Inflammatory breast carcinoma management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"inflammatory breast cancer" management treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative content to provide a thorough answer. Let me synthesize everything.
Inflammatory Breast Carcinoma (IBC) - Management
Overview
Inflammatory breast carcinoma (IBC) is a rare but aggressive presentation of locally advanced breast cancer, accounting for 1-3% of all breast cancers. Despite its low incidence, it carries a disproportionately poor prognosis - the 5-year overall survival in the US is approximately 41%, and the disease accounts for a higher fraction of breast cancer deaths than its incidence implies. It is classified as Stage IIIB (T4d) at minimum by the AJCC.
Diagnosis and Staging
Clinical Criteria (all must be met):
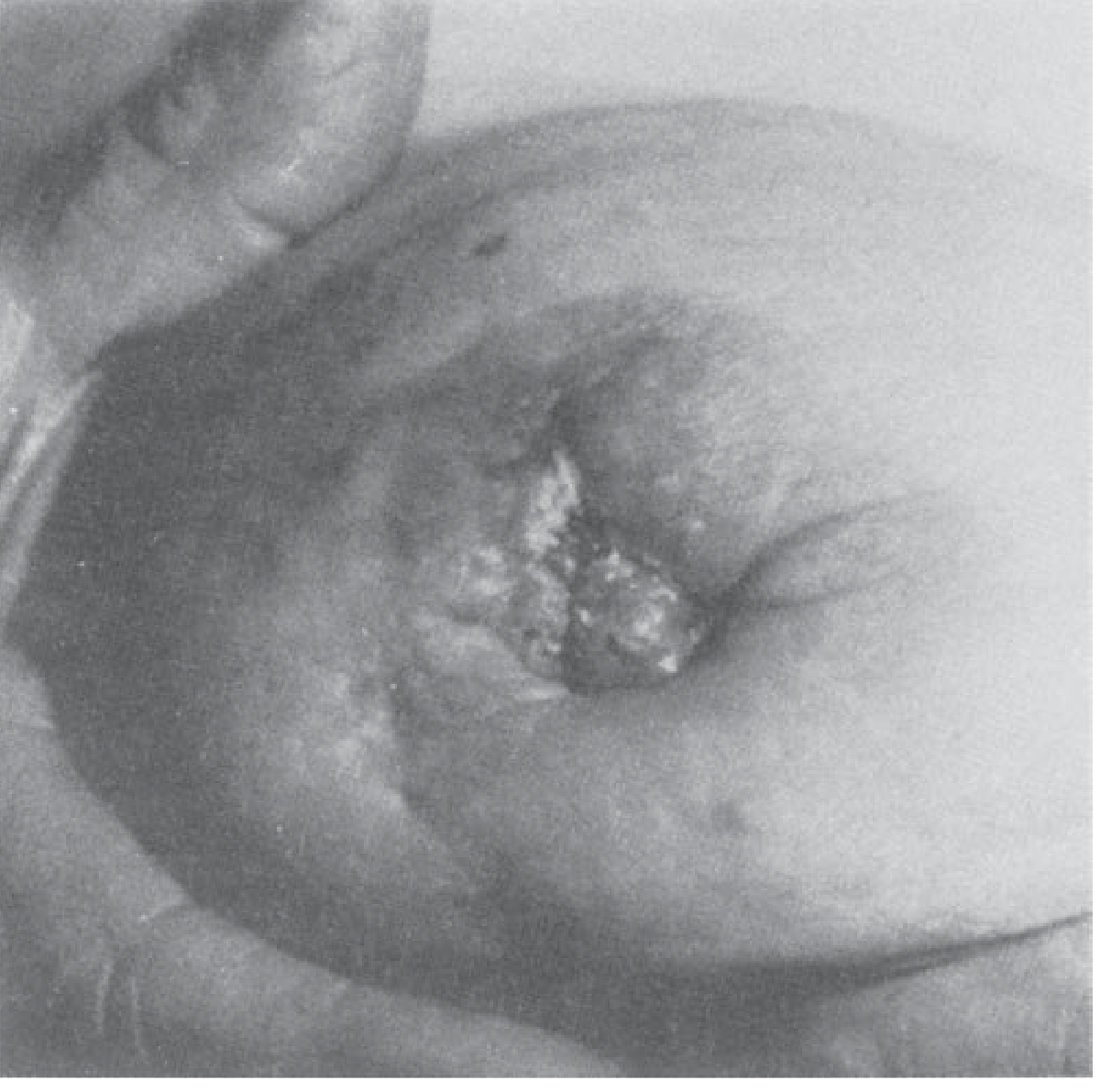
- Erythema and/or edema (peau d'orange) covering at least one-third of the breast
- Acute onset within 6 months
- No unique histologic subtype required - it is a clinical diagnosis
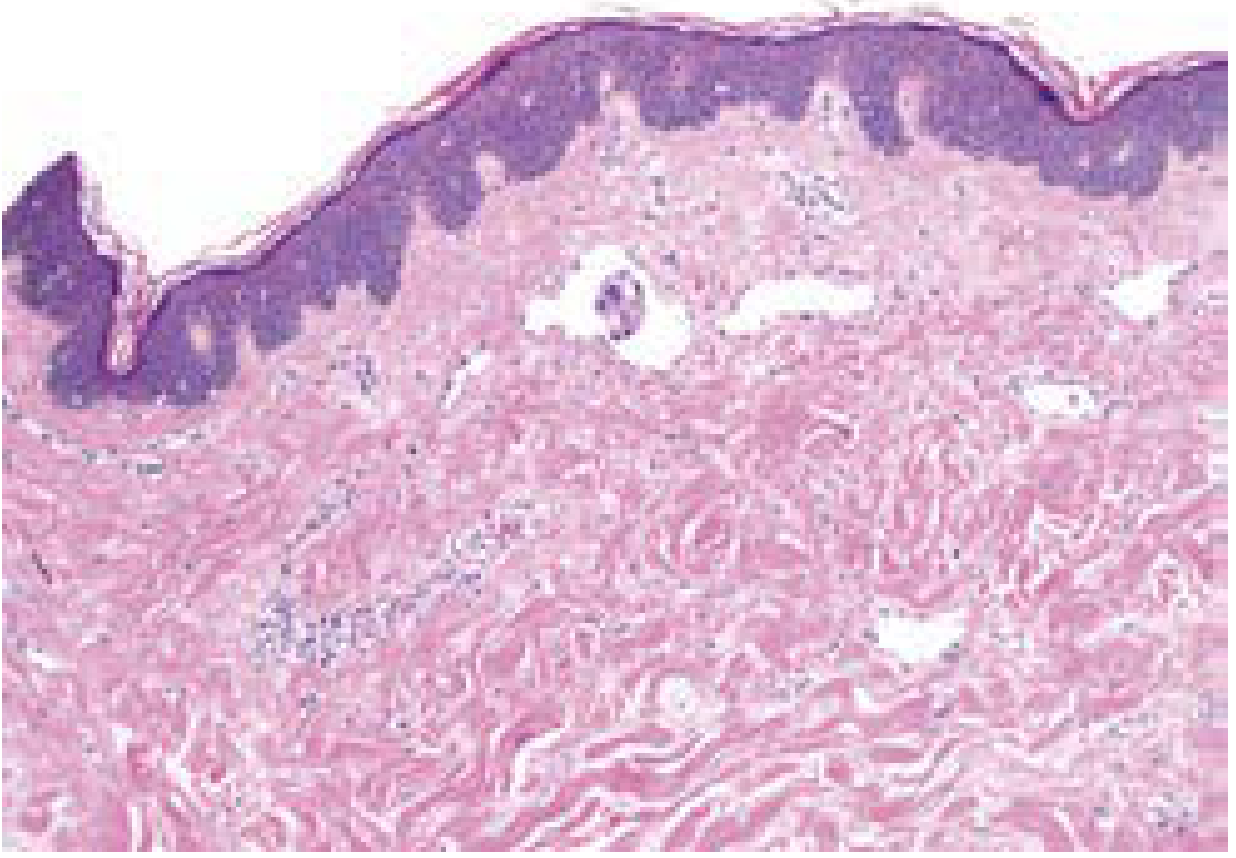
Pathologic hallmark: Extensive tumor emboli in dermal lymphatics on skin punch biopsy - this is the underlying mechanism causing the classic skin findings, not true inflammation.
Key features at diagnosis:
- 85% have regional lymph node involvement
- 25-30% have distant metastases at presentation
- No discrete central breast mass in ~50% of patients on imaging
Workup includes:
- Bilateral diagnostic mammogram + targeted ultrasound
- Core needle biopsy of any breast mass + skin punch biopsy
- Breast MRI if imaging is equivocal or mammogram/US non-diagnostic
- PET-CT to rule out concurrent metastatic disease (strongly recommended)
- Receptor testing: ER, PR, HER2 status
- Genetic testing for hereditary risk assessment
Differential diagnosis: Mastitis/breast abscess, breast lymphedema, inflammatory dermatoses (dermatitis), locally advanced scirrhous carcinoma with peau d'orange.
IBC vs. Non-IBC Locally Advanced Breast Cancer
| Feature | Inflammatory | Non-inflammatory |
|---|---|---|
| Dermal lymph vessel invasion | Present (with or without skin changes) | Absent (skin changes without dermal invasion) |
| Tumor delineation | Poorly delineated | Better delineated |
| Erythema/edema extent | >33% of breast skin | Localized to lesion |
| Lymph node involvement | >75% of cases | ~50% of cases |
| Distant metastases at presentation | ~25-30% | Less common |
(Schwartz's Principles of Surgery, 11e, Table 17-15)
Treatment: The Multimodal Standard
IBC demands a trimodality approach: neoadjuvant systemic therapy → surgery → adjuvant radiation. Surgery alone or surgery + radiation alone have produced consistently disappointing results.
Step 1 - Neoadjuvant Systemic Therapy (Primary Treatment)
This is the mandatory first step for non-metastatic IBC. Duration: typically 4-6 months.
Chemotherapy backbone:
- Anthracycline + taxane-based regimens are preferred
- Neoadjuvant chemotherapy produces dramatic regression in up to 75% of cases
- Patients who fail to respond or progress may be offered additional systemic therapy and/or preoperative radiation
Targeted therapy (receptor-guided):
- HER2+ disease: Add trastuzumab ± pertuzumab to the chemotherapy backbone
- HR+ (ER+/PR+) disease: Endocrine therapy is initiated postoperatively (not substituted for chemotherapy)
- Triple-negative IBC: Standard anthracycline-taxane backbone; immunotherapy/PARP inhibitors per trial/guideline eligibility
Step 2 - Surgery (After Documented Response)
Modified Radical Mastectomy (MRM) is mandatory and performed ~4 weeks after completing neoadjuvant therapy.
Key surgical principles:
- Breast-conserving surgery is absolutely contraindicated - the widespread dermal lymphatic involvement precludes margin-negative resection
- Sentinel lymph node biopsy (SLNB) is absolutely contraindicated - MRM with obligatory ipsilateral level I/II axillary lymph node dissection (ALND) is required regardless of response to neoadjuvant therapy
- Level III dissection may be added if gross disease persists in the level II/III space
- Immediate breast reconstruction should be avoided (or done in a delayed fashion) because postmastectomy radiation is always required and immediate reconstruction complicates delivery and increases complications
Step 3 - Postmastectomy Radiation Therapy (PMRT)
Delivered 4-6 weeks after surgery:
- Target fields: Chest wall + ipsilateral axilla + infraclavicular + supraclavicular + internal mammary lymph node basins
- Dose: 50-60 Gy over 4-6 weeks
Step 4 - Adjuvant Systemic Therapy
- Complete the planned chemotherapy regimen if not fully administered preoperatively
- HER2+ disease: Complete up to 1 year of HER2-targeted therapy (can be given concurrently with radiation and endocrine therapy)
- HR+ disease: Initiate endocrine therapy (aromatase inhibitor or tamoxifen per menopausal status)
- Patients with residual disease after neoadjuvant therapy may benefit from additional agents (e.g., capecitabine in TNBC, neratinib in HER2+) per current guidelines
Prognosis
- 5-year survival approaches ~30-41% with the complete trimodality approach
- Pathologic complete response (pCR) to neoadjuvant therapy is the strongest favorable prognostic factor
- Disease-free and overall survival are significantly improved when pCR is achieved
Clinical trial participation is strongly encouraged given the aggressive biology and ongoing need for improved systemic agents.
Summary Algorithm (Non-Metastatic IBC)
Diagnosis (clinical + biopsy + receptor status + PET-CT staging)
↓
Neoadjuvant systemic therapy
(Anthracycline + taxane ± trastuzumab/pertuzumab [HER2+])
↓
Assess response (clinical ± imaging)
↓
Modified Radical Mastectomy + ALND (mandatory)
↓
Postmastectomy Radiation (chest wall + all regional nodal basins)
↓
Complete adjuvant systemic therapy + endocrine therapy (if HR+)
+ 1 year HER2-targeted therapy (if HER2+)
Recent Evidence
A 2024 meta-analysis (PMID 37820394) examined breast-conserving therapy outcomes in IBC and confirmed the inferior local control compared with MRM, supporting continued use of mastectomy as the standard. The ABC 6th/7th consensus guidelines (PMID 38896983) address management of advanced/metastatic IBC within the broader metastatic breast cancer framework.
Sources: Schwartz's Principles of Surgery, 11e, p. 629 | Current Surgical Therapy, 14e, pp. 805-806 | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.