Babinskis sign
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Here is a thorough breakdown of Babinski's sign from authoritative neurology textbooks.
Babinski's Sign
Definition
Babinski's sign is the abnormal plantar (extensor) response elicited by stroking the lateral sole of the foot. It was first described by the French neurologist Joseph Babinski in 1896 (great toe sign) and expanded in 1903 (fan/toe abduction sign).
Normal response: downward (plantar) flexion of all toes.
Babinski's sign (positive/abnormal): dorsiflexion (extension, upgoing) of the great toe, often with fanning (abduction) of the other four toes. Together these are sometimes called the "extensor plantar response."
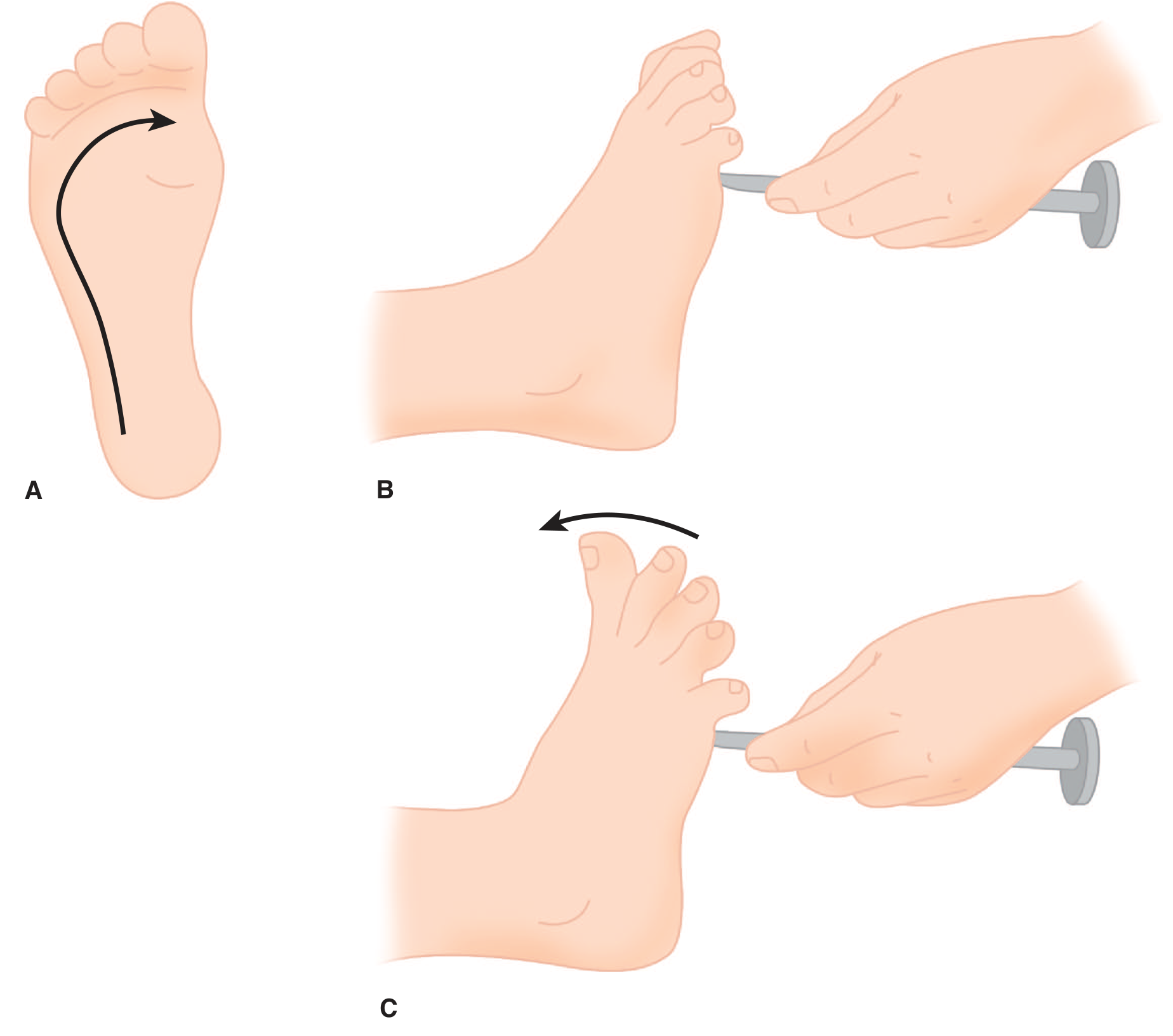
Figure: A. The plantar response is elicited by stroking from the heel to the ball of the foot. B. Normal plantar response - toes flex downward. C. Extensor plantar response (Babinski's sign) - great toe extends upward with fanning of remaining digits. - Adams and Victor's Principles of Neurology, 12th Ed.
How to Elicit It
- Use a blunt object (e.g., a key, tongue blade handle, or reflex hammer tip)
- Stroke firmly from the lateral heel upward toward the ball of the foot, then arc medially toward the big toe
- The stimulus must be firm but does not need to be painful
- Alternative sites: squeeze the calf (Schafer), stroke the shin downward (Oppenheim), squeeze the Achilles tendon, flick the 4th toe - all have the same significance
- If the patient withdraws due to ticklishness, ask them to perform the test themselves
Significance
Babinski's sign is one of the most reliable indicators of an upper motor neuron (UMN) lesion - specifically, damage anywhere along the corticospinal (pyramidal) tract.
| Condition | Significance |
|---|---|
| Adults | Always abnormal - indicates corticospinal tract damage |
| Infants (<~18 months) | Normal - descending tracts are not yet myelinated |
| Bilateral | Suggests bilateral corticospinal lesion (e.g., spinal cord lesion, bilateral hemispheric disease) |
"The sign is a dependable marker of damage to the corticospinal system." - Adams and Victor's Principles of Neurology, 12th Ed., p. 20
Pathophysiology
Babinski's sign is a release phenomenon - a fragment of the primitive spinal flexor (nocifensive/protective) reflex that is normally suppressed by descending corticospinal inhibition.
- The great toe extension, paradoxically, is a dorsiflexion component of the "triple flexion response" (hip, knee, and ankle all flex in response to a noxious stimulus)
- In an intact corticospinal system, this response is suppressed and only plantar flexion occurs
- When the corticospinal tract is damaged, the spinal reflex is disinhibited (released)
- Electrophysiologically, this reflex is mediated by Aδ (pain) afferents converging on spinal interneurons
Clinical Context - UMN vs. LMN
Babinski's sign clusters with the full UMN syndrome:
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes | Hyperreflexia, clonus | Hyporeflexia or areflexia |
| Plantar response | Extensor (Babinski +ve) | Flexor (normal) or absent |
| Wasting | Absent or mild disuse atrophy | Prominent, early |
| Fasciculations | Absent | Present |
| Distribution | Antigravity muscles (arm flexors, leg extensors) | Affected muscles only |
Important Pitfalls
- "Silent" toes - if toes neither go up nor down, and the contralateral side clearly goes down, the silent side is considered abnormal
- Withdrawal response - brisk withdrawal (ticklishness) can mimic or obscure the sign; use alternative stimuli or ask the patient to test themselves
- Severe toe extensor weakness - may prevent the sign even with a genuine UMN lesion
- Bilateral cerebral lesions can also produce the jaw jerk and other cranial hyperreflexia (pseudobulbar palsy)
Named Equivalents (Same Significance as Babinski)
Dozens of eponymous variants exist using alternative stimulation sites but all indicate the same corticospinal pathology:
| Sign | Stimulus |
|---|---|
| Chaddock | Stroke lateral malleolus/dorsolateral foot |
| Oppenheim | Firm downward scraping of the shin |
| Gordon | Squeezing the calf |
| Schafer | Squeezing the Achilles tendon |
| Bing | Pricking the dorsum of foot |
| Gonda/Allen | Flick/snap the 4th toe downward |
Conditions Where Babinski's Sign Is Found
- Stroke (most common)
- Spinal cord compression / trauma
- Multiple sclerosis
- Motor neuron disease (ALS) - upper motor neuron component
- Brain tumors
- Cerebral palsy
- Hepatic encephalopathy (metabolic)
- Post-ictal state (Todd's paralysis)
- Deep sleep or general anesthesia (transient)
- Normal infants up to ~18 months of age
Sources: Adams and Victor's Principles of Neurology, 12th Ed., pp. 20, 73-74; Neuroanatomy through Clinical Cases, 3rd Ed., p. 1929-1932; Neuroscience: Exploring the Brain, 5th Ed., p. 1327
This is a shared conversation. Sign in to Orris to start your own chat.