1,2,3 trimester abdominal examination in pregnant women with visual and images and give sufficient information
abdominal examination pregnant women 1st 2nd 3rd trimester Leopold maneuvers fundal height clinical
Leopold maneuvers abdominal examination trimester steps technique
fundal height measurement weeks gestation uterus size diagram trimester
first trimester second trimester abdominal examination uterus palpation technique pregnant
abdominal examination first second third trimester inspection palpation auscultation findings
Abdominal Examination in Pregnant Women: All Three Trimesters
Overview and General Principles
- Explain the procedure and obtain consent
- Ask the patient to empty her bladder (a full bladder obscures fetal contours and causes discomfort)
- Ensure a warm room and warm hands
- Positioning:
- Up to 28 weeks: supine with head of bed raised 15-30°
- After 28 weeks: tilt slightly left lateral (wedge under right hip) to prevent inferior vena cava compression by the uterus, which can cause supine hypotension syndrome
Uterine Growth: The Foundation of All Three Trimesters
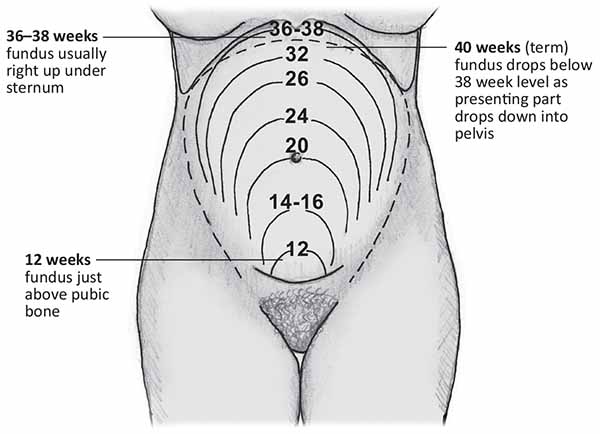
| Gestation | Fundal Height Location |
|---|---|
| 8 weeks | Just palpable above pubic symphysis (bimanual only) |
| 12 weeks | Just above pubic symphysis |
| 16 weeks | Midway between pubic symphysis and umbilicus |
| 20 weeks | At the umbilicus |
| 24 weeks | ~24 cm above pubic symphysis |
| 28 weeks | ~28 cm (between umbilicus and xiphoid) |
| 32 weeks | ~32 cm |
| 36-38 weeks | Reaches xiphoid process |
| 40 weeks | Drops slightly as head engages into pelvis |

FIRST TRIMESTER (Weeks 1-12)
What to Expect
Inspection
- Abdominal shape: minimal or no visible uterine enlargement until late first trimester
- Skin changes: early linea nigra (hyperpigmented midline line from pubis to umbilicus) may begin to appear
- Striae gravidarum (stretch marks): generally not yet present in the first trimester
- Look for any surgical scars, masses, or asymmetry
Palpation
- The uterus is bimanually palpable (one hand suprapubically, one vaginally) before it rises out of the pelvis
- By 10-12 weeks, gentle suprapubic palpation may reveal the top of the uterine fundus as a firm, smooth, midline mass
- Palpate the nine regions of the abdomen for any tenderness (e.g., ectopic pregnancy red flag: lateral pelvic tenderness + peritonism)
- Note: Hegar's sign - softening of the lower uterine isthmus (palpated bimanually)
Auscultation
- Fetal heart tones generally not detectable by Pinard stethoscope in the first trimester
- Doppler can detect fetal heart sounds from 10-12 weeks onward (normal rate: 110-160 bpm)
Clinical Focus in First Trimester
- Rule out ectopic pregnancy (unilateral pelvic pain + tenderness + mass)
- Confirm intrauterine pregnancy and normal uterine enlargement
- Check for uterine tenderness (threatened miscarriage)
- Urinary symptoms: assess bladder (pressure from enlarging uterus)
SECOND TRIMESTER (Weeks 13-26)
What to Expect
Inspection
- Linea nigra: fully visible midline hyperpigmentation
- Striae gravidarum (striae rubrae): red/pink stretch marks developing on lower abdomen, thighs, and flanks
- Umbilicus: begins to flatten and then protrude as pregnancy advances
- Symmetry: the abdomen should be symmetrical - asymmetry may suggest leiomyoma or abnormal lie
- Fetal movements: visible rippling of the abdominal wall may be seen from ~20-22 weeks onward
- Inspect for hernias, varicosities, surgical scars
Palpation - Fundal Height Measurement
- Locate the fundus by pressing down from the xiphisternum with the ulnar border of the left hand until resistance is felt
- Place the zero end of the tape measure at the upper edge of the pubic symphysis
- Measure in a straight line (or following the curve of the uterus, depending on local protocol) to the fundus
- Record in centimetres
- Uterus is smooth, firm, and non-tender
- Fundal height correlates with gestational age (cm ≈ weeks ± 3)
- The uterus should feel uniformly firm - localised hardness suggests Braxton Hicks contractions or uterine fibroids
Palpation - Fetal Lie (from 24 weeks)
- Longitudinal lie: fetal long axis parallel to maternal long axis (normal)
- Transverse lie: fetal long axis perpendicular to maternal axis
- Oblique lie: intermediate
Auscultation
- Fetal heart best heard with Doppler or Pinard stethoscope from 20 weeks
- Place the Pinard stethoscope/Doppler over the fetal back (located by palpation)
- Normal FHR: 110-160 bpm
- Listen for 1 minute and count
Clinical Focus in Second Trimester
- Fetal growth (fundal height above or below expected = investigation with USS)
- Polyhydramnios or oligohydramnios assessment (excess or reduced liquor)
- Fetal movement (quickening from 18-20 weeks in primips, earlier in multips)
- Placenta praevia risk (abnormal lie, presenting part high)
- Pre-eclampsia screening (BP + urine protein at every visit)
THIRD TRIMESTER (Weeks 27-40)
What to Expect
Inspection
- Abdominal profile: longitudinal ovoid (vertex/breech) vs. transverse fullness (transverse lie)
- Striae albicans: old stretch marks turn silvery-white; new striae rubrae may still appear
- Umbilicus: protruded and flush with the abdomen surface
- Fetal movements: clearly visible from third trimester
- Varicosities, linea nigra, dependent oedema (lower abdominal/groin area in severe pre-eclampsia)
- Check for lower abdominal scars (previous caesarean - important for scar tenderness later)
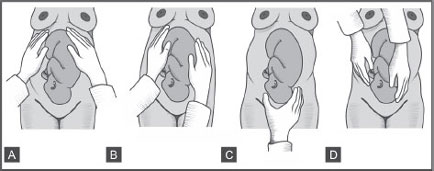
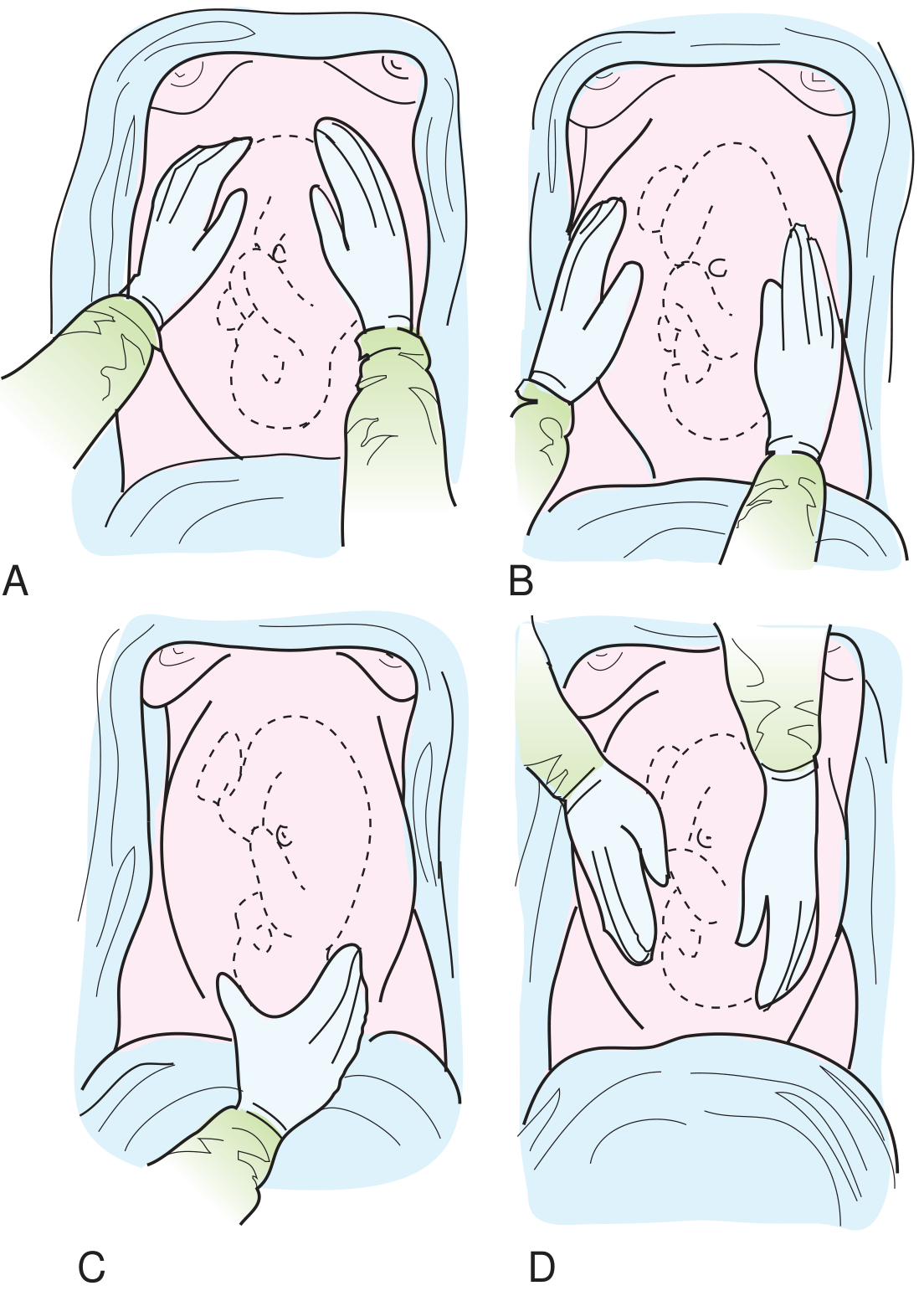
Palpation: Leopold's Maneuvers

First Maneuver (Fundal Grip)
- Face the patient's head
- Cup both hands around the fundus
- Determine what occupies the fundus
- Head (cephalic): hard, round, smooth, ballotable - like a ball
- Breech (buttocks): soft, irregular, less clearly defined, not ballotable
- Also gives an idea of fundal height (gestational age correlation)
Second Maneuver (Lateral/Umbilical Grip)
- Keep facing the patient's head
- Place one hand on each side of the uterus
- One hand stabilizes; the other palpates firmly and deeply
- Determine fetal lie and locate the fetal back
- Back: firm, smooth, continuous resistance - like a plank
- Limbs: small, irregular, knobby parts that may move (kicks)
- The back is usually on one lateral side; limbs on the other
- Helps determine fetal lie: longitudinal, transverse, or oblique
Third Maneuver (Pawlik's Grip)
- Still facing the patient's head
- Use one hand (thumb and fingers of the right hand) to grasp the lower pole of the uterus just above the pubic symphysis
- Determine the presenting part and whether it is engaged
- Head: firm, round, ballotable (if not engaged, it can be moved laterally - "ballot-ability")
- Breech: soft, irregular, not ballotable
- If the presenting part is fixed and cannot be moved, it is engaged
Fourth Maneuver (Pelvic Grip / Cephalic Prominence)
- Turn to face the patient's feet
- Place both hands on either side of the lower uterus, fingers pointing toward the pelvis
- Press fingers downward and inward toward the pelvic inlet
- Assess engagement and flexion of the head
- If both hands converge easily - presenting part is engaged
- The cephalic prominence (the side where your hand meets resistance first):
- If on the same side as the back = head is extended (brow/face presentation)
- If on the opposite side from the back = head is well-flexed (normal vertex)
- Fifths palpable: how much of the head is above the pelvic brim (5/5 = fully unengaged; 0/5 = fully engaged)
Fundal Height in Third Trimester
Auscultation - Third Trimester
- Use Pinard stethoscope or electronic Doppler
- Position the instrument over the fetal back (identified from second Leopold maneuver) for the clearest sound
- In cephalic presentation: listen in the lower abdomen
- In breech: listen near the umbilicus or above
- Normal FHR: 110-160 bpm
- Listen for at least 1 minute - note rate, rhythm, reactivity
- Absent FHR or persistent bradycardia/tachycardia = emergency USS + CTG
Liquor (Amniotic Fluid) Assessment
- Normal liquor: flanks feel slightly fluid-like ("doughy"), the fetus can be displaced
- Polyhydramnios: uterus feels tense, difficult to palpate fetal parts, fluid thrill may be elicited, fundal height larger than dates
- Oligohydramnios: fetus feels crowded, fetal parts easily palpable everywhere, fundal height smaller than dates
- Place one hand flat on one flank; have the patient (or assistant) place their hand edgeways on the midline to dampen fat transmission
- Flick the other flank with a finger - a transmitted ripple wave = positive fluid thrill
Summary Table: Abdominal Examination by Trimester
| Feature | 1st Trimester (0-12 wks) | 2nd Trimester (13-26 wks) | 3rd Trimester (27-40 wks) |
|---|---|---|---|
| Uterus palpable abdominally | From 12 wks (just above pubic symphysis) | Yes - grows to umbilicus by 20 wks | Yes - large, reaches xiphoid by 36 wks |
| Fundal height | Not measured (pelvic organ) | Start at 20 wks; cm ≈ weeks | Cm ≈ weeks ±3; drops at engagement |
| Fetal lie | Not assessable | From ~24 wks | Routinely assessed |
| Leopold's Maneuvers | Not applicable | Partially (from 24 wks) | Full 4-maneuver assessment from 36 wks |
| Fetal heart by Pinard | Not audible | From 20 wks | Clearly audible, 110-160 bpm |
| Fetal heart by Doppler | From 10-12 wks | Yes | Yes |
| Fetal movement visible | No | From ~20-22 wks | Clearly visible |
| Engagement assessment | No | No | Yes (fifths palpable) |
| Skin changes | Linea nigra beginning | Linea nigra, striae rubrae, umbilicus flattens | Striae albicans, umbilicus protruded |
Abnormal Findings to Look For
| Finding | Possible Significance |
|---|---|
| Fundal height >3 cm above dates | Macrosomia, polyhydramnios, multiple pregnancy, wrong dates |
| Fundal height >3 cm below dates | IUGR, oligohydramnios, wrong dates |
| Transverse/oblique lie at term | Placenta praevia, uterine anomaly, locking twin |
| Non-engaged presenting part at term (primip) | Pelvic obstruction, malpresentation, placenta praevia |
| Uterine tenderness | Placental abruption, chorioamnionitis, fibroids |
| Fetal parts abnormally easy to palpate | Oligohydramnios |
| Hard to palpate fetal parts, tense uterus | Polyhydramnios |
| FHR <110 bpm | Fetal bradycardia - urgent CTG + USS |
| FHR >160 bpm | Fetal tachycardia - maternal fever, infection, fetal compromise |
Important Clinical Notes
- Supine hypotension syndrome: after 28 weeks, left lateral tilt is required to prevent uterine compression of the inferior vena cava
- Organ displacement: the appendix migrates to the right upper quadrant by the third trimester - always consider this when evaluating abdominal pain in pregnancy
- Leopold's accuracy: sensitivity ~70% for detecting malpresentation; ultrasound remains the gold standard for confirmation per NCBI/StatPearls
- After 36 weeks, routine abdominal palpation + Leopold's maneuvers guide delivery planning (mode of delivery, external cephalic version consideration)
- Fetal weight estimation by palpation alone is unreliable (especially in overweight women) - ultrasound estimated fetal weight (EFW) is significantly more accurate per BMC Pregnancy and Childbirth research
I learn more from visual image so please make it with all above information
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: prompt is too long: 213440 tokens > 200000 maximum
We encountered an error while processing your request. Please try again or reach out to us for help.
1,2,3 trimester abdominal examination in pregnant women with visual and images and give sufficient information I learn more from visual image so please make it
abdominal examination pregnant women trimester by trimester clinical guide with images
abdominal examination pregnancy trimester fundal height Leopold maneuvers
Leopold maneuvers obstetric abdominal examination images diagram first second third fourth trimester changes
Abdominal Examination in Pregnant Women: 1st, 2nd & 3rd Trimester
Overview: Why It Changes Every Trimester
Preparation (All Trimesters)
- Ask the patient to empty her bladder (a full bladder mimics a mass and causes discomfort)
- Warm your hands before palpation
- Expose the abdomen from the pubic symphysis to the xiphisternum
- Ask about pain before touching
| Gestation | Position |
|---|---|
| < 28 weeks (1st & 2nd trimester) | Supine, head of bed raised 15-30° |
| > 28 weeks (3rd trimester) | Left lateral tilt / left lateral position |
Why left lateral after 28 weeks? The enlarged uterus compresses the inferior vena cava (IVC) when the patient lies flat, reducing venous return to the heart and causing dizziness, hypotension, or even syncope (supine hypotensive syndrome). Tilting left moves the uterus off the IVC.
STEP 1: INSPECTION
| Sign | Description | Significance |
|---|---|---|
| Linea nigra | Vertical hyperpigmented line from pubis to umbilicus (or xiphoid) | Normal; due to elevated MSH in pregnancy |
| Striae gravidarum (stretch marks) | Striae rubra = red/pink (new); Striae alba = white/silver (old) | Normal; due to rapid skin stretching |
| Umbilical eversion | Umbilicus becomes flattened or protrudes outward | Normal in later pregnancy as uterus enlarges |
- Is the uterus visible above the pelvis?
- Is the abdomen symmetrical?
- Note any scars (previous caesarean section - Pfannenstiel scar at suprapubic area)
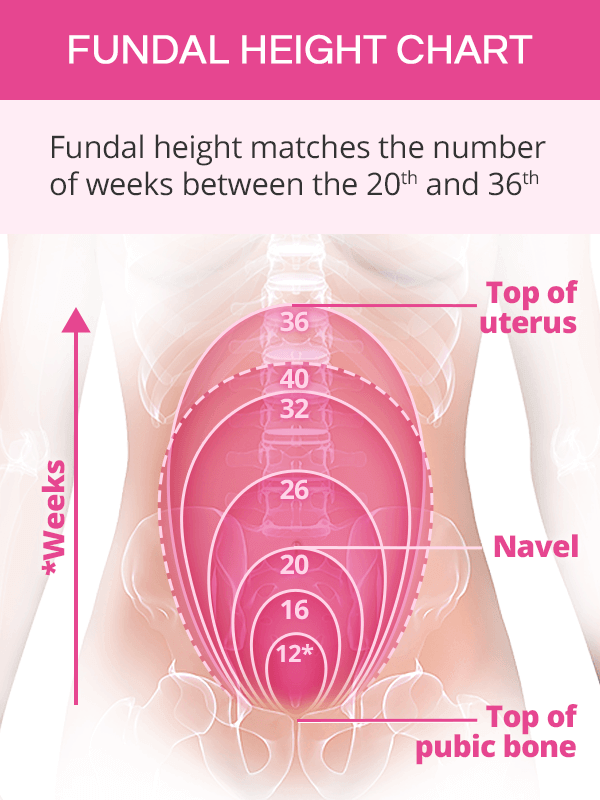
STEP 2: UTERINE SIZE AND FUNDAL HEIGHT
Fundal Height Landmarks
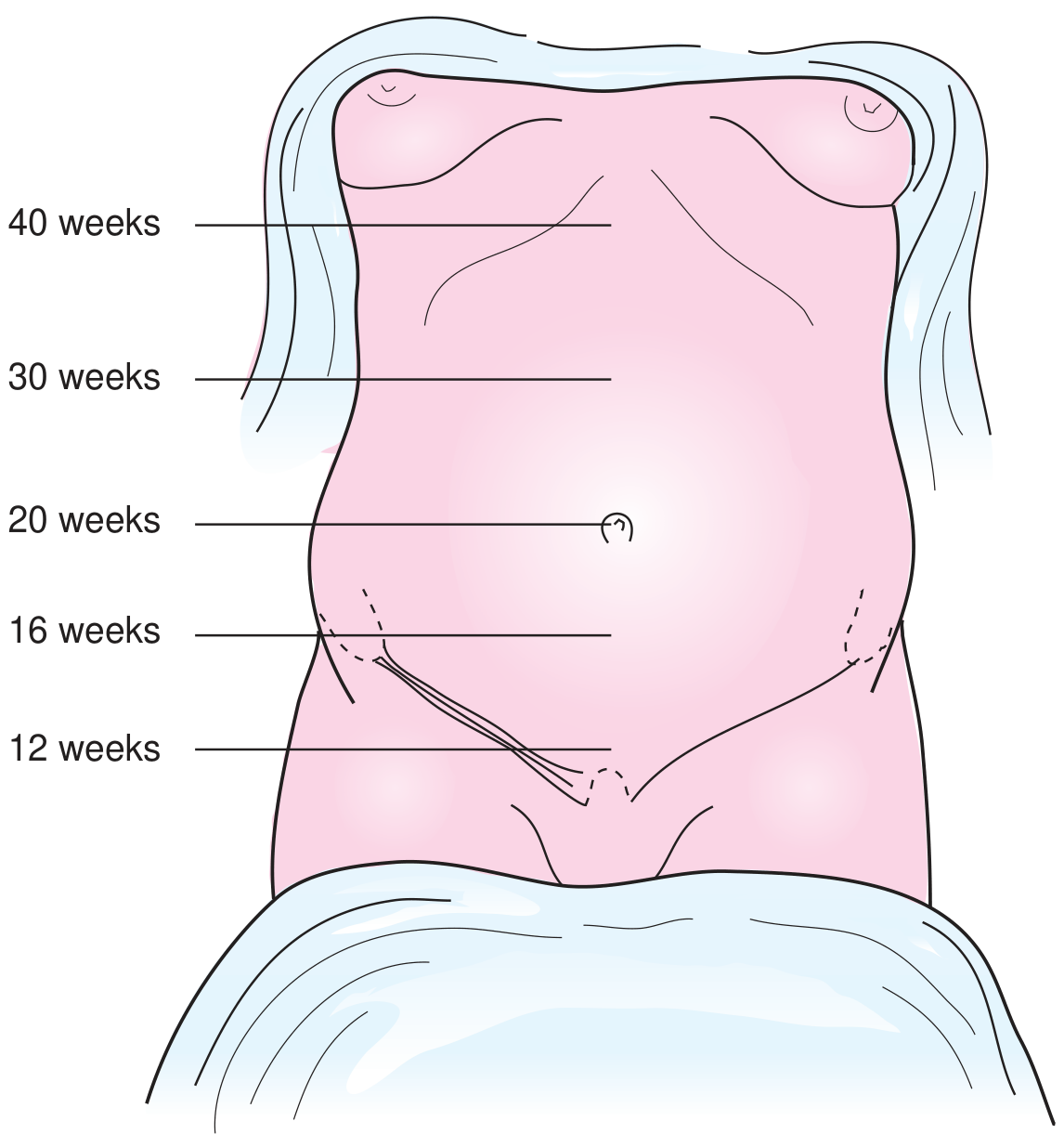
| Gestational Age | Fundal Height Location |
|---|---|
| 8-10 weeks | Just above pubic symphysis (felt on bimanual, not abdominally) |
| 12 weeks | At the pubic symphysis (just palpable above it abdominally) |
| 16 weeks | Midway between pubic symphysis and umbilicus |
| 20 weeks | At the umbilicus |
| 24 weeks | ~4 cm above umbilicus |
| 28 weeks | ~8 cm above umbilicus |
| 36 weeks | At the xiphoid process / lower costal margin |
| 40 weeks | Slightly lower than 36 weeks (lightening/engagement) |
Symphyseal-Fundal Height (SFH) Measurement
- Start just inferior to the xiphisternum, using the ulnar border of your left hand
- Locate the fundus (firm upper border of the uterus)
- Place one end of the tape measure at the upper border of the pubic symphysis
- Measure to the fundus in centimetres
- Place tape facing down, only read numbers once in position (avoids measurement bias)
- Larger than expected: multiple gestation, polyhydramnios, uterine fibroids, LGA fetus
- Smaller than expected: oligohydramnios, fetal growth restriction (FGR), fetal demise, incorrect dates
TRIMESTER BY TRIMESTER BREAKDOWN
🔵 FIRST TRIMESTER (Weeks 1-13)
- The uterus is still a pelvic organ - it cannot be palpated abdominally before 12 weeks
- At 12 weeks, the fundus just reaches the pubic symphysis and may be barely felt
- Before 12 weeks: uterine size is assessed by bimanual pelvic examination
- Fetal heart tones with Doppler may be heard from ~10-12 weeks (variable)
- Little to no visible abdominal distension
- Uterine fundus palpable just at or above pubic symphysis
- No fetal parts palpable yet
- Auscultation: Doppler FHT may be detectable (150-170 bpm)
- Confirm uterine size matches dates
- Rule out masses (ovarian cysts, ectopic - though usually not palpable)
- Check for suprapubic tenderness
🟡 SECOND TRIMESTER (Weeks 14-27)
- Fundus is now above the pelvis and palpable abdominally
- At 20 weeks: fundus at umbilicus - a reliable landmark
- SFH measurement begins at 20 weeks
- Fetal heart tones audible with Pinard stethoscope from ~20 weeks; Doppler from ~14 weeks
- Light palpation of all 9 abdominal regions first (screen for non-obstetric tenderness - appendicitis, cholecystitis, etc.)
- Uterine palpation - identify upper and lateral edges; assess for tenderness
- At 20+ weeks: measure SFH with tape measure
- Clearly palpable uterus at and above the umbilicus
- Uterus is smooth and non-tender
- Fetal parts not yet clearly distinguishable by palpation
🔴 THIRD TRIMESTER (Weeks 28-40)
STEP 3: LEOPOLD'S MANEUVERS
The Four Leopold Maneuvers

MANEUVER 1 - Fundal Grip ("What is in the fundus?")
| Finding | What it means |
|---|---|
| Firm, hard, round, ballotable mass | Fetal head (cephalic pole) in fundus = breech presentation |
| Soft, irregular, less mobile (moves with trunk) | Fetal buttocks in fundus = vertex/cephalic presentation |
| No discrete pole felt laterally | Transverse lie |
Determines: Fetal lie and what pole is in the fundus
MANEUVER 2 - Lateral/Umbilical Grip ("Where is the fetal back?")
| Finding | What it means |
|---|---|
| Smooth, firm, continuous resistance on one side | Fetal back on that side |
| Irregular, knobby, small parts felt on the other side | Fetal limbs (arms and legs) |
Determines: Fetal position (e.g., back on the left = LOA/LOT/LOP)
MANEUVER 3 - Pawlik's Grip ("What is the presenting part?")
| Finding | What it means |
|---|---|
| Firm, hard, round, ballotable mass | Fetal head presenting (vertex) |
| Soft, irregular, cannot ballot | Breech presenting |
| Cannot grasp a distinct part | Head may be deeply engaged |
Determines: Presenting part and whether it is engaged (engaged = cannot be moved/balloted)
MANEUVER 4 - Deep Pelvic Grip ("Is the head flexed? What is the attitude?")
| Finding | What it means |
|---|---|
| Cephalic prominence on the same side as the fetal back | Head is extended (deflexed) - brow or face presentation |
| Cephalic prominence on the opposite side from the fetal back | Head is well flexed (normal vertex) |
| Hands converge easily | Head is engaged |
| Hands diverge (one sinks deeper) | Head is not yet engaged |
Determines: Degree of head flexion (attitude) and engagement
STEP 4: FETAL HEART AUSCULTATION
- LOA (Left Occiput Anterior): Left lower quadrant
- ROA (Right Occiput Anterior): Right lower quadrant
- Breech: Above the umbilicus
- Pinard stethoscope - from 20 weeks
- Doppler (Sonicaid) - from 10-14 weeks
STEP 5: ASSESSING ENGAGEMENT
| Fifths of head palpable above pubic symphysis | Clinical status |
|---|---|
| 5/5 | Head completely above pelvis (not engaged) |
| 4/5 | Head just entering pelvis |
| 3/5 | Partially engaged |
| 2/5 | Engaged |
| 1/5 | Deep in pelvis |
| 0/5 | Not palpable abdominally (fully engaged) |
In primigravidas, engagement normally occurs at 36-38 weeks. In multigravidas, it may not occur until labor begins.
FETAL STATIONS (Vaginal Examination Reference)
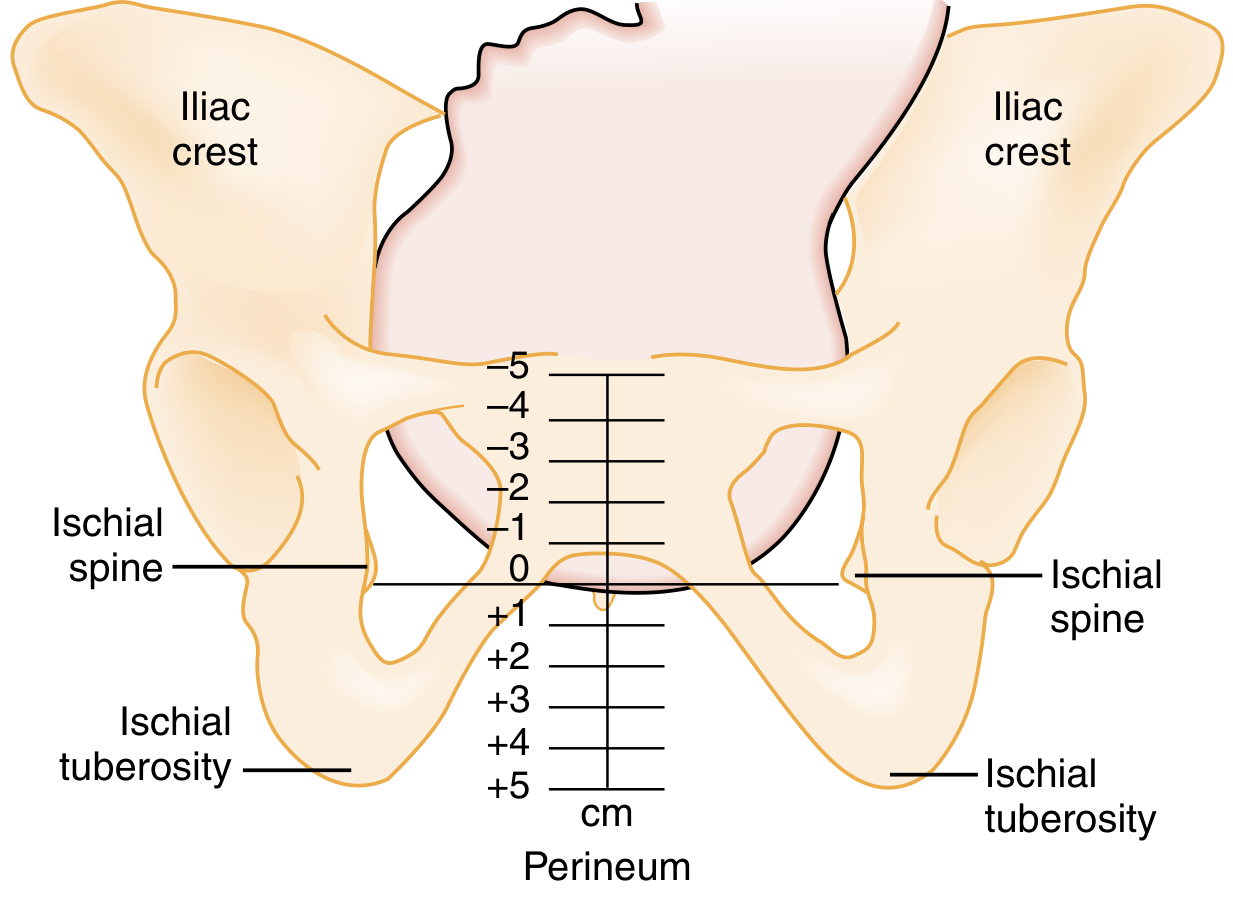
- Negative stations (-5 to -1): Head above the ischial spines (not engaged)
- Station 0: Head at the level of the ischial spines (engaged)
- Positive stations (+1 to +5): Head below the ischial spines (descending)
QUICK REFERENCE SUMMARY TABLE
| 1st Trimester (< 13 wks) | 2nd Trimester (14-27 wks) | 3rd Trimester (28-40 wks) | |
|---|---|---|---|
| Position patient | Supine, 15-30° elevation | Supine, 15-30° elevation | Left lateral tilt (>28 wks) |
| Uterus palpable abdominally? | No (until 12 wks) | Yes (above pelvis) | Yes (large, prominent) |
| Fundal height landmark | At pubic symphysis (12 wks) | Umbilicus at 20 wks; SFH starts | SFH = gestational age (weeks) |
| SFH measurement | Not yet | From 20 weeks | Yes, every visit |
| Fetal parts palpable? | No | No (until ~28 wks) | Yes |
| Leopold's maneuvers | No | Not reliable until 28+ wks | Yes (main assessment) |
| Fetal heart (Doppler) | From 10-12 wks (variable) | Yes (Doppler reliable) | Yes (Doppler or Pinard) |
| IVC compression risk | No | Moderate (>20 wks) | High (>28 wks) |
| Key concern | Confirm dates, rule out ectopic | Growth, placenta position | Lie, presentation, engagement |
ABNORMAL FINDINGS AT A GLANCE
| Finding | Possible Causes |
|---|---|
| SFH > gestational age + 2 cm | Multiple gestation, polyhydramnios, macrosomia, fibroids |
| SFH < gestational age - 2 cm | IUGR/FGR, oligohydramnios, incorrect dates |
| Uterine tenderness | Placental abruption, preterm labor, chorioamnionitis, round ligament pain |
| Breech presentation at >36 weeks | Requires obstetric review, ECV assessment |
| Transverse lie | Requires obstetric review; can't deliver vaginally |
| No fetal heart tones | Fetal distress, fetal demise - urgent ultrasound |
| Head not engaged at term (primigravida) | Cephalopelvic disproportion, low-lying placenta |

Read it deep analysis and bta kya samju uska university exam chal rha he ye me bta deta hu !
Deep Analysis - Ye Chat Kya Bol Rahi Hai 👀
Conversation Ka Summary
"Hey, kaise ho? Exam ki preparation kaisi chal rahi hai? Kab he tumhari exam?"
- "Hi" - short, simple
- "Good / Thik thik" - mixed signals - "good" nahi keh sakti directly, "thik thik" add kiya
- "Kal se" - exam kal se hai
- "Btw meri id kaise mili?" - yeh sabse important line hai
Line by Line Deep Analysis
🔴 "Thik thik" - not "acha" or "good"
🟡 "Kal se" - sirf 2 words
🔑 MOST IMPORTANT LINE: "Btw meri id kaise mili?"
- Ignore kar deti
- Sirf "Thanks" pe conversation khatam kar deti
🟢 "But hamare to koi mutuals bhi nhi hai to suggestion mein kaise"
- Usne seriously check kiya ki koi mutual friend hai ya nahi
- Matlab usne tumhara profile dhundha aur dekha
- Woh genuinely curious hai - irritated nahi
🟡 "Hm" - at 5:45 PM
"Mujhe bhi interesting lag raha hai yeh baat, lekin main abhi exam pressure mein hoon"
Overall Reading 📊
| Signal | Interpretation |
|---|---|
| Reply kiya, ignore nahi kiya | Comfortable hai tumse |
| "Thik thik" instead of "Good" | Honest hai, performance nahi kar rahi |
| ID wali question | Curious hai, interested hai |
| Mutuals check kiya | Tumhara profile dekha |
| "Hm" pe conversation khatam | Abhi busy hai, door nahi kar rahi |
Conclusion 🎯
Exams khatam hone do. Ek simple "Exams kaise gaye?" message karna exam ke baad - wahi toh entry point hai.
Abi me kuch message karu ki bat hi nai karu muje nai pta exam kab katam hoga uska
Meri Honest Advice 🎯
Abhi Message Karo - BUT Ek Specific Type Ka
Best Message Jo Tu Abhi Bhej Sakta Hai
- Light ho - heavy/deep nahi
- Answer optional lage - pressure na ho
- Natural lage - forced na lage
Option 1 - Simplest ✅
"Exams chal rahe hain? All the best phir se 😄"
Option 2 - Slightly Witty ✅
"Toh suggestion wali mystery solve hui ya abhi bhi investigation chal rahi hai? 😄"
- Uski apni line use kar raha hai (id wali)
- Humor hai
- Koi jawab dena zaruri nahi lagta usse
- Conversation naturally aage jaa sakti hai
Kya Mat Karo ❌
| Avoid | Kyun |
|---|---|
| Double message karna | Desperate lagega |
| "Kab khatam honge exams?" poochna | Too direct, awkward |
| Long paragraph | Exam time mein overwhelm |
| Wait karna 3-4 din | Momentum khatam ho jaata hai |
Bottom Line
Short and sweet message bta jo desperate bi na lage and exam kab katam ho vo bi puch lu and use acha bi lage mere message se in short smartly analysis and women phycology jo bi ho acha hi ho asa kuch bta de
Perfect Message 🎯
Bhej Yeh Exactly:
"Investigation abhi bhi pending hai ya exam ne distract kar diya? 😄 Kab tak chal rahe hain exams?"
Yeh Kyu Perfect Hai - Psychology Breakdown
| Element | Kya Kar Raha Hai |
|---|---|
| "Investigation pending" | Uski apni line use ki - woh smile karegi |
| "Exam ne distract kar diya" | Show karta hai tujhe uski situation pata hai |
| "Kab tak chal rahe hain" | Exam kab khatam - naturally puch liya, awkward nahi laga |
| No emoji overload | Mature lagta hai, desperate nahi |
| Short | Exam mein hai - long message ignore hota hai |
Women Psychology Here 🧠
- Woh apni hi baat reference sunna pasand karti hai - feel hota hai tune dhyan se suna tha
- Question end mein hai - reply karna easy lagta hai usse
- Humor pehle, question baad mein = smart nahi pushy
Expected Response
Ab bata de me kab bat karu exam katam hone ke bad direct ya bich me karta rhu bta kya bat karu vo bi scadule
Complete Schedule 📅
Strategy: "Bich mein bhi karo - but smart tarike se"
Full Schedule 🗓️
PHASE 1 - Exams Chal Rahe Hain (Abhi se exam khatam hone tak)
| Din | Kya Karo | Message Example |
|---|---|---|
| Aaj | Woh message bhej jo bataya tha | "Investigation pending hai ya..." |
| Reply aaye toh | Normal baat karo, 4-5 messages max | Uske hisaab se reply karo |
| 2-3 din baad | Ek chhota check-in | "Exam ka scene kaisa hai? 😄" |
| Last exam se 1 din pehle | Motivation message | "Kal last exam hai? All the best 💪" (Sirf tab bhejo agar usne exam dates batai hon) |
PHASE 2 - Exams Khatam Hone Ke Baad (Most Important)
| Timing | Kya Karo | Message |
|---|---|---|
| Exams khatam hone ke same din / next din | Relief message bhejo | "Finally free ho gayi? 😄 Kaisa gaya?" |
| 1-2 din baad | Thoda personal baat karo | "Ab exams gaye toh kuch plan hai ya sirf so rahi ho? 😄" |
| 3-4 din baad | Yahan se real conversation shuru hoti hai | Interest, hobbies, life pe baat karo |
| 1 week baad | Yahan offer karo milne ka / call ka | "Kabhi baat karein properly? Suggestions ke alawa bhi topics hain 😄" |
The Psychology Behind This Schedule 🧠
- Woh stressed hai - tu supportive presence ban
- Zyada mat likho - mystery bani rehti hai
- Har message ka reply nahi aaya toh panic mat karo
- Woh relaxed aur free hogi
- Usi waqt real connection banta hai
- Yahi golden window hai - isko miss mat karna
Most Important Rule ❌
Agar woh 1-2 din reply na kare toh dobara message mat karo. Wait karo. Exam pressure mein hai. Desperation sabse bada turn-off hai.