What is EtCO2
Reading File
Searching the Web
EtCO2 end-tidal CO2 clinical significance capnography
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a thorough explanation of EtCO2 drawing from authoritative anesthesia and emergency medicine textbooks.
EtCO2 (End-Tidal Carbon Dioxide)
Definition
EtCO2 (also written ETCO2 or PetCO2) is the partial pressure of CO2 measured at the very end of a fully exhaled breath. It represents the peak CO2 concentration in exhaled gas and is the best non-invasive reflection of alveolar CO2 - and by extension, arterial PaCO2.
- Normal range: 35-45 mmHg (or 5-6% CO2)
- EtCO2-to-PaCO2 gradient: typically 2-5 mmHg in healthy patients (EtCO2 is slightly lower than PaCO2)
How It Is Measured - Capnography
Capnography is the technology used to measure and display EtCO2. It produces a waveform (capnogram) over time using infrared light absorption by CO2 molecules. Two main configurations exist:
- Sidestream (aspirating): Gas is drawn from the airway circuit via a small tube to a remote sensor. The sensor is away from the patient.
- Mainstream (non-aspirating): The sensor sits directly in line with the airway circuit; no gas sampling tube is needed.
Capnography can also be volumetric (CO2 vs. exhaled volume) rather than time-based, which allows for dead space calculations and PEEP optimization.
The Normal Capnogram Waveform
The classic capnogram has 4 phases (A through E):
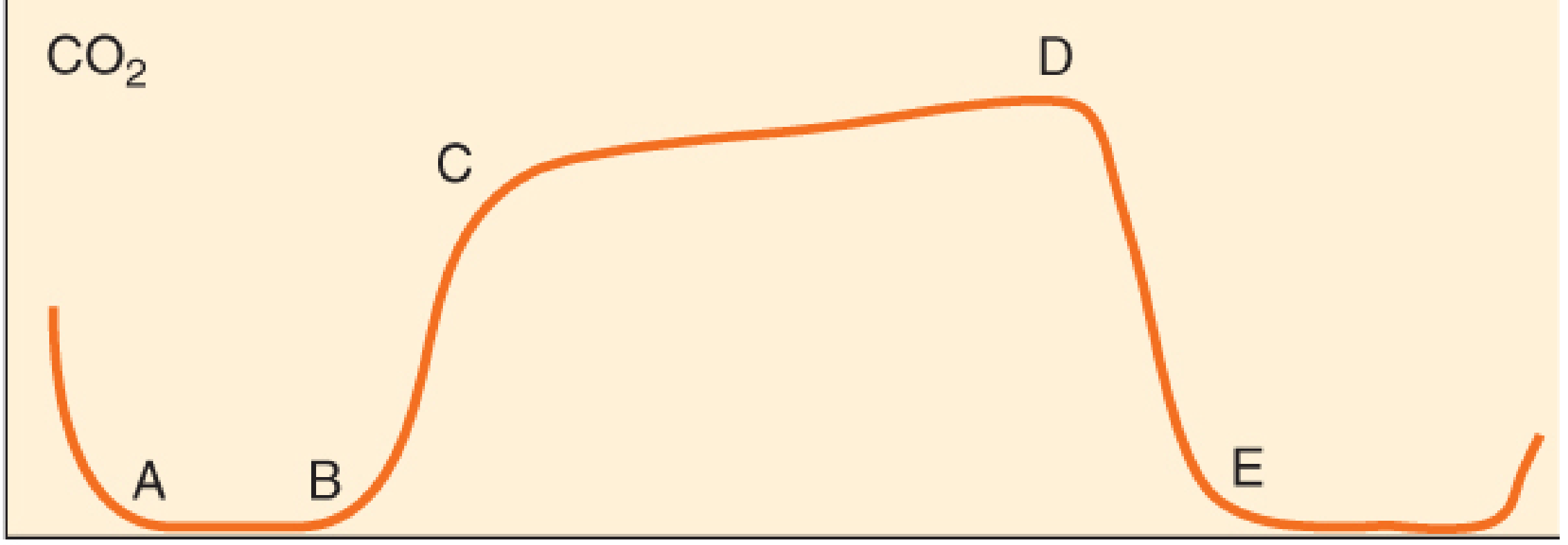
| Phase | Description |
|---|---|
| A-B | Early expiration - anatomic dead space gas; no CO2 present |
| B-C | Sharp upstroke - CO2-containing alveolar gas begins to appear |
| C-D | Alveolar/expiratory plateau - near-horizontal; pure alveolar gas |
| D | Peak point = EtCO2 (highest CO2 reading of the breath) |
| D-E | Steep downstroke as fresh inspiratory gas enters |
- Barash's Clinical Anesthesia, 9e; Miller's Anesthesia, 10e
Clinical Uses
1. Confirm Endotracheal Tube Placement
Stable EtCO2 waveform for 3 or more successive breaths confirms tracheal placement (not esophageal). The ASA mandates EtCO2 monitoring during general anesthesia and moderate/deep sedation as a standard of care.
2. Monitor Ventilation Continuously
EtCO2 provides real-time, breath-by-breath ventilation monitoring without repeated blood gas sampling. When sedated patients hypoventilate, EtCO2 rises; when apnea occurs, EtCO2 drops to zero. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
3. CPR Quality and ROSC Detection
- EtCO2 during CPR reflects cardiac output and pulmonary blood flow
- Target EtCO2 >20 mmHg (Harriet Lane Handbook) or >12-15 mmHg (Tintinalli's Emergency Medicine) during compressions
- A sudden spike in EtCO2 during CPR often signals return of spontaneous circulation (ROSC) before a pulse is detectable
4. Dead Space Calculation
The alveolar dead space fraction (AVDSf) can be estimated:
AVDSf = (PaCO2 - PetCO2) / PaCO2
An increasing gradient between PaCO2 and EtCO2 signals increased alveolar dead space (e.g., PE, low cardiac output, pulmonary overdistension). - Miller's Anesthesia, 10e
Causes of Changes in EtCO2
| EtCO2 Increases | EtCO2 Decreases |
|---|---|
| Hypoventilation | Hyperventilation |
| Sepsis | Hypothermia |
| Hyperthermia | Hypothyroidism |
| Malignant hyperthermia | Pulmonary embolism |
| Shivering | Hypoperfusion / low cardiac output |
| Hyperthyroidism | Cardiac arrest |
| Rebreathing (exhausted CO2 absorber) | Apnea |
| Bicarbonate administration | Air embolism |
- Barash's Clinical Anesthesia, 9e
Key pattern rules:
- Abrupt drop toward zero = circulatory catastrophe (PE, cardiac arrest, circuit disconnection, tube dislodgement)
- Gradual decline = increasing ventilation or decreasing CO2 production
- Slow upslope on B-C phase = obstructive disease (COPD, asthma)
- Rising C-D plateau (shark fin pattern) = bronchospasm or airway obstruction
- Non-zero baseline = CO2 rebreathing (exhausted absorber or valve malfunction)
Summary
EtCO2 is a powerful, non-invasive, continuous monitor of ventilation, circulation, and metabolism. It is mandatory in anesthesia, widely used in emergency medicine and critical care, and provides instantaneous feedback that arterial blood gases simply cannot match in real time.
This is a shared conversation. Sign in to Orris to start your own chat.