I now have comprehensive material across all mechanisms. Here is the complete answer:
Mechanisms of Coma in Diabetes Mellitus
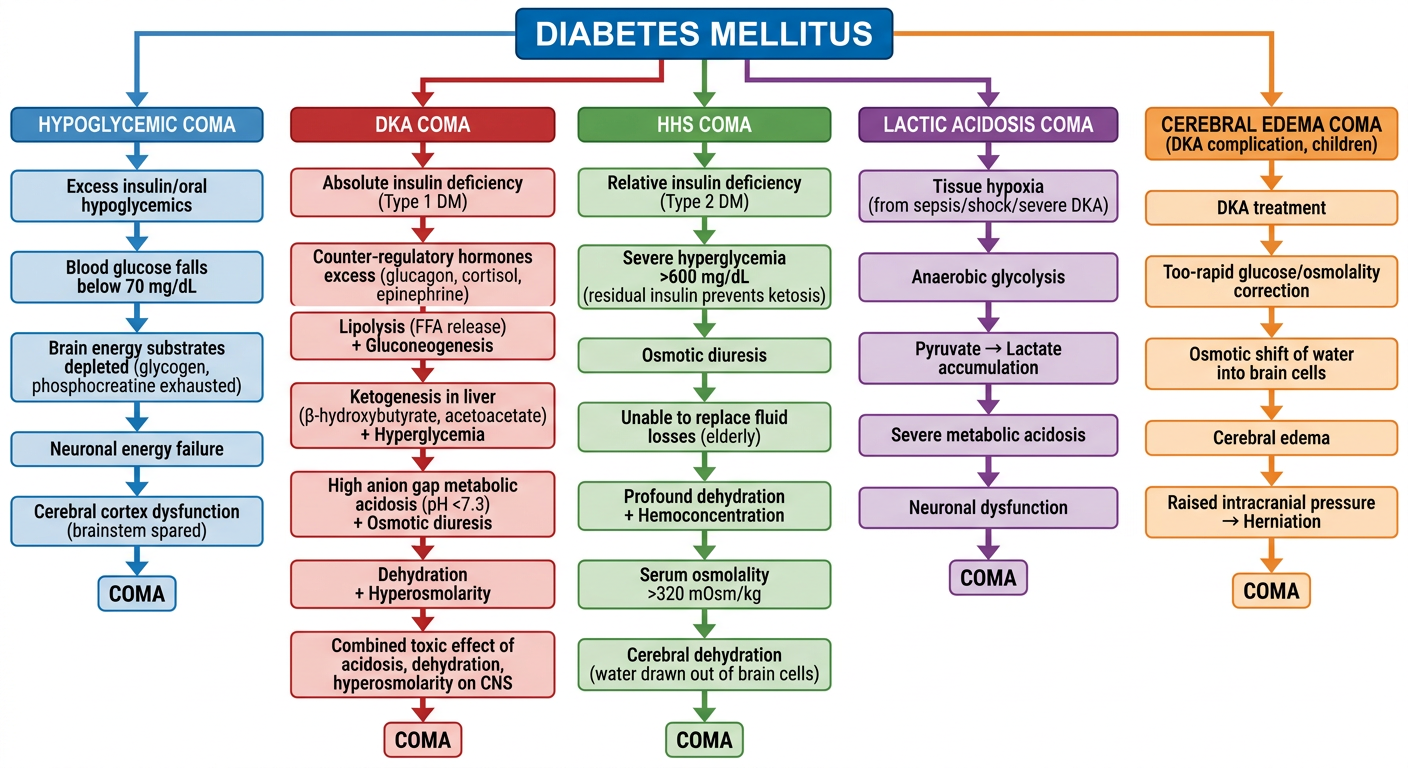
Diabetes mellitus can produce coma through five distinct mechanisms, each with its own pathophysiology, clinical profile, and treatment. As Ganong's Review of Medical Physiology summarizes: "Coma in diabetes can be due to acidosis and dehydration. However, the plasma glucose can be elevated to such a degree that independent of plasma pH, the hyperosmolarity of the plasma causes unconsciousness. Accumulation of lactate in the blood (lactic acidosis) may also complicate diabetic ketoacidosis if the tissues become hypoxic... Brain edema occurs in about 1% of children with ketoacidosis, and it can cause coma."
1. Hypoglycemic Coma
Mechanism
This is the most common cause of coma in a known diabetic and arises from excessive insulin or oral hypoglycemic agents (especially sulfonylureas) relative to glucose availability.
The brain depends on glucose as its primary energy substrate. As blood glucose falls:
- At 31-46 mg/dL (1.7-2.6 mM): cerebral glucose consumption declines but oxygen consumption remains normal; decision-making slows
- Below ~1.0 mM/dL: energy reserves collapse, the EEG becomes isoelectric
The brain has limited backup stores - astrocyte glycogen, lactate, phosphocreatine - but these are exhausted rapidly in sustained hypoglycemia.
Pathologically, hypoglycemia damages the cerebral hemispheres preferentially (laminar/pseudolaminar cortical necrosis in fatal cases) while largely sparing the brainstem - the opposite pattern to hypoxia. (Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 385)
Clinical Features
Presents in four forms:
- Quiet delirium - sleepy confusion
- Manic delirium - wild, agitated behavior
- Coma with multifocal brainstem signs - neurogenic hyperventilation, decerebrate spasms, hypothermia (33-35°C); pupillary light reactions and oculomotor responses are usually preserved (distinguishing it from structural coma)
- Stroke-like focal deficits - transient focal neurological signs, with or without coma
A critical point: alcohol alone can cause severe hypoglycemia, so blood glucose must be checked in all patients with altered consciousness even when alcohol intoxication seems the obvious explanation.
Key Lab
Blood glucose < 70 mg/dL (typically < 50 mg/dL in symptomatic cases); low or absent serum ketones; normal or mildly elevated lactate.
Treatment
IV dextrose (D50W) immediately; thiamine must be given before glucose in malnourished patients to avoid precipitating Wernicke's encephalopathy.
2. Diabetic Ketoacidosis (DKA) Coma
Mechanism
DKA is caused by absolute or relative insulin deficiency combined with excess counter-regulatory hormones (glucagon, epinephrine, cortisol). The hormonal milieu causes:
- Lipolysis - adipose tissue releases free fatty acids (FFAs)
- Ketogenesis - the liver converts FFAs → β-hydroxybutyrate, acetoacetate, acetone
- Gluconeogenesis - muscle delivers amino acids, lactate, and pyruvate to the liver for glucose production
- Hyperglycemia → osmotic diuresis → dehydration, hemoconcentration
- Accumulation of ketoacids → high anion gap metabolic acidosis (pH < 7.3, bicarbonate < 15 mmol/L)
Coma results from the combined toxic effects of acidosis, dehydration, and hyperosmolarity on the nervous system. (Ganong's, p. 443)
Typically seen in Type 1 diabetes (though also in insulin-deficient Type 2 under physiologic stress, sepsis, steroids, or SGLT2 inhibitor use). (Katzung's Basic and Clinical Pharmacology, 16th Ed.)
Clinical Features
- Gradual onset over hours to days
- Polyuria, polydipsia, weakness, nausea, vomiting
- Deep slow Kussmaul breathing (respiratory compensation for acidosis)
- Fruity/acetone breath
- Dehydration, tachycardia, hypotension
- Mental status changes ranging from confusion to frank coma
- Abdominal pain (can mimic acute abdomen)
Key Labs
| Parameter | Finding in DKA |
|---|
| Blood glucose | Elevated (often 250-600 mg/dL, though can be lower in euglycemic DKA) |
| Arterial pH | < 7.3 (severe < 7.0) |
| Bicarbonate | < 15 mmol/L |
| Anion gap | Elevated |
| Ketones | Strongly positive (β-hydroxybutyrate predominates) |
| Serum osmolality | Elevated but usually < 320 mOsm/kg |
(Goldman-Cecil Medicine, Table 210-12)
Treatment
Aggressive IV hydration, insulin infusion (~0.1 U/kg/h regular insulin IV), potassium and electrolyte replacement, and treatment of the precipitating cause.
3. Hyperosmolar Hyperglycemic State (HHS) Coma
Mechanism
In HHS, extreme hyperglycemia (glucose > 600 mg/dL) with severe dehydration produces a hyperosmolar state (serum osmolality > 320 mOsm/kg). The mechanism of coma is direct hyperosmolarity, which is independent of pH.
Why no significant ketosis in HHS? Because residual insulin secretion in Type 2 diabetics is sufficient to suppress lipolysis but insufficient to control hyperglycemia. Without lipolysis, there is no substrate for ketogenesis.
The sequence is:
- Inadequate fluid intake (elderly, disabled) cannot compensate for glucose-induced osmotic diuresis
- Progressive hemoconcentration and dehydration worsen hyperglycemia
- Prerenal renal impairment further reduces glucose excretion
- Rising osmolality draws water out of brain cells → cerebral dehydration → coma
"The clinical severity and levels of consciousness generally correlate with the severity and duration of hyperosmolarity. Up to 10% of patients with the hyperosmolar hyperglycemic state present with frank coma." (Goldman-Cecil Medicine)
Typical patient: elderly Type 2 diabetic, often precipitated by infection, dehydration, diuretics, steroids, or phenytoin.
Clinical Features
- Gradual onset over days to weeks
- Profound dehydration, weight loss
- Neurological symptoms ranging from confusion to stupor to coma
- Seizures (focal or generalized)
- No Kussmaul breathing (no significant acidosis)
- No acetone breath
Key Labs
| Parameter | Finding in HHS |
|---|
| Blood glucose | > 600 mg/dL (often 800-1200 mg/dL) |
| Serum osmolality | > 320 mOsm/kg (often 350-380) |
| Arterial pH | > 7.3 (normal or near-normal) |
| Bicarbonate | > 18 mmol/L |
| Ketones | Absent or trace |
Treatment
Aggressive IV rehydration (the cornerstone), careful electrolyte correction, low-dose insulin (after initial hydration), and treatment of precipitating cause. The rate of correction must be monitored carefully - too rapid a fall in osmolality risks cerebral edema.
4. Lactic Acidosis Coma
Mechanism
Lactic acidosis can occur in diabetes as a complication of DKA when tissues become hypoxic (e.g., from severe dehydration, shock, or sepsis), or independently from metformin use in patients with renal failure. Lactic acid accumulates when aerobic metabolism is impaired and pyruvate is shunted to lactate.
Lactic acidosis itself can cause coma via severe metabolic acidosis affecting neuronal function. Adams and Victor's notes: "Lactic acidosis may affect the brain by lowering arterial blood [pH]."
This is important because in DKA, the nitroprusside-based ketone test detects acetoacetate but not β-hydroxybutyrate and does not detect lactate - so co-existing lactic acidosis can be underestimated without a direct lactate measurement.
Key Labs
- Blood lactate > 5 mmol/L (severe lactic acidosis)
- High anion gap metabolic acidosis
- Elevated lactate:pyruvate ratio
5. Cerebral Edema (especially in Children with DKA)
Mechanism
Cerebral edema complicates approximately 1% of children with DKA and carries a mortality of ~25%. The exact mechanism is debated but likely involves:
- Rapid osmotic shifts during treatment (too-rapid correction of hyperglycemia and hyperosmolality)
- Possibly vasogenic edema from cerebral ischemia during DKA
- Aquaporin-mediated water shifts
This is a distinct mechanism from the metabolic/osmotic causes above - it is a structural complication causing coma via raised ICP and herniation. (Ganong's Review of Medical Physiology, p. 443)
Summary Comparison Table
| Feature | Hypoglycemic Coma | DKA Coma | HHS Coma | Lactic Acidosis | Cerebral Edema (DKA) |
|---|
| DM type | T1 > T2 | T1 (mainly) | T2 (mainly) | T1/T2 | T1 (children) |
| Blood glucose | Low (< 70) | Elevated (250-600) | Very high (> 600) | Variable | Elevated (during DKA) |
| Ketones | Absent | Strongly positive | Absent/trace | May be present | Positive |
| pH | Normal | < 7.3 | > 7.3 | Very low | < 7.3 |
| Osmolality | Normal | Mildly elevated | Markedly elevated (> 320) | Variable | Elevated then dropping |
| Onset | Rapid (minutes) | Hours to days | Days to weeks | Variable | During/after DKA treatment |
| Breathing | Normal or irregular | Kussmaul | Normal | Variable | Normal initially |
| Key mechanism | Energy failure (no glucose substrate) | Acidosis + dehydration + hyperosmolarity | Hyperosmolarity | Severe acidosis | Raised ICP/herniation |
| Immediate Rx | IV dextrose | IV fluids + insulin | IV fluids | IV fluids + treat cause | Mannitol + slow glucose correction |
Sources:
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, 5th Ed., pp. 385, 397
- Ganong's Review of Medical Physiology, 26th Ed., pp. 442-443
- Goldman-Cecil Medicine, International Ed.
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 1198