Oxygen dissociation curve for md emergency medicine exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I have rich, comprehensive material. Now let me compile the full exam-focused answer.
Oxygen Dissociation Curve - MD Emergency Medicine Exam
The Curve
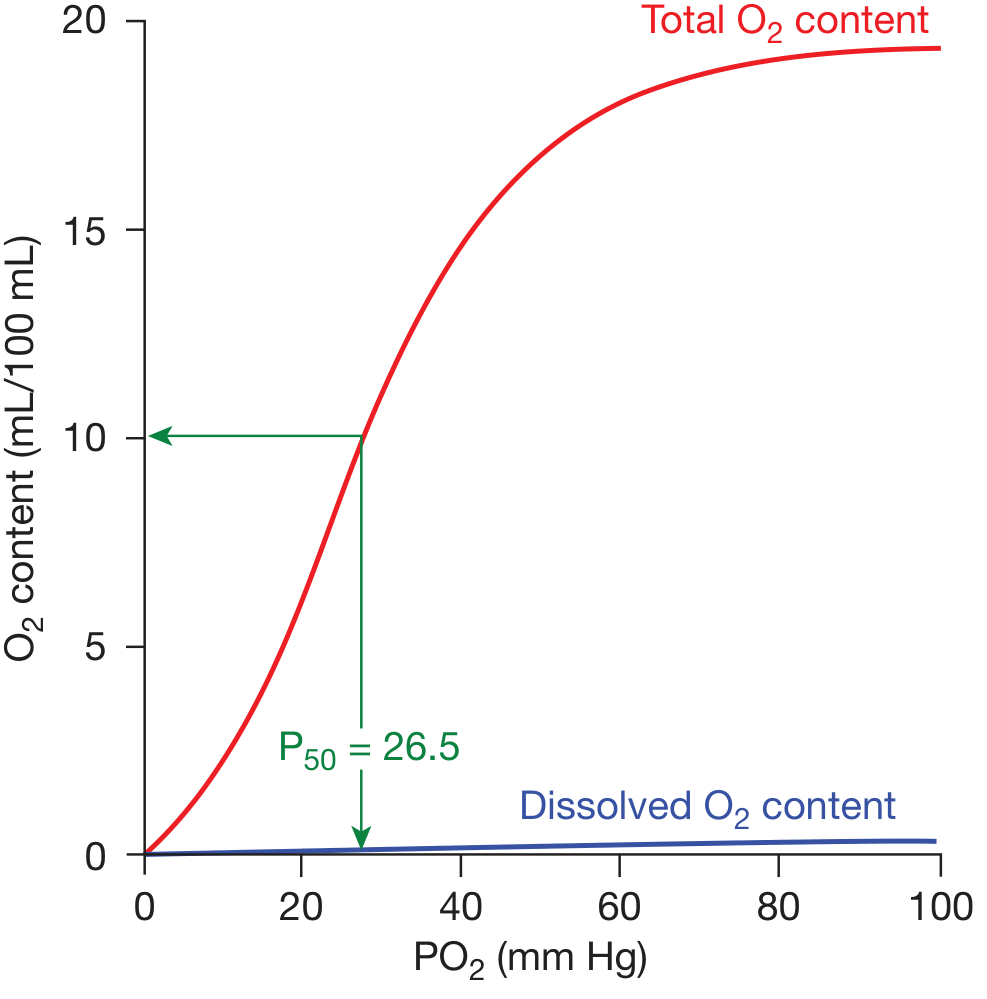
Figure: Oxygen dissociation curve. Red line = total O2 content (Hb-bound + dissolved). Blue line = dissolved O2 only. P50 = 26.5 mmHg. (Fishman's Pulmonary Diseases and Disorders)
What the Curve Represents
The ODC shows the relationship between the partial pressure of oxygen (PaO2) and the percent saturation of hemoglobin with oxygen (SpO2). It is sigmoid (S-shaped), not hyperbolic - a direct consequence of cooperative O2 binding by hemoglobin's four subunits.
- Fishman's Pulmonary Diseases, block3
Why sigmoid matters (exam point): Each O2 molecule that binds to hemoglobin increases the affinity of the remaining heme groups for O2 (cooperativity). The net result is that affinity for the last O2 bound is ~300x greater than for the first - Lippincott Biochemistry 8e.
Key Values to Memorize
| Parameter | Normal Value |
|---|---|
| PaO2 in arterial blood (lungs) | ~95-100 mmHg |
| SpO2 at 100 mmHg PaO2 | ~97-100% |
| PaO2 in mixed venous blood (rest) | ~40 mmHg |
| SpO2 at 40 mmHg PaO2 | ~75% |
| P50 (PaO2 at 50% SpO2) | ~26.5 mmHg |
| Critical threshold PaO2 | 60 mmHg (~90% SpO2) |
Two Critical Zones of the Curve
1. Upper Flat Portion (PaO2 60-100 mmHg)
- Hemoglobin remains ~90-100% saturated
- Clinical advantage: Even with lung disease dropping PaO2 from 100 to 60 mmHg, SpO2 remains adequate (~90%)
- This is why you can tolerate moderate hypoxemia without catastrophic desaturation
2. Lower Steep Portion (PaO2 20-60 mmHg)
- Small drops in PaO2 cause large drops in saturation
- Clinical advantage for tissues: Large amounts of O2 are released per small drop in PO2, promoting efficient diffusion into metabolizing tissues
- At rest, only ~25% of delivered O2 is extracted; the remaining 75% is reserve
- The "slippery slope" - once PaO2 drops below 60 mmHg, rapid desaturation follows
Allosteric Effectors & Curve Shifts
Bohr Effect (pH and CO2)
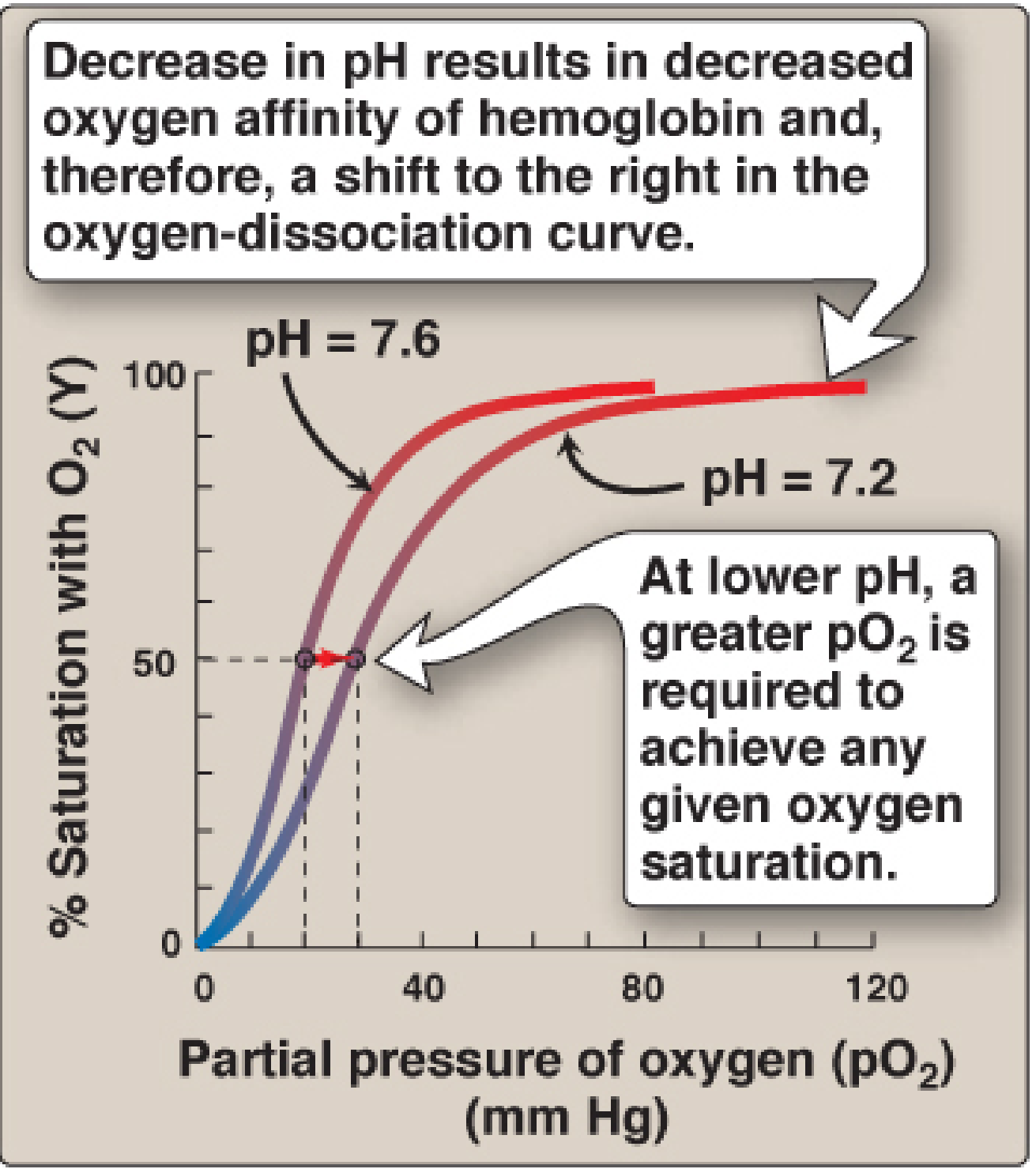
Figure: Bohr effect - decreased pH shifts curve right (decreased Hb-O2 affinity). - Lippincott Biochemistry 8e
The mnemonic CADET face right covers all right-shift causes:
- CO2 increased
- Acid (decreased pH)
- DPG (2,3-DPG/BPG) increased
- Exercise (increased temperature)
- Temperature increased
Table: Factors Shifting the ODC
| RIGHT Shift (↓ Hb-O2 affinity, more O2 released to tissues) | LEFT Shift (↑ Hb-O2 affinity, more O2 held by Hb) |
|---|---|
| ↑ CO2 (↑ pCO2) | ↓ CO2 |
| ↓ pH (acidosis) | ↑ pH (alkalosis) |
| ↑ Temperature | ↓ Temperature |
| ↑ 2,3-DPG/BPG | ↓ 2,3-DPG/BPG |
| Exercise | Stored blood (DPG depleted) |
| Anemia, COPD (compensatory ↑ DPG) | Fetal Hb (HbF) |
| Sickle cell Hb (HbS) | Carboxyhemoglobin (COHb) |
| High altitude (chronic, via ↑ DPG) | Methemoglobin |
| High altitude (acute) |
- Mulholland & Greenfield's Surgery 7e, Guyton & Hall Physiology
Right shift = good for tissues (O2 unloaded more readily). P50 increases.
Left shift = good for lungs (O2 loaded more readily). P50 decreases.
2,3-BPG (2,3-Bisphosphoglycerate) - High-Yield
- Most abundant organic phosphate in RBCs; synthesized from glycolytic intermediates
- Binds exclusively to deoxyhemoglobin (T form) in the central pocket formed by the two β-globin chains
- Oxygenation narrows this pocket, expelling 2,3-BPG
- Effect: shifts ODC right → more O2 released to tissues
2,3-BPG increases in:
- Chronic hypoxia (COPD, high altitude)
- Chronic anemia
- Compensatory response to improve tissue O2 delivery
2,3-BPG decreases in:
-
Stored blood (blood bank) - acts as an O2 "trap" rather than delivery system; replenished within 6-24 hours post-transfusion
-
Transfusing large volumes of old blood is dangerous in critically ill patients
-
Lippincott Biochemistry 8e
Bohr Effect - Mechanism (Exam Depth)
In metabolically active tissues:
- CO2 is produced → converted by carbonic anhydrase to H2CO3 → HCO3- + H+
- ↑ H+ lowers pH in tissue capillaries
- H+ binds histidine residues on deoxyhemoglobin (higher pKa than oxyhemoglobin) → forms salt bridges → stabilizes T (deoxy) form
- Result: O2 is released in tissues
In pulmonary capillaries:
- CO2 is exhaled → pH rises → equilibrium shifts toward oxyhemoglobin → O2 is loaded
Represented as: HbO2 + H+ ⇌ HbH + O2
Fetal Hemoglobin (HbF) - Left Shift
- HbF has γ-chains instead of β-chains
- 2,3-BPG binds poorly to γ-chains → HbF has lower affinity for 2,3-BPG → higher O2 affinity
- ODC is left-shifted relative to adult HbA
- Physiological advantage: allows fetus to extract O2 from maternal blood at the placenta
- Clinical note: HbF's P50 is ~20 mmHg vs ~26.5 mmHg for HbA
Carbon Monoxide (CO) - Left Shift + Haldane Effect
- CO binds hemoglobin with 240x greater affinity than O2 → forms carboxyhemoglobin (COHb)
- Dual problem:
- Reduces O2-carrying capacity (fewer sites for O2)
- Left-shifts the ODC for remaining Hb sites - O2 that is bound is not released to tissues
- This is why CO poisoning is so deadly even at moderate COHb levels
- SpO2 on pulse oximetry reads falsely normal (cannot distinguish OxyHb from COHb)
Myoglobin vs Hemoglobin
| Feature | Myoglobin | Hemoglobin |
|---|---|---|
| Structure | Monomer | Tetramer |
| Curve shape | Hyperbolic | Sigmoid |
| O2 affinity | High (always) | Variable (allosteric) |
| P50 | ~2-3 mmHg | ~26.5 mmHg |
| Cooperativity | No | Yes |
| Function | O2 storage (muscle) | O2 transport (blood) |
| 2,3-BPG effect | None | Decreases affinity (right shift) |
A hyperbolic curve (myoglobin) cannot deliver O2 to tissues efficiently - it would hold O2 throughout the range of tissue pO2. The sigmoid ODC allows hemoglobin to load in high-pO2 lungs and unload in low-pO2 tissues. - Lippincott Biochemistry 8e
Clinical Emergency Scenarios (High Yield)
1. Septic Shock / Lactic Acidosis
- ↓ pH + ↑ CO2 + ↑ temperature → right shift → facilitates O2 unloading to ischemic tissues
- Compensatory but may be overwhelmed if cardiac output fails
2. Massive Transfusion
- Stored RBCs are 2,3-BPG depleted → left shift → O2 remains bound, not delivered to tissues
- Use fresh blood or "rejuvenated" blood when possible; 2,3-BPG restores in 6-24 hrs
3. CO Poisoning
- SpO2 falsely normal on pulse ox - always measure COHb directly with co-oximetry
- Left-shifted ODC + reduced capacity = tissue hypoxia despite apparent normal sats
- Treatment: 100% O2 (displaces CO), hyperbaric O2 in severe cases
4. High Altitude / COPD (Chronic Hypoxia)
- Compensatory ↑ 2,3-BPG → right shift → improves O2 delivery to tissues
- Guyton & Hall: BPG mechanism allows O2 release at up to 10 mmHg higher tissue pO2
5. Alkalosis (Hyperventilation / Over-correction of Acidosis)
- ↑ pH → left shift → Hb holds O2 → tissue hypoxia despite adequate PaO2
- Clinically relevant during aggressive bicarbonate administration or excessive ventilation
6. Hypothermia
- ↓ Temperature → left shift → reduced O2 delivery, but also reduced metabolic demand (protective in therapeutic hypothermia post-cardiac arrest)
Quick Memory Frame
RIGHT shift = "HEAT" releases O2
↑ H+ ↑ CO2 ↑ Temperature ↑ 2,3-DPG
→ more O2 to tissues (P50 goes UP)
LEFT shift = "COLD stored fetal blood"
↓ H+ ↓ CO2 ↓ Temperature ↓ 2,3-DPG
HbF, COHb, MetHb
→ Hb holds O2 (P50 goes DOWN)
Sources: Fishman's Pulmonary Diseases and Disorders | Lippincott Illustrated Reviews: Biochemistry, 8e | Guyton and Hall Textbook of Medical Physiology | Mulholland & Greenfield's Surgery 7e
This is a shared conversation. Sign in to Orris to start your own chat.