Hello
Hello! I'm Orris. How can I help you today?
Carpopedal syndrome
Reading File
Finding Sources
Searching PubMed
carpopedal spasm tetany hypocalcemia
Reading File
Reading File
Loading Image
Here is a thorough overview of carpopedal spasm (sometimes loosely called "carpopedal syndrome"):
Carpopedal Spasm
Definition
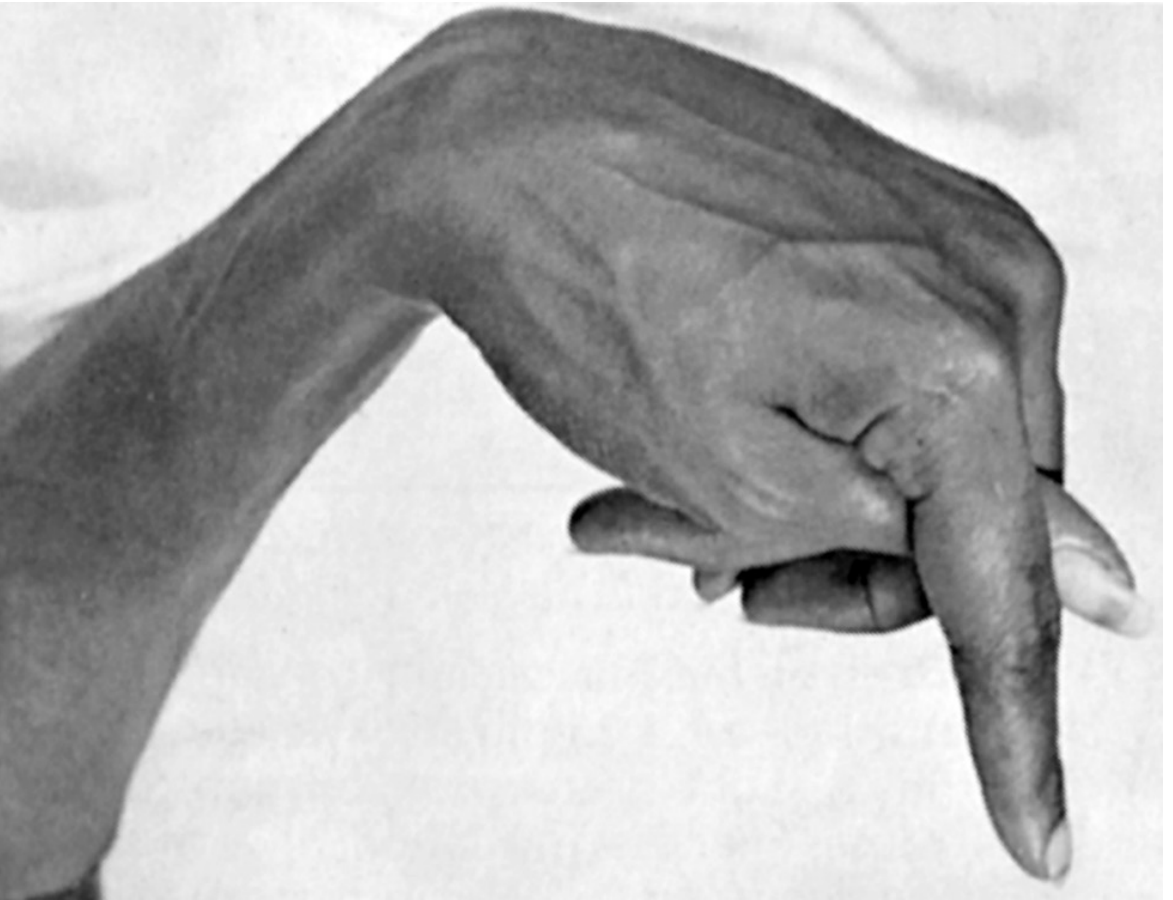
Carpopedal spasm is an involuntary, sustained tetanic contraction of the muscles of the hands (carpo-) and feet (pedo-). It is not a stand-alone "syndrome" per se but rather the hallmark clinical manifestation of tetany, most commonly driven by hypocalcemia. It is sometimes called the "main d'accoucheur" (obstetrician's hand) posture in the hand.
Pathophysiology
When extracellular calcium falls, neuronal membrane permeability to sodium increases, lowering the threshold for action potential generation. Peripheral nerve fibers become so excitable they discharge spontaneously, sending trains of impulses to skeletal muscles - resulting in sustained (tetanic) contractions. The hands are typically affected first, producing the characteristic flexed-wrist, flexed-MCP, extended-IP joint posture.
- Normal serum calcium: ~9.4 mg/dL
- Tetany typically appears at: ~6 mg/dL (35% below normal)
- Lethal level: ~4 mg/dL
(Guyton and Hall Textbook of Medical Physiology)
Causes
| Mechanism | Examples |
|---|---|
| Hypocalcemia | Hypoparathyroidism (post-thyroidectomy, autoimmune), vitamin D deficiency, chronic renal failure, hypomagnesemia, pancreatitis, proton pump inhibitor use |
| Hypomagnesemia | Leads to hypocalcemia via impaired PTH secretion; causes neuromuscular hyperexcitability independently |
| Respiratory alkalosis | Hyperventilation (anxiety, heat exposure) lowers ionized Ca²+ by increasing protein binding |
| Metabolic alkalosis | Same mechanism - reduced ionized fraction |
Clinical Features of Hypocalcemia / Tetany
From Goldman-Cecil Medicine, the features of neuromuscular irritability include:
- Paresthesias of fingers, toes, and circumoral region (often earliest symptom)
- Tetanic carpopedal spasm and muscle cramps
- Chvostek sign - twitching of circumoral muscles on tapping the facial nerve just anterior to the ear (present in ~10% of normal individuals)
- Trousseau sign - carpal spasm elicited by inflating a BP cuff to 20 mmHg above systolic pressure for 3 minutes (more specific than Chvostek)
- Laryngospasm and bronchospasm
- Seizures (focal, grand mal, or syncope)
- Prolonged QT interval on ECG
- Confusion
Additional features noted in Morgan & Mikhail's Clinical Anesthesiology include masseter spasm and cardiac irritability.
Key Clinical Associations
Post-thyroidectomy / parathyroidectomy: Inadvertent removal or devascularization of parathyroid glands causes acute hypoparathyroidism. PTH drops, serum calcium falls within 24 hours, and carpopedal spasm with orofacial tingling appears. This is a medical emergency. (Gray's Anatomy for Students; Schwartz's Principles of Surgery)
Hyperventilation tetany: During heat exhaustion or anxiety, rapid breathing causes respiratory alkalosis, reducing ionized calcium. Produces paresthesias and carpopedal spasm with minimal muscle pain (distinguishing it from heat cramps). (Harrison's Principles of Internal Medicine 22e; Rosen's Emergency Medicine)
Hypomagnesemia: Significant Mg²+ depletion impairs PTH release, causing secondary hypocalcemia and carpopedal spasm, seizures, muscular weakness, and cardiac arrhythmias. (Henry's Clinical Diagnosis and Management by Laboratory Methods)
Workup
For hypocalcemia-driven carpopedal spasm, investigate:
| Test | Interpretation |
|---|---|
| Serum calcium (total + ionized) | Low in true hypocalcemia |
| Serum albumin | Correct for hypoalbuminemia |
| Serum magnesium | Hypomagnesemia impairs PTH |
| PTH | Low = hypoparathyroidism; high = secondary cause |
| 25-OH-D3 | Low in vitamin D deficiency |
| 1,25(OH)₂D3 | Low in chronic renal failure |
| Phosphate | High in hypoparathyroidism / CKD |
| Creatinine | Assess renal function |
| ABG | Assess for alkalosis if hyperventilation suspected |
Treatment
Acute symptomatic hypocalcemia (tetany/seizures):
- IV calcium gluconate 10 mL of 10% solution (2.20 mmol Ca²+) diluted in 50 mL of 5% dextrose or 0.9% NaCl, given slowly over >5 minutes
- Can repeat as needed; persistent cases require a calcium gluconate infusion (e.g., 10 ampules diluted and infused over several hours)
- Monitor serum calcium regularly
Chronic management:
- Oral calcium supplements + vitamin D (calcitriol for hypoparathyroidism)
- Address underlying cause (Mg²+ replacement if hypomagnesemic, correct alkalosis, etc.)
Hyperventilation tetany:
- Reassurance + removing the patient from the heat/stressor
- Rebreathing techniques to correct alkalosis
(Goldman-Cecil Medicine; Schwartz's Principles of Surgery)
Summary: Carpopedal spasm is the clinical fingerprint of tetany, most often from hypocalcemia. The key diagnostic bedside signs are Chvostek and Trousseau. Workup targets the calcium-PTH-vitamin D axis, and acute treatment is IV calcium gluconate.
This is a shared conversation. Sign in to Orris to start your own chat.