ETIOPATHOGENESIS, Clinical features, INVESTIGATION and MANAGEMENT of ACUTE RHEUMATIC FEVER. University Exam Final Year MBBS ( LAQ ). Harrison reference
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have very comprehensive data from Harrison's 22E, Robbins, and Goldman-Cecil. I have enough to write a thorough, exam-ready long answer question response. Let me compile it now.
ACUTE RHEUMATIC FEVER (ARF)
Final Year MBBS - Long Answer Question | Harrison's Principles of Internal Medicine 22E (2025)
DEFINITION
Acute Rheumatic Fever (ARF) is a multisystem inflammatory disease resulting from an autoimmune reaction to infection with Group A Streptococcus (GAS) (Streptococcus pyogenes). Almost all manifestations resolve completely except for cardiac valvular damage (Rheumatic Heart Disease - RHD), which may persist after other features resolve.
- Harrison's 22E, Chapter 371
EPIDEMIOLOGY
- Primarily affects children aged 5-14 years; rare after age 30
- Initial episodes rare in adults; recurrent episodes remain common in adolescents and young adults
- RHD prevalence peaks at 25-40 years of age
- No clear gender association for ARF; RHD is more common in females (up to 2x)
- Global burden: >40 million with RHD, >300,000 deaths annually; 95% in low- and middle-income countries (LMICs)
- Highest burden in: sub-Saharan Africa, Pacific nations, South/Central Asia, Australasia
ETIOPATHOGENESIS
1. Organism Factors (Group A Streptococcus)
- Classically caused by GAS pharyngitis (upper respiratory tract infection)
- Certain M-protein serotypes (types 1, 3, 5, 6, 14, 18, 19, 24, 27, 29) are classically "rheumatogenic" - but many more serotypes are now known to be rheumatogenic
- Recent evidence also implicates skin infection in ARF pathogenesis
- The 2-3 week latent period between infection and ARF onset reflects the time needed to mount an immune response
- Skin streptococcal infections are never associated with ARF (unlike post-streptococcal glomerulonephritis, which can follow either throat or skin infection)
2. Host Factors (Genetic Susceptibility)
- Only 3-6% of any population are susceptible to ARF, suggesting strong genetic predisposition
- This proportion does not vary dramatically between populations
- HLA class II antigens (HLA-DR7, HLA-DR4) are associated with susceptibility
- Familial clustering supports a genetic basis
3. Pathogenetic Mechanism - Molecular Mimicry
The central mechanism is molecular mimicry (Type II and Type IV hypersensitivity):
- GAS M protein contains epitopes structurally similar to human cardiac proteins (myosin, tropomyosin, laminin, vimentin)
- Antibodies directed against streptococcal M proteins cross-react with cardiac antigens (pericardial, myocardial, valvular)
- CD4+ T cells directed against M protein also recognize cardiac antigens
- Antibody binding activates complement and recruits Fc-receptor-bearing cells (neutrophils, macrophages)
- Cytokines produced by stimulated T cells lead to macrophage activation (forming Aschoff bodies in myocardium)
- Combined antibody- and T cell-mediated reactions damage heart tissue
- Chorea results from antibody binding to basal ganglia
- Arthritis is caused by immune complex deposition in joints
- Skin manifestations result from delayed hypersensitivity reactions
Key point: Streptococci are completely absent from the lesions - confirming the immunological (not infective) basis of tissue damage.
4. Pathology - Aschoff Bodies (Pathognomonic)
The Aschoff body is the pathognomonic lesion of ARF:
- Focal inflammatory lesions found in cardiac tissues
- Composed of: T lymphocytes, plasma cells, and plump activated macrophages called Anitschkow cells (also called "caterpillar cells" due to central wavy ribbon of chromatin)
- Aschoff bodies may be found in all three cardiac layers (pancarditis)
Gross/Microscopic pathology:
- Acute valvulitis: Fibrinoid necrosis within cusps/tendinous cords; small (1-2 mm) verrucae (vegetations) along lines of closure
- MacCallum plaques: Subendocardial irregular thickenings in left atrium due to regurgitant jets
- Chronic RHD: Leaflet thickening, commissural fusion, shortening and fusion of tendinous cords (leading to mitral stenosis)
- Mitral valve involved virtually always; isolated in ~2/3; with aortic valve in ~25%
(Robbins Pathologic Basis of Disease, Chapter 12)
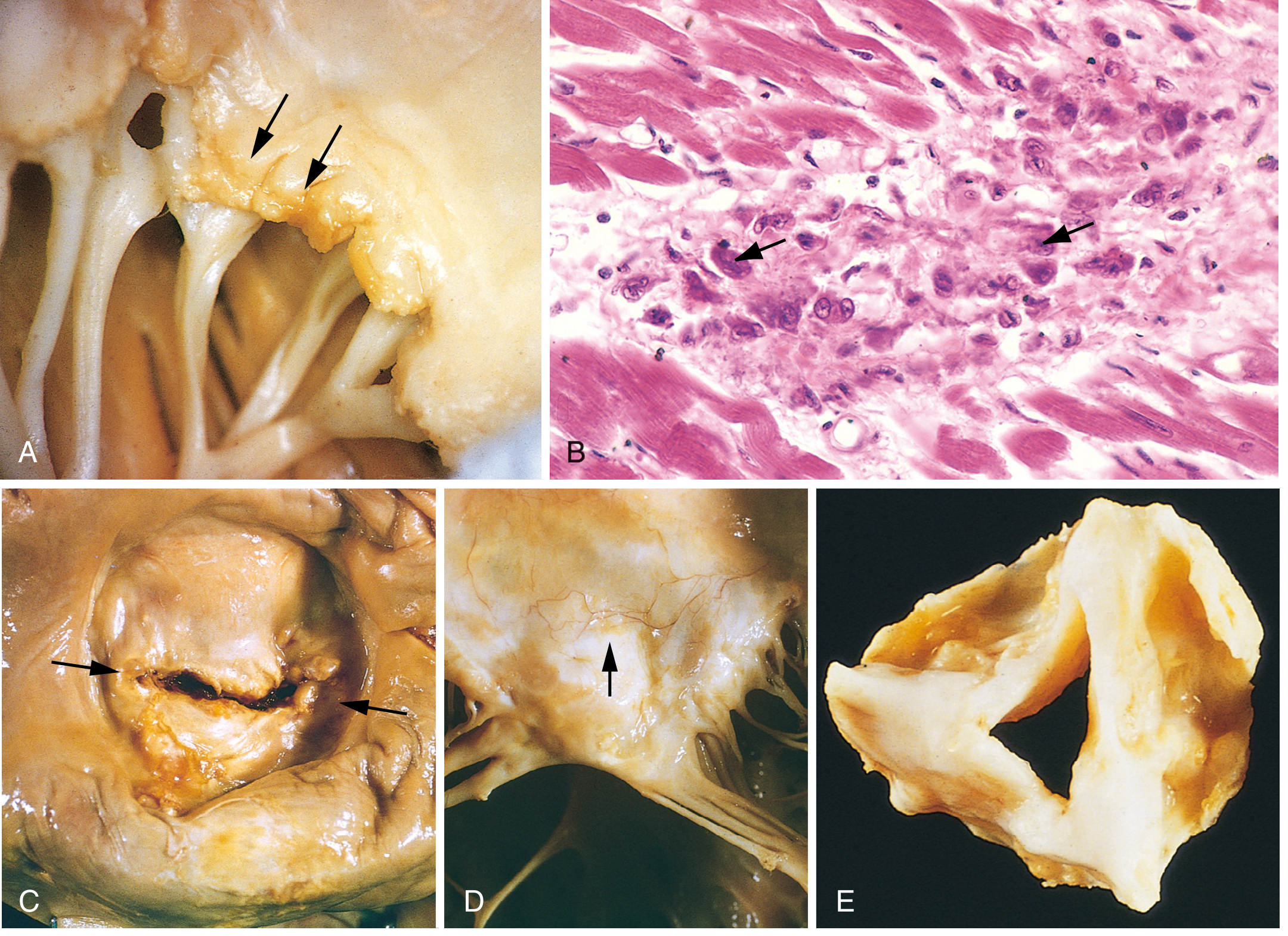
Fig. 12.22 - Robbins Pathologic Basis of Disease: Acute and chronic rheumatic heart disease
CLINICAL FEATURES
ARF typically develops 2-3 weeks after GAS pharyngitis. Manifestations are remembered by the mnemonic JONES (Jones Criteria):
Major Criteria (JONES)
| Feature | Frequency | Key Details |
|---|---|---|
| J - Joints (Arthritis) | 75% | Migratory polyarthritis of large joints (knees, ankles, elbows, wrists); exquisitely painful; fleeting |
| O - cOre (Carditis) | >50% | Pancarditis - pericarditis, myocarditis, endocarditis; murmurs (mitral regurgitation most common) |
| N - Nodules (subcutaneous) | <10% | 0.5-2 cm; painless; over bony prominences or extensor tendons |
| E - Erythema marginatum | <10% | Pink, non-pruritic, blanching macules/papules; serpiginous pattern on trunk and proximal limbs; spares face |
| S - Sydenham's Chorea | 30% | Involuntary, non-rhythmic, purposeless movements; worse unilaterally; stops during sleep; "St. Vitus' dance" |
Carditis (most important, detailed):
- Pancarditis affects all layers - endocardium, myocardium, pericardium
- Endocarditis/Valvulitis: Most significant - mitral valve most affected (mitral regurgitation = apical pansystolic murmur); aortic valve second
- Myocarditis: Tachycardia, cardiac enlargement, heart failure
- Pericarditis: Pericardial friction rub, chest pain
- ECG changes: Prolonged PR interval (1st degree AV block) is most common
- Rapid sleeping pulse and tachycardia out of proportion to fever
- Subclinical (echocardiographic) carditis exists without clinical signs
Arthritis (most common, detailed):
- Migratory polyarthritis of large joints
- Each joint affected for hours to a few days, then moves on
- Exquisitely painful, out of proportion to clinical signs
- Responds rapidly and dramatically to NSAIDs (diagnostic clue - absence of NSAID response should prompt reconsideration)
- Synovial fluid: sterile with lymphocyte predominance
- Leaves no permanent joint damage
Sydenham's Chorea:
- May appear late (up to 6 months after infection) - can occur in isolation without other ARF features
- Involuntary, non-rhythmic, purposeless movements
- Usually more pronounced on one side (hemichorea)
- Stops completely during sleep (distinguishes from other movement disorders)
- Associated with emotional lability
Minor Criteria
| Minor Criterion | Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|---|
| Arthralgia | Polyarthralgia | Monoarthralgia |
| Fever | ≥38.5°C | ≥38.5°C |
| ESR | ≥60 mm/hr | ≥30 mm/hr |
| CRP | ≥3.0 mg/dL | ≥3.0 mg/dL |
| ECG | Prolonged PR interval | Prolonged PR interval |
(Note: Arthralgia cannot be used as a minor criterion if arthritis is being used as a major criterion; prolonged PR cannot be minor if carditis is major)
INVESTIGATIONS
Always Request (Harrison's Table 371-3):
| Investigation | Purpose |
|---|---|
| ECG | Prolonged PR interval (1st-degree AV block); pericarditis changes |
| Echocardiogram | Detect subclinical valvulitis; assess severity of carditis (MANDATORY in all suspected ARF) |
| Complete Blood Count (CBC) | Normochromic normocytic anemia; leukocytosis |
| C-Reactive Protein (CRP) | Elevated in active inflammation (≥3.0 mg/dL) |
| ESR | Elevated; ≥60 mm/hr (low-risk), ≥30 mm/hr (high-risk) |
| Streptococcal serology | Antistreptolysin O (ASO) titer: elevated >200 Todd units; Anti-DNase B (more sensitive for skin infections) |
In Relevant Situations:
- Throat swab / skin sore swab: GAS culture (may be negative by time ARF presents)
- Blood cultures: To exclude infective endocarditis
- Synovial fluid aspirate: Cell count, microscopy, culture, gonococcal PCR
- Pregnancy test (if applicable)
- Creatinine (UEC): Baseline before NSAID use
To Exclude Alternative Diagnoses:
- Autoantibodies, dsDNA, anti-CCP antibodies (to exclude lupus/JIA/reactive arthritis)
- Urine for Neisseria gonorrhoeae, Chlamydia trachomatis molecular tests
- Viral serology: hepatitis, CMV, parvovirus B19, respiratory viruses
Evidence of Preceding Streptococcal Infection (mandatory for diagnosis):
- ASO titer (rises 3-6 weeks after pharyngeal infection)
- Anti-DNase B (better for skin infections, stays elevated longer)
- Throat culture (often negative by time ARF diagnosed)
- Note: Both tests together have >95% sensitivity
DIAGNOSIS - REVISED JONES CRITERIA (AHA 2015)
Evidence of preceding GAS infection is mandatory plus:
| ARF Episode | Criteria Required |
|---|---|
| Initial ARF | 2 major OR 1 major + 2 minor criteria |
| Recurrent ARF | 2 major OR 1 major + 2 minor OR 3 minor criteria |
Risk population stratification (important update in 2015 revision):
- Low-risk populations: ARF incidence <2/100,000 school-aged children/year; focus on high specificity - monoarthritis not counted as major criterion
- Moderate/High-risk populations: Higher incidence settings; focus on high sensitivity - monoarthritis is a major criterion; monoarthralgia is a minor criterion
Special circumstances (diagnosis made without full Jones criteria):
- Pure Sydenham's chorea (may occur in isolation)
- Indolent carditis (slowly progressive valvular disease discovered late)
- Recurrent ARF in patient with established RHD
(Goldman-Cecil Medicine, Table 269-3; Harrison's 22E, Chapter 371)
MANAGEMENT
A. Hospitalization
All patients with ARF should be hospitalized for monitoring and initiation of treatment.
B. Eradication of GAS (Antibiotics)
Drug of choice: Penicillin
| Route | Regimen |
|---|---|
| Benzathine Penicillin G (IM, preferred) | 1.2 million units single dose IM (600,000 units for children ≤27 kg) |
| Phenoxymethyl penicillin (oral) | 500 mg twice daily (250 mg for children ≤27 kg) × 10 days |
| Amoxicillin (oral) | 50 mg/kg/day (max 1 g) × 10 days |
| Penicillin allergy: Azithromycin | 250 mg daily (oral macrolide) |
C. Treatment of Arthritis
- First-line: Aspirin (Salicylates) - 80-100 mg/kg/day in divided doses (max 4-8 g/day)
- Alternative: Naproxen - 10-20 mg/kg/day divided twice-daily
- Duration: 1-2 weeks after all symptoms resolve (not just joint symptoms)
- Dramatic NSAID response within 24-48 hours is itself diagnostically helpful
- Monitor renal function (check creatinine before starting NSAIDs)
D. Treatment of Carditis
- Mild/Moderate carditis: Bed rest, NSAIDs, close monitoring
- Severe carditis with heart failure:
- Treat with goal-directed heart failure therapy: diuretics, angiotensin receptor blockers (ACEi/ARBs)
- Fluid restriction
- Bed rest
- Corticosteroids (prednisolone): Some experts recommend in severe cases despite limited high-quality evidence
- Valve surgery: Rarely needed acutely; can be considered for acute valve leaflet rupture
- Echocardiography should be performed on all cases
E. Treatment of Chorea
- Usually does not require specific treatment - resolves spontaneously within weeks to months
- Supportive care: reduce stress, avoid stimulants
- For severe/disabling cases: Carbamazepine or valproic acid (preferred over haloperidol)
- Steroids occasionally used in severe chorea
F. Secondary Prophylaxis (Most Important Long-Term Measure)
Prevents recurrent GAS infections and subsequent ARF episodes that worsen cardiac damage.
| Patient Category | Duration |
|---|---|
| ARF without carditis | 5 years or until age 21 (whichever is longer) |
| ARF with carditis, no residual RHD | 10 years or until age 21 |
| ARF with carditis and residual RHD | At least 10 years or until age 40 (sometimes lifelong) |
| Severe RHD or post-valve surgery | Lifelong |
Drug of choice: Benzathine Penicillin G
- 1.2 million units IM every 4 weeks (3-weekly in high-risk patients)
- Alternative (less effective): Oral Penicillin V 250 mg twice daily
- Penicillin allergy: Erythromycin/Azithromycin
G. Bed Rest Protocol
| Severity | Activity Restriction |
|---|---|
| ARF without carditis | Bed rest until ESR/acute phase reactants normalize (~2 weeks) |
| ARF with mild carditis | Bed rest for 3-4 weeks |
| ARF with severe carditis | Strict bed rest for 2-3 months |
PROGNOSIS
- Arthritis, chorea, skin manifestations resolve completely with no permanent sequelae
- Carditis determines prognosis: 35-70% of patients with ARF develop chronic clinical RHD
- Resolution of carditis is most likely in the first year after acute episode
- Risk factors for RHD progression: severe initial carditis, recurrent ARF episodes, mitral valve involvement
- Secondary prophylaxis is the most effective intervention to prevent progression to severe RHD
SUMMARY TABLE
| Feature | Details |
|---|---|
| Causative organism | Group A Streptococcus (S. pyogenes) |
| Mechanism | Molecular mimicry - Type II + IV hypersensitivity |
| Latent period | 2-3 weeks after GAS pharyngitis |
| Age group | 5-14 years |
| Most common feature | Arthritis (75%) |
| Most important feature | Carditis (determines prognosis) |
| Pathognomonic lesion | Aschoff body (Anitschkow/caterpillar cells) |
| Diagnosis | Revised Jones Criteria (AHA 2015) |
| Most specific investigation | Echocardiography (subclinical carditis) |
| Antibiotic of choice | Benzathine Penicillin G |
| Secondary prophylaxis | Benzathine Penicillin G 1.2M units IM 4-weekly |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 371 - Acute Rheumatic Fever
- Goldman-Cecil Medicine International Edition, Chapter 269
- Robbins & Cotran Pathologic Basis of Disease, Chapter 12
Jones Criteria for RF
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from Harrison's 22E, Braunwald's Heart Disease, and Rosen's Emergency Medicine. Here is the complete, exam-ready answer:
JONES CRITERIA FOR THE DIAGNOSIS OF RHEUMATIC FEVER
Revised Jones Criteria - American Heart Association (AHA), 2015
HISTORY OF JONES CRITERIA
- Originally proposed by Dr. T. Duckett Jones in 1944 to aid in the diagnosis of ARF due to the absence of a definitive pathognomonic test
- Subsequently revised in 1956, 1965, 1984, 1992, and most recently 2015 (AHA)
- The 2015 revision introduced three major changes:
- Subclinical (echocardiographic) carditis accepted as a major criterion in all populations
- Risk stratification based on population ARF prevalence (low vs moderate/high risk)
- Expansion of arthritis criteria in moderate/high-risk populations
(Harrison's 22E, Chapter 371; Braunwald's Heart Disease, Chapter 81)
PREREQUISITE: EVIDENCE OF PRECEDING GROUP A STREPTOCOCCAL INFECTION
This is mandatory for diagnosis (except in pure Sydenham's chorea and indolent carditis):
| Test | Details |
|---|---|
| Positive throat culture | GAS on throat swab |
| Positive rapid streptococcal antigen test | Rapid GAS antigen detection |
| Elevated/rising ASO titer | Most commonly used; rises 3-6 weeks after pharyngeal infection; >200 Todd units |
| Elevated Anti-DNase B (ADB) | More sensitive for skin infections; stays elevated longer |
| Elevated anti-streptokinase, anti-hyaluronidase | Supplementary streptococcal antibody tests |
Note: Because most cases lack a positive throat culture by the time ARF presents, serologic evidence is usually required. Using both ASO + Anti-DNase B together provides >95% sensitivity. Age-specific local reference ranges should be used.
DIAGNOSTIC CRITERIA
PART A: Threshold for Diagnosis
| ARF Episode | Criteria Needed |
|---|---|
| Initial ARF | 2 Major OR 1 Major + 2 Minor manifestations |
| Recurrent ARF (in known RHD patient) | 2 Major OR 1 Major + 2 Minor OR 3 Minor manifestations |
PART B: MAJOR CRITERIA
| Major Criterion | Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|---|
| 1. Carditis | Clinical and/or subclinical (echocardiographic valvulitis) | Clinical and/or subclinical (echocardiographic valvulitis) |
| 2. Arthritis | Polyarthritis only | Monoarthritis OR polyarthritis; polyarthralgia also counts |
| 3. Chorea (Sydenham's) | Yes | Yes |
| 4. Erythema marginatum | Yes | Yes |
| 5. Subcutaneous nodules | Yes | Yes |
PART C: MINOR CRITERIA
| Minor Criterion | Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|---|
| Arthralgia | Polyarthralgia | Monoarthralgia |
| Fever | ≥38.5°C | ≥38.5°C |
| ESR | ≥60 mm/hr | ≥30 mm/hr |
| CRP | ≥3.0 mg/dL | ≥3.0 mg/dL |
| Prolonged PR interval | Yes (unless carditis = major criterion) | Yes (unless carditis = major criterion) |
POPULATION RISK DEFINITIONS
| Population Risk | Definition |
|---|---|
| Low risk | ARF incidence <2 per 100,000 school-aged children per year AND all-age RHD prevalence ≤1 per 1000 per year (e.g., USA, UK, Australia non-indigenous) |
| Moderate/High risk | ARF incidence ≥2 per 100,000 per year (e.g., India, sub-Saharan Africa, Pacific nations, Indigenous Australians) |
Rationale: In low-risk populations, criteria emphasize high specificity to avoid false-positive diagnosis. In high-risk populations, criteria emphasize high sensitivity to avoid missing cases.
DETAILED NOTES ON EACH MAJOR CRITERION
1. Carditis (Most Important - Determines Prognosis)
Pancarditis - all three layers may be involved:
| Layer | Manifestation |
|---|---|
| Endocarditis/Valvulitis | Mitral regurgitation (apical pansystolic murmur, most common); aortic regurgitation |
| Myocarditis | Tachycardia, cardiac enlargement, CCF, Aschoff bodies |
| Pericarditis | Pericardial friction rub, precordial pain |
Clinical carditis = new murmur, signs of heart failure, or pericardial rub
Subclinical (echocardiographic) carditis = valvulitis on echo without clinical signs - this is now a MAJOR criterion in 2015 revision (important exam point)
- Echocardiographic criteria include pathologic mitral or aortic regurgitation (meeting specific jet criteria)
- Isolated trivial regurgitation on echo is NOT sufficient - must meet defined echocardiographic criteria
-
50% of patients presenting with chorea will have subclinical carditis on echo
- Prolonged PR interval on ECG (1st-degree AV block) is common (35% of children with ARF)
2. Arthritis (Most Common Feature ~75%)
- Migratory polyarthritis of large joints (knees, ankles, elbows, wrists, hips) in low-risk populations
- In moderate/high-risk populations: monoarthritis and polyarthralgia also count as major
- Joints affected for hours to days, then "migrates" to next joint
- Exquisitely painful, out of proportion to signs
- Dramatic response to NSAIDs within 24-48 hours (so characteristic it is diagnostically useful)
- Synovial fluid: sterile with lymphocyte predominance
- Leaves no permanent joint damage
Important rule: Joint manifestations can only be counted in either the major OR the minor category in the same patient - never both. If arthritis is a major criterion, arthralgia cannot also be a minor criterion.
3. Sydenham's Chorea (~30%)
- Involuntary, non-rhythmic, purposeless movements
- Predominantly affects head (darting tongue movements) and upper limbs
- Can be generalized or unilateral (hemichorea)
- Associated with emotional lability, obsessive-compulsive traits
- Stops during sleep (distinguishing feature)
- May occur in isolation, months after GAS infection - in this case, Jones criteria may be fulfilled on chorea alone (streptococcal evidence may be absent)
- Usually resolves within 6 weeks; occasionally takes up to 6 months
4. Erythema Marginatum (<10%)

Erythema marginatum - the pen mark shows the location of the rash approximately 60 minutes earlier, demonstrating its evanescent nature. (Braunwald's Heart Disease, Fig. 81.5)
- Serpiginous, flat or slightly raised, non-pruritic, non-scarring rash
- Pink macules that clear centrally with spreading edges
- Evanescent - appears and disappears rapidly (within hours)
- Occurs on trunk and proximal limbs; almost never on the face
- Worsens with fever; may persist or recur despite treatment
- Follows an indolent course independent of ARF severity
5. Subcutaneous Nodules (<10%)

Subcutaneous nodule over the bony prominence of the elbow. (Braunwald's Heart Disease, Fig. 81.4)
- Small (0.5-2 cm), firm, painless, freely movable
- Located over bony prominences and extensor tendons (elbows, knees, wrists, occiput, vertebral spinous processes)
- Appear in crops; delayed manifestation (2-3 weeks after onset of disease)
- Last days to a few weeks (rarely >1 month)
- Strongly associated with severe carditis - their presence should prompt careful cardiac evaluation
- Less common in recent ARF episodes
SPECIAL SITUATIONS (Diagnosis Without Full Criteria)
Three clinical situations where ARF may be diagnosed without fulfilling full Jones criteria:
| Situation | Criteria |
|---|---|
| Pure Sydenham's chorea | Diagnosis of ARF can be made on chorea alone (streptococcal evidence may be absent due to long latency) |
| Indolent/low-grade carditis | Slowly progressive valvular disease presenting late |
| Recurrent ARF in established RHD | Lower threshold: 3 minor criteria alone may suffice |
IMPORTANT RULES AND CAVEATS (High-Yield for Exams)
- Joint manifestations - can only be counted in major OR minor category, not both in same patient
- Prolonged PR interval - cannot be a minor criterion if carditis is already a major criterion
- ASO titer may be normal in ARF following skin infection - Anti-DNase B is more sensitive in these cases
- Echocardiographic carditis alone (subclinical carditis) is now a major criterion - this is the key 2015 update
- Pure chorea is the only situation where ARF can be diagnosed without evidence of GAS infection
- Fever threshold is the same (≥38.5°C) in both low and high-risk populations (minor criterion)
- In moderate/high-risk populations, the ESR threshold is lower (≥30 vs ≥60 mm/hr), reflecting increased sensitivity
SUMMARY DIAGRAM
PREREQUISITE (MANDATORY):
Evidence of preceding GAS infection
(ASO titer / Anti-DNase B / throat culture)
↓
┌──────────────────────────────┐
│ MAJOR CRITERIA (5) │
│ C - Carditis │
│ A - Arthritis │
│ N - Nodules (subcutaneous) │
│ E - Erythema marginatum │
│ S - Sydenham's Chorea │
└──────────────────────────────┘
+
┌──────────────────────────────┐
│ MINOR CRITERIA (4) │
│ • Fever ≥38.5°C │
│ • ESR/CRP elevated │
│ • Prolonged PR interval │
│ • Arthralgia │
└──────────────────────────────┘
↓
INITIAL ARF = 2 Major OR 1 Major + 2 Minor
RECURRENT ARF = 2 Major OR 1M+2m OR 3 Minor
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 371 - Table 371-2
- Braunwald's Heart Disease, Chapter 81 - Table 81.2
- Goldman-Cecil Medicine, Table 269-3
- Gewitz MH et al. Revision of the Jones Criteria for diagnosis of ARF. AHA Scientific Statement. Circulation 2015;131:1806-1818
This is a shared conversation. Sign in to Orris to start your own chat.