high | Thick wall with elastin and collagen |
| Arteriole | Small | ~60 mmHg | Moderate | Thick smooth muscle layer |
| Capillary | Very small | ~25 mmHg | Very low | Single endothelial cell layer sufficient |
| Aneurysm | Progressively larger | Same | Progressively higher | Wall rupture risk increases as diameter expands |
This is why capillaries (with their tiny radii) can withstand significant pressures despite having a single-cell wall - their small radius keeps wall tension low. Conversely, an aortic aneurysm becomes increasingly unstable as it dilates: larger radius → higher wall tension → greater rupture risk, in a vicious self-reinforcing cycle.
Shear stress (a separate mechanical force) is the frictional drag that flowing blood exerts on the endothelial surface. It is proportional to flow velocity and viscosity, and inversely related to r³. Endothelial mechanosensors detect shear stress and regulate vascular remodeling throughout life.
- Guyton and Hall Textbook of Medical Physiology, p. 186-187
- Medical Physiology (Boron & Boulpaep), p. 662-663
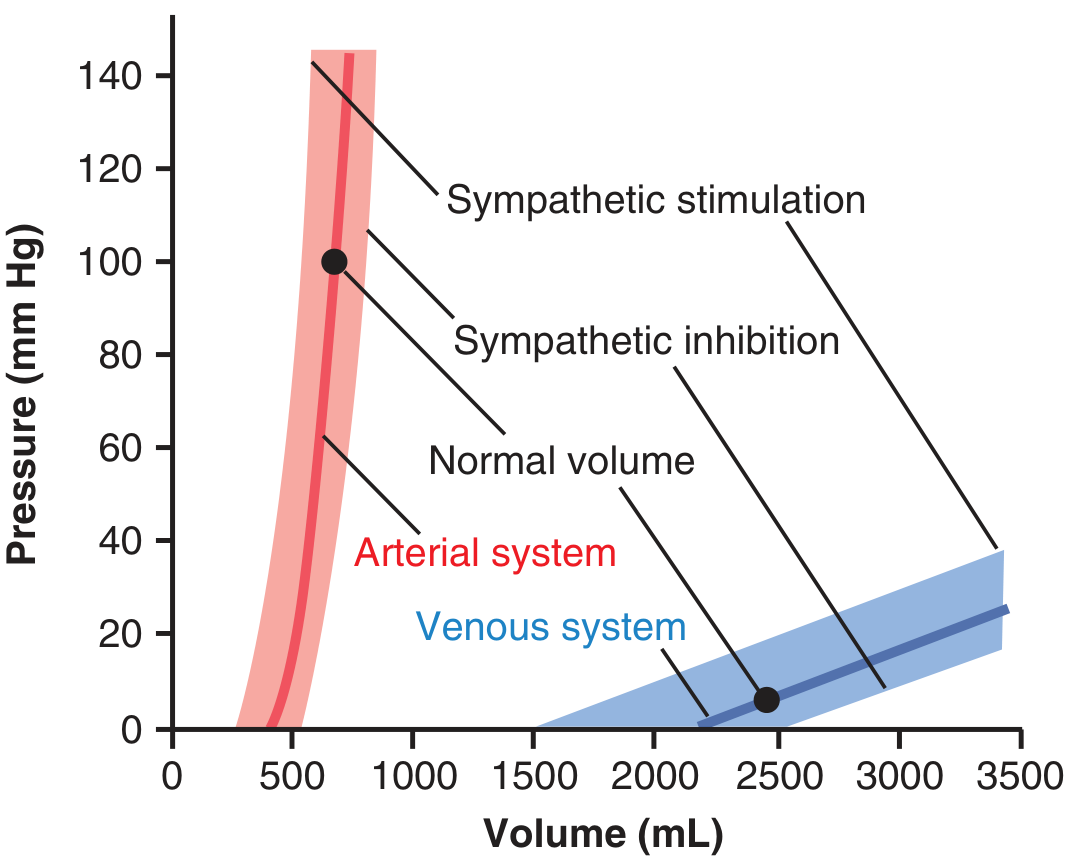
6. Vascular Distensibility and Compliance
All blood vessels are distensible - they expand when pressure rises. This property differs markedly between vessel types:
Vascular distensibility = fractional increase in volume per mmHg pressure rise:
$$\text{Distensibility} = \frac{\Delta V}{\Delta P \times V_0}$$
Vascular compliance (capacitance) = total volume stored per mmHg:
$$\text{Compliance} = \frac{\Delta V}{\Delta P}$$
Note: compliance = distensibility × volume. A vein may be 8× more distensible than a corresponding artery AND have 3× the volume, giving it ~24× greater compliance.
Functional consequences:
- Arteries: Low compliance (relatively stiff walls) → pressure rises sharply with volume addition → act as pressure reservoirs that maintain driving force during diastole (Windkessel effect)
- Veins: High compliance → enormous volumes can be accommodated with minimal pressure change → act as volume reservoirs (capacitance vessels). Up to 500 mL can be shifted into veins with almost no change in venous pressure
Sympathetic tone shifts the pressure-volume curve: Sympathetic stimulation increases smooth muscle tone, raising pressure at any given volume. Inhibition does the opposite. This is how the body rapidly redistributes blood volume during hemorrhage or exercise.
- Guyton and Hall Textbook of Medical Physiology, p. 187-188
Summary Table
| Physical Principle | Key Equation | Primary Site of Importance | Clinical Relevance |
|---|---|---|---|
| Flow-pressure-resistance | Q = ΔP/R | Entire vasculature | Basis of CO, BP, TPR calculations |
| Poiseuille (radius⁴) | R = 8ηl/πr⁴ | Arterioles | Stenosis, vasodilation/constriction |
| Series resistance | R_total = R₁ + R₂ + ... | Within organs | Arterioles dominate organ resistance |
| Parallel resistance | 1/R_total = 1/R₁ + 1/R₂ + ... | Between organ systems | Why adding beds lowers total R |
| Reynolds number | N_R = ρdv/η | Large vessels, stenoses | Murmurs, bruits, Korotkoff sounds |
| Law of Laplace | T = ΔP·r/h | All vessels, aneurysms | Aneurysm risk, capillary integrity |
| Compliance | C = ΔV/ΔP | Arteries & veins | Windkessel effect, volume buffering |
These physical laws work together. Arterioles control resistance (via r⁴ in Poiseuille's law), veins buffer volume (via compliance), arterial walls withstand tension (via Laplace), and the entire system maintains laminar flow to minimize energy losses (governed by Reynolds number).
This is a shared conversation. Sign in to Orris to start your own chat.