Reading File
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
I now have all the information needed to provide a comprehensive answer. Let me compile the full response.
Answers to the Clinical Case
Clinical Clues Summary
The patient is an elderly male, chronic smoker and alcoholic, recently diagnosed diabetic, presenting with:
- High-grade fever, productive cough, chest pain, dyspnea x 3 days
- Dull percussion note on right upper chest
- Chest X-ray: consolidation over right upper lobe
- Sputum sent for microbiology
1. Identify the Pathogen
Klebsiella pneumoniae (also historically called "Friedlander's bacillus")
This is the classic presentation. The combination of:
- Right upper lobe consolidation on CXR - this is the hallmark radiographic feature of K. pneumoniae pneumonia
- Alcoholism - the single strongest risk factor for community-acquired K. pneumoniae pneumonia
- Diabetes mellitus - a major additional risk factor
- Chronic smoker (associated COPD/mucociliary damage)
- Elderly patient (reduced host immunity)
Gram stain of sputum would show large, encapsulated, gram-negative rods arranged singly or in pairs. Culture on MacConkey agar would show large, mucoid, pink (lactose-fermenting) colonies. The organism may produce a "string test" positive result due to its hypermucoviscous capsule.
"The classic cause of community-acquired gram-negative bacillary pneumonia, K. pneumoniae (Friedlander pneumonia), causes 3-5% of CAP overall... Excessive alcohol use, diabetes, and COPD are the major risk factors for community-acquired K. pneumoniae infection." - Murray & Nadel's Textbook of Respiratory Medicine
2. Pathogenicity of Klebsiella pneumoniae
A. The Polysaccharide Capsule (Primary Virulence Factor)
- The capsule is the most important virulence factor
- It inhibits opsonization and phagocytosis - prevents neutrophils and macrophages from engulfing the organism
- It shields pathogen-associated molecular patterns (PAMPs) required to activate Toll-like receptors (TLRs), blunting innate immune recognition
- K1 and K2 capsular types are the most common causes of serious infection
- Hypervirulent strains have increased capsule content due to altered capsule biosynthesis regulators
B. Lipopolysaccharide (LPS / Endotoxin)
- An important virulence factor
- Triggers systemic inflammatory response (fever, sepsis)
- Lipid A component causes endotoxemia and septic shock
C. Siderophores (Iron Acquisition)
- K. pneumoniae expresses multiple siderophores that sequester iron from the host
- Iron is essential for bacterial survival and multiplication
- Yersiniabactin is expressed specifically in the lung and evades the host's lipocalin-2 neutrophil defense mechanism
D. Fimbriae and Adhesins
- Allow adherence to respiratory epithelial cells
- Type 1 and type 3 fimbriae facilitate biofilm formation
E. Result of These Virulence Factors Together
- Massive lobar consolidation with alveolar exudate (the hallmark "brick-red currant jelly sputum" due to blood-stained mucoid sputum - though now rarely seen)
- Tissue destruction with potential cavitation and lung abscess formation
- High mortality (25-75%) if untreated, especially with bacteremia
"A major virulence factor for K. pneumoniae infection is the capsule... The capsule inhibits opsonization and phagocytosis and can shield pathogen-associated molecular patterns required to activate TLRs." - Murray & Nadel's Textbook of Respiratory Medicine
3. Interpret the Susceptibility Report
The table below shows two sets of antibiotics - likely representing two different organisms or two disks for the same organism. Looking at the pattern, rows 1-5 appear to be one organism panel and rows 6-8 another (note the different disk strengths for tetracycline/chloramphenicol/vancomycin). The interpretations are:
| Antimicrobial Agent | Disk (µg) | Resistant (mm) | Intermediate (mm) | Sensitive (mm) | Observed Zone (mm) | Interpretation |
|---|---|---|---|---|---|---|
| Erythromycin | 30 | ≤19 | 20-22 | ≥23 | 16 | RESISTANT |
| Levofloxacin | 30 | ≤18 | 19-24 | ≥25 | 25 | SENSITIVE |
| Tetracycline | 10 | ≤19 | 20-22 | ≥23 | 26 | SENSITIVE |
| Chloramphenicol | 10 | ≤12 | 13-14 | ≥15 | 16 | SENSITIVE |
| Vancomycin | 5 | ≤16 | 17-20 | ≥21 | 20 | INTERMEDIATE |
| Tetracycline | 10 | ≤13 | 14-16 | ≥17 | 13 | RESISTANT |
| Chloramphenicol | 20/10 | ≤13 | 14-17 | ≥18 | 21 | SENSITIVE |
| Vancomycin | 100/10 | ≤17 | 18-20 | ≥21 | 25 | SENSITIVE |
Key interpretive notes:
- Erythromycin - RESISTANT: Zone = 16 mm, which is ≤19 mm (resistant cutoff). This drug should NOT be used.
- Levofloxacin - SENSITIVE: Zone = 25 mm, which meets the ≥25 mm sensitive threshold exactly. This is a clinically useful drug for this patient.
- Tetracycline (1st row) - SENSITIVE: Zone = 26 mm, well above the ≥23 mm threshold.
- Chloramphenicol (1st row) - SENSITIVE: Zone = 16 mm, which is ≥15 mm - just over the sensitive threshold.
- Vancomycin (5µg) - INTERMEDIATE: Zone = 20 mm, which falls in the 17-20 mm intermediate range. Intermediate means the drug may work at higher doses or in sites of concentration, but should not be relied upon as first-line.
- Tetracycline (2nd row, likely different disk/organism) - RESISTANT: Zone = 13 mm, which is ≤13 mm (resistant).
- Chloramphenicol (20/10 disk) - SENSITIVE: Zone = 21 mm, which is ≥18 mm.
- Vancomycin (100/10 disk, likely co-trimoxazole or combination) - SENSITIVE: Zone = 25 mm, which is ≥21 mm.
Note on Vancomycin: Vancomycin is a glycopeptide active against gram-positive organisms only. Its presence on a K. pneumoniae (gram-negative) sensitivity panel is unusual - this may reflect a mixed infection or an error in the panel. K. pneumoniae is intrinsically resistant to vancomycin due to its outer membrane. The last two rows (with different disk strengths for tetracycline, chloramphenicol, and what appears labeled as vancomycin) may represent a second organism co-isolated (possibly Staphylococcus aureus given upper lobe disease in a smoker/diabetic), or the "vancomycin" label may be a mislabel for co-trimoxazole (SXT, commonly tested as 1.25/23.75 µg disk).
4. Treatment
Based on the susceptibility results, the organism is sensitive to levofloxacin:
Drug of Choice: Levofloxacin 750 mg IV/PO once daily
This is a respiratory fluoroquinolone with excellent:
- Gram-negative coverage including K. pneumoniae
- Lung penetration and tissue concentration
- Bioavailability (near 100% oral)
Additional considerations for this specific patient:
| Factor | Implication |
|---|---|
| Elderly + severe CAP | May require IV therapy initially; consider ICU if hypoxic |
| Diabetic | Monitor blood glucose closely (fluoroquinolones can affect glycemia) |
| Alcoholic | Risk of malnutrition, liver disease - check LFTs; thiamine supplementation |
| Smoker | Increased airway damage, slower clearance |
Supportive treatment:
- Oxygen supplementation (maintain SpO2 >94%)
- IV fluids for hydration
- Antipyretics (paracetamol)
- If severe sepsis: blood cultures x2, early antibiotics within 1 hour
- Nutritional support
Duration: 5-7 days for CAP with levofloxacin (or until afebrile x 48-72 hours)
If there is concern for hypervirulent K. pneumoniae (given diabetes + alcoholism + upper lobe disease), a combination regimen with a beta-lactam (e.g., ceftriaxone or piperacillin-tazobactam) plus levofloxacin may be preferred until full susceptibility results are confirmed. Erythromycin should be avoided (RESISTANT). Tetracycline, while sensitive, is not a first-line drug for serious pneumonia.
"In patients with serious infection, a two-drug regimen of a β-lactam/β-lactamase inhibitor or carbapenem with an aminoglycoside or a fluoroquinolone is recommended for treatment until susceptibility results are known." - Murray & Nadel's Textbook of Respiratory Medicine, p. 1007
analyse_media
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I have all the material needed. Here is the comprehensive answer:
Answers to the Clinical Case
Clinical Summary
An elderly COPD patient on mechanical ventilation develops new fever, purulent tracheal secretions, dropped SpO2, leukocytosis (14,000 WBC, neutrophil-predominant), and fresh bilateral consolidation patches on day 5 of intubation. BAL fluid sent for culture.
Microbiology clues:
- Gram-negative coccobacilli
- Non-motile
- Oxidase negative
- Does not ferment sugars (non-fermenter)
- Resistant to all antibiotics except carbapenems and colistin
1. Identify the Organism
Acinetobacter baumannii
This is the classic organism fitting every clue provided:
| Characteristic | A. baumannii |
|---|---|
| Morphology | Gram-negative coccobacilli (short rods, nearly spherical in stationary phase) |
| Motility | Non-motile (no flagella) |
| Oxidase test | Negative (distinguishes it from Pseudomonas, which is oxidase-positive) |
| Sugar fermentation | Non-fermenter (uses oxidative metabolism only) |
| Resistance pattern | MDR - typically resistant to most antibiotics; carbapenems are last resort; colistin/polymyxins used for pandrug-resistant strains |
| Setting | Classic cause of ICU/ventilator-associated pneumonia (VAP), especially late-onset (>5 days) |
A. baumannii is an environmental organism that thrives on hospital surfaces and medical equipment. It has an extraordinary capacity to acquire resistance determinants. The late-onset VAP on day 5 of intubation fits perfectly - peak VAP incidence is between days 5-9 post-intubation.
"Acinetobacter spp are a cause of pneumonia in patients who have risk factors for antimicrobial resistant organisms, often manifested as ventilator-associated pneumonia." - Goldman-Cecil Medicine
2. What is Ventilator-Associated Pneumonia (VAP)?
VAP is defined as the development of pneumonia 48 hours or more after endotracheal intubation.
Key features:
- Incidence: Occurs in up to 40% of intubated patients; it is the most frequent ICU-acquired infection and the most frequent ventilator-associated complication
- Timing: Peak incidence is 5-9 days after intubation (matching this case exactly); cumulative risk is proportional to duration of intubation
- Pathogenesis: The endotracheal tube (ETT) bypasses normal upper airway defenses (mucociliary clearance, cough reflex, IgA). Bacteria colonize the oropharynx and sub-glottic secretions accumulate above the ETT cuff, which then aspirate into the lower airways. Biofilm formation on the ETT inner surface provides a reservoir for repeated inoculation.
Diagnostic criteria:
- New or worsening infiltrate on CXR in a ventilated patient (>48h post-intubation)
- PLUS at least 2 of:
- Fever (>38°C) or hypothermia (<36°C)
- Leukocytosis (>12,000) or leukopenia (<4,000)
- Purulent tracheal secretions
Microbial diagnosis:
- Non-invasive: Endotracheal aspirate (ETA) cultures + blood cultures (positive ~15% of cases)
- Invasive: Bronchoscopy with BAL (as done in this case) and protected specimen brush (PSB)
"VAP is defined as the development of pneumonia 48 or more hours after endotracheal intubation... VAP occurs in up to 40% of intubated patients; it is the most frequent ventilator-associated complication and most frequent ICU-acquired infection." - Frameworks for Internal Medicine
3. Treatment of This Patient
The isolate is resistant to all antibiotics except carbapenems and colistin - this is a carbapenem-susceptible but otherwise MDR A. baumannii strain.
First-line treatment: Carbapenem
Since the organism is susceptible to carbapenems, the preferred approach is:
Meropenem 2 g IV q8h (infused over 3 hours - extended infusion maximizes pharmacodynamic efficacy via time-dependent killing)
OR
Imipenem-cilastatin 500 mg IV q6h (extended infusion over 3 hours)
Role of Colistin (Polymyxin E):
- Since the isolate is also sensitive to colistin, inhaled colistin can be added as adjunct therapy for lung infections to achieve high local concentrations in the airways that IV colistin cannot achieve
- Colistin is preferred over polymyxin B for respiratory infections due to better lung penetration via inhalation
- Nephrotoxicity and neurotoxicity must be monitored
Combination therapy (for severe/ICU VAP):
A two-drug regimen is recommended in severe infection:
- Carbapenem + inhaled colistin (augmented therapy)
- If available: Sulbactam-durlobactam (approved 2023 for VAP caused by A. baumannii-calcoaceticus complex; 28-day mortality 19% vs. 32% with colistin alone)
Supportive management:
- Optimize mechanical ventilation (lung-protective: Vt 6 mL/kg ideal body weight, plateau pressure <30 cm H2O)
- Daily spontaneous awakening trials (SATs) and spontaneous breathing trials (SBTs) to reduce ventilator days
- Treat underlying COPD exacerbation
- Strict infection control to prevent outbreak spread
"In susceptible strains, a carbapenem or ampicillin-sulbactam is considered first-line therapy. Some strains may only be susceptible to polymyxins (eg, polymyxin B, colistin). In such cases, inhaled colistin may be added to augment therapy." - Frameworks for Internal Medicine "Meropenem 2g q8h - carbapenem-susceptible isolates only; infuse over 3h" - Harrison's Principles of Internal Medicine, 22e (Table 167-1)
4. What is a VAP Bundle? Why is it Used?
Definition:
A VAP bundle is a set of evidence-based practices grouped together and applied consistently to every mechanically ventilated patient to prevent VAP. The concept is that implementing all components together achieves greater benefit than any single intervention alone.
Why it is used:
VAP causes significant morbidity, mortality, prolonged ICU stays, and increased healthcare costs. Bundle implementation standardizes care, reduces variation, and improves patient safety - even when individual studies on single components show mixed results.
Components of the VAP Bundle:
| Component | Rationale |
|---|---|
| 1. Head-of-bed elevation (30-45°) | Semi-recumbent positioning prevents aspiration of gastric contents and sub-glottic secretions |
| 2. Spontaneous Awakening Trials (SATs) + Spontaneous Breathing Trials (SBTs) | Daily sedation holidays + SBTs reduce total ventilator days, which is the primary VAP risk driver |
| 3. Subglottic secretion suctioning | Drains pooled secretions above the ETT cuff before they aspirate; 3 large meta-analyses showed VAP rate reduction |
| 4. Oral hygiene with chlorhexidine | Reduces oropharyngeal bacterial colonization and subsequent aspiration |
| 5. Avoid unnecessary ventilator circuit changes | Frequent circuit changes increase VAP risk by introducing contaminated secretions |
| 6. GI prophylaxis (H2-blocker or PPI) | Prevents stress ulcers; reduces gastric bacterial overgrowth |
| 7. VTE prophylaxis | Prevents deep vein thrombosis in immobile ICU patients |
| 8. Consider early tracheostomy (if prolonged ventilation anticipated) | Lower VAP rate than ETT; shortens mechanical ventilation duration |
"Bundles of care... are evidence-based practices that are grouped together to encourage the consistent delivery of these practices... they allow for standardized care as well as decreasing variation, thereby improving healthcare quality and safety." - Current Surgical Therapy 14e
"In an effort to reduce a new bacterial infection while mechanically ventilated, the components of the VAP bundle aim to reduce bacterial colonization and prevent aspiration of contaminated secretions." - Miller's Anesthesia, 10e
Note on "YAP-bundle" in the question:
This is a typographical error in the question sheet. The correct term is VAP bundle (Ventilator-Associated Pneumonia bundle), as confirmed by the clinical context.
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed. Here is the comprehensive answer:
Answers to the HIV / Oral Thrush Clinical Case
Clinical Context
An HIV-positive male taking HAART irregularly presents with oral thrush - a classic opportunistic infection signaling immune compromise due to poor antiretroviral adherence.
1. Identify the Agent + Labelled Diagrams
The infecting agent is Candida albicans - the most common cause of oral candidiasis (thrush).
Microscopic Morphology of Candida albicans
C. albicans is a dimorphic fungus that can exist as:
- Yeast phase: small (5-7 µm), oval, thin-walled budding cells (blastoconidia)
- Hyphal/pseudohyphal phase: when invasive (seen in tissue infection)
Here is the actual microscopic image from the medical textbook (cornmeal agar preparation) showing the classic morphology:
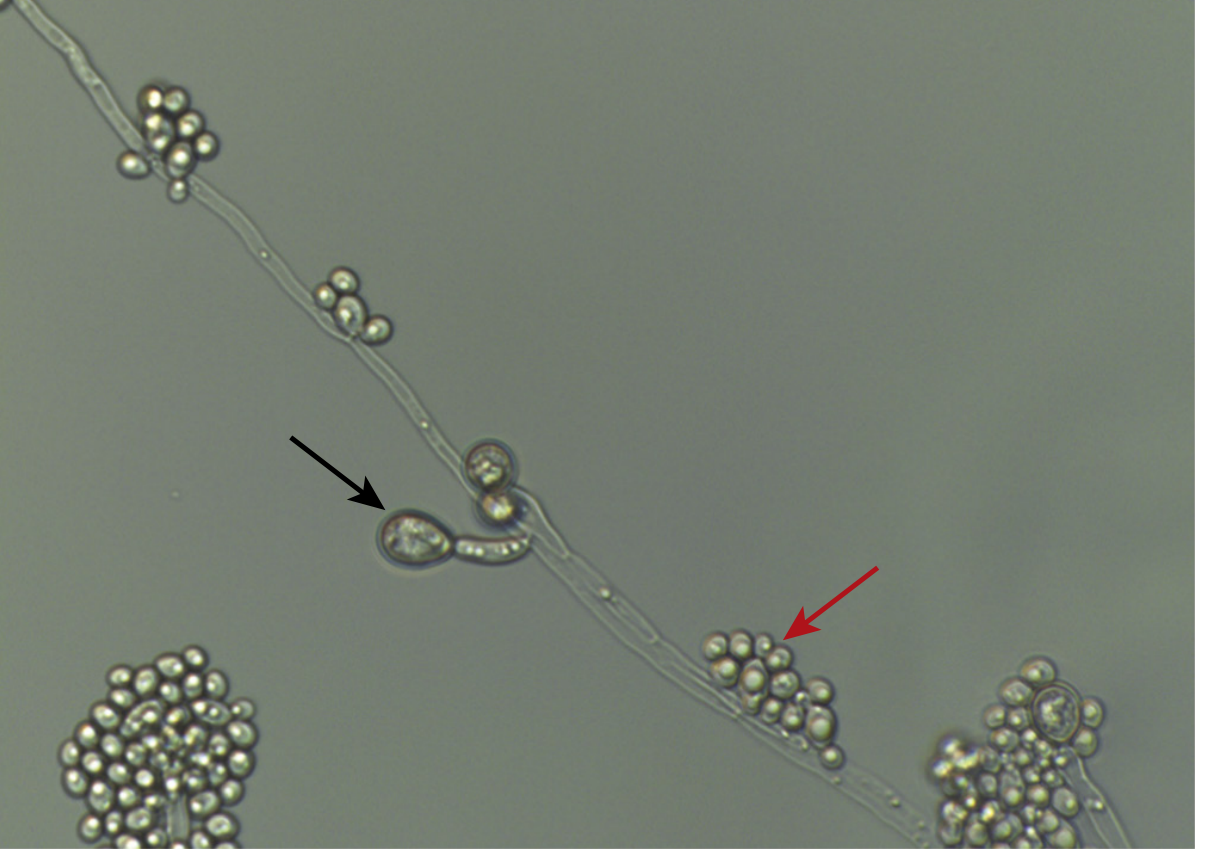
Fig. 65.2 - Candida albicans on cornmeal agar: large chlamydospores (black arrow), blastoconidia/buds (red arrow), pseudohyphae (elongated chains), and true hyphae. (Medical Microbiology 9e)
Labelled Diagram Description (for your exam drawing):
CANDIDA ALBICANS - Microscopic Morphology
Yeast Phase (on mucosa):
___
/ \ <- Blastoconidia (budding yeast, 5-7µm)
| O |
\___/
| <- Bud (blastoconidium)
_|_
/ \
| O | <- Parent cell
Pseudohyphae (in tissue invasion):
O—O—O—O—O <- elongated, pinched at septa, NOT true hyphae
(constrictions at junctions = hallmark of pseudohyphae)
True hyphae (parallel walls, no constriction)
═══════════
Chlamydospores (diagnostic for C. albicans):
___
--( O )-- <- Large, thick-walled terminal/intercalary spore
--- <- produced on cornmeal agar
Key Diagnostic Tests:
- Germ tube test (Reynolds-Braude phenomenon): C. albicans produces germ tubes within 2-3 hours when incubated in serum at 37°C - a confirmatory and rapid test
- Cornmeal agar: produces chlamydospores (thick-walled terminal spores) - unique to C. albicans
- KOH mount of oral scraping: shows budding yeasts + pseudohyphae
- Culture on Sabouraud's dextrose agar: white/cream-coloured, pasty colonies
"Morphology ranges from budding yeasts to pseudohyphae and true hyphae. Reproduction is by formation of blastoconidia (buds)." - Medical Microbiology 9e
"Diagnosis of oral thrush is generally clinical with white mucosal plaques that are removed with gentle scraping... Biopsy of affected oral tissue shows yeasts, pseudohyphae, and hyphae invading into the epithelium." - Harrison's Principles of Internal Medicine 22e
2. Risk Factors for Acquiring This Infection + CD4+ T Cell Levels
Risk Factors for Candida Infection in HIV Patients:
| Risk Factor | Mechanism |
|---|---|
| HIV infection with low CD4 count | Loss of T-cell-mediated immunity; CD4+ cells are critical for anti-Candida defense |
| Irregular/non-adherent HAART (this patient) | Allows ongoing viral replication → progressive CD4 depletion |
| Broad-spectrum antibiotics | Disrupt normal bacterial flora that competes with Candida |
| Corticosteroid use | Suppresses local and systemic immunity |
| Diabetes mellitus | Elevated glucose feeds yeast; impaired neutrophil function |
| Dentures | Create a warm, moist environment for Candida colonization |
| Xerostomia (dry mouth) | Saliva has antifungal properties (IgA, lactoferrin) |
| Smoking | Alters oral mucosal integrity and microbiome |
| Chemotherapy/malignancy | Neutropenia |
"Oral carriage rates are increased substantially in hospitalized patients; those with HIV infection, dentures, and diabetes; patients receiving antineoplastic chemotherapy; those receiving antibiotics." - Medical Microbiology 9e
CD4+ T Cell Levels in This Patient:
Oral thrush (oropharyngeal candidiasis) typically occurs when CD4+ count falls below 200 cells/µL.
More specifically:
| CD4+ Count | Expected Opportunistic Infection |
|---|---|
| <500 cells/µL | Oral thrush, recurrent herpes zoster, TB reactivation |
| <200 cells/µL | Oral/esophageal candidiasis, PCP (Pneumocystis pneumonia) ← this patient |
| <100 cells/µL | Cryptococcal meningitis, Toxoplasma encephalitis |
| <50 cells/µL | CMV retinitis, disseminated MAC |
Since this patient has oral thrush, his CD4+ count is likely below 200 cells/µL (normal is ~800-1200 cells/µL).
"Opportunistic infections usually do not occur in HIV-infected patients until CD4 T-cell counts have dropped from the normal level of about 1000 cells/µL to less than 200 cells/µL." - Jawetz, Melnick & Adelberg's Medical Microbiology 28e
3. Other Opportunistic Infections in This Patient
With CD4+ <200 cells/µL (due to irregular HAART), this patient is at risk for:
Fungi:
- Pneumocystis jirovecii pneumonia (PCP) - the most common OI; presents with dry cough, progressive dyspnea, bilateral interstitial infiltrates on CXR
- Cryptococcus neoformans - meningitis (CD4 <100); "soap bubble" lesions on brain MRI; India ink stain shows encapsulated yeast
- Histoplasma capsulatum - disseminated histoplasmosis in endemic areas
- Coccidioides immitis - disseminated coccidioidomycosis
Bacteria:
- Mycobacterium tuberculosis (TB) - reactivation TB even at higher CD4 counts
- Mycobacterium avium-intracellulare (MAC) - disseminated at CD4 <50 (fever, wasting, night sweats)
- Nocardia asteroides - pulmonary/CNS lesions
- Salmonella - recurrent bacteremia
Viruses:
- CMV (Cytomegalovirus) - retinitis (leading to blindness at CD4 <50), esophagitis, colitis
- HSV (Herpes simplex) - persistent, progressive mucocutaneous ulcers
- VZV (Varicella-zoster) - disseminated zoster
- JC polyomavirus - Progressive Multifocal Leukoencephalopathy (PML)
- EBV - oral hairy leukoplakia, B-cell lymphoma
Protozoa:
- Toxoplasma gondii - CNS toxoplasmosis (ring-enhancing lesions on CT)
- Cryptosporidium - chronic, voluminous watery diarrhea
- Isospora belli - chronic diarrhea and malabsorption
Malignancies (AIDS-defining):
- Kaposi's sarcoma (HHV-8) - skin/mucosal purple lesions
- Non-Hodgkin lymphoma (EBV-associated)
- Cervical cancer (HPV-associated, AIDS-defining in women)
"The most common opportunistic infections in untreated AIDS patients include: Protozoa (Toxoplasma, Cryptosporidium), Fungi (Candida, Cryptococcus, Histoplasma, Pneumocystis jiroveci), Bacteria (MAC, M. tuberculosis), Viruses (CMV, HSV, VZV, JC polyomavirus)." - Jawetz, Melnick & Adelberg's Medical Microbiology 28e
4. Treatment
Treatment has two parallel arms: treat the oral thrush AND address the underlying cause (irregular HAART).
A. Treatment of Oral Thrush (Candida albicans)
Mild disease:
- Nystatin oral suspension (100,000 units/mL): 4-6 mL swish-and-swallow 4x/day for 7-14 days
- Clotrimazole troches (10 mg): dissolve 5x/day for 14 days - a palatable alternative to nystatin
Moderate to severe disease (or if topical therapy fails):
- Fluconazole 100-200 mg orally once daily for 7-14 days - drug of choice for systemic azole therapy
- Note: fluconazole resistance is increasing, especially in patients with prior azole exposure
If esophageal involvement (dysphagia/odynophagia):
- Systemic fluconazole 200-400 mg/day for 14-21 days
- Alternative: itraconazole, voriconazole, or an echinocandin (caspofungin, micafungin) for refractory disease
"Mild oral thrush may be treated with topical agents such as nystatin suspension or clotrimazole troches, but moderate and severe disease or esophageal involvement should be treated with systemic, primarily azole therapy." - Harrison's Principles of Internal Medicine 22e
B. Address HIV - Optimize HAART
The underlying problem is irregular HAART use allowing CD4+ depletion:
- Assess adherence barriers (side effects, pill burden, cost, mental health, substance use)
- Reinforce/restart antiretroviral therapy with an effective regimen (current guidelines favor integrase strand transfer inhibitor-based regimens: e.g., bictegravir/tenofovir alafenamide/emtricitabine - single-tablet once daily)
- Goal: Achieve viral suppression (HIV RNA undetectable) and CD4+ count recovery above 200 cells/µL, which will reduce recurrent OIs
- Consider OI prophylaxis if CD4+ remains <200: TMP-SMX (cotrimoxazole) for PCP prophylaxis
C. General Supportive Measures:
- Oral hygiene reinforcement
- Screen for and treat other OIs (check for PCP, TB, CMV)
- Nutritional support (oral thrush causes dysphagia and malnutrition)
- Follow-up CD4 count and HIV viral load in 4-8 weeks after HAART optimization
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Here is the comprehensive answer:
Answer: Mucormycosis (Rhinocerebral) in a Diabetic with DKA
Clinical Clue Analysis
| Finding | Significance |
|---|---|
| Uncontrolled diabetic + ketoacidosis (DKA) | Classic predisposing condition for mucormycosis |
| Facial swelling on left side | Rhinocerebral/rhino-orbital spread |
| Thin serosanguineous discharge | Tissue necrosis with vascular invasion - hallmark of Mucorales |
| KOH wet mount: ribbon-like, broad, aseptate hyphae | Pathognomonic for Mucorales (order) |
| SDA at 37°C, 3-4 days: grey-white, thick, cottony fluffy growth | Rapid-growing Mucorales colony on culture |
1. Identify the Pathogen
The infecting agent is Rhizopus oryzae (most common) belonging to the Order Mucorales - causing Mucormycosis (Rhinocerebral/Rhino-orbital form)
Other Mucorales genera that can cause the same disease: Mucor, Lichtheimia (Absidia), Cunninghamella, Rhizomucor
"Rhizopus oryzae and R. delemar are by far the most common causes of mucormycosis in the Western Hemisphere." - Harrison's Principles of Internal Medicine 22e
2. Labelled Diagrams
A. Microscopic Morphology (KOH Wet Mount / Tissue Section)
MUCORALES - Microscopic Features (KOH Mount / Tissue)
←←← BROAD, RIBBON-LIKE HYPHAE (6-30 µm wide) ←←←
═══════════════════════════════════════════ <- True hyphae
(NO septa = ASEPTATE)
↑ ↑
Right-angle Right-angle
branching (90°) branching (90°)
Compare: Aspergillus = narrow, SEPTATE, acute-angle (45°) branching
The histopathology image below shows the broad, ribbon-like, nonseptate Rhizopus hyphae invading brain parenchyma (arrows) with a thrombosed blood vessel (arrowhead) - classic angioinvasion:
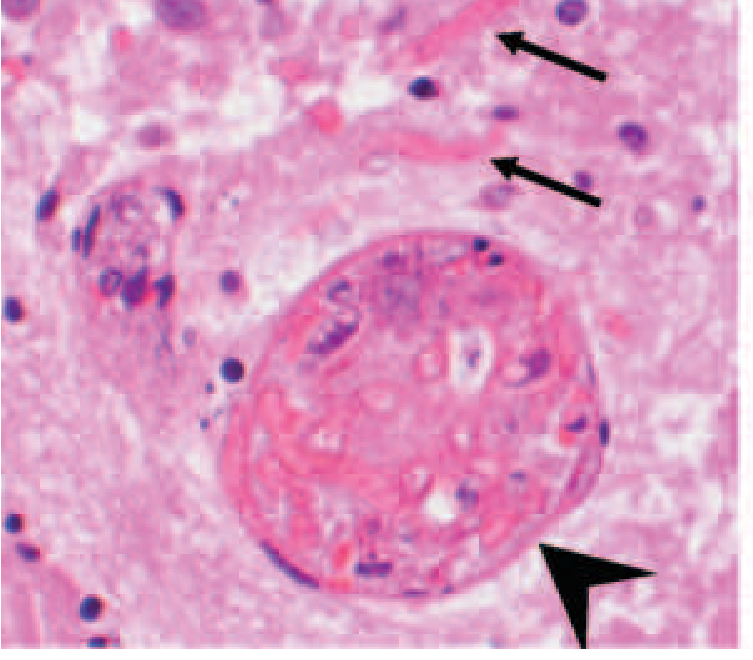
Fig. 224-1A: Histopathology of Rhizopus delemar in infected brain - broad, ribbon-like, nonseptate hyphae in parenchyma (arrows) and thrombosed vessel with intravascular hyphae (arrowhead), H&E. (Harrison's 22e)
B. Colony Morphology on SDA (Sabouraud's Dextrose Agar)
MUCORALES COLONY - SDA at 37°C
Day 1-2: Rapid white growth spreads across the plate
Day 3-4: Grey-white, thick, cottony-fluffy mycelium
(fills the entire tube/plate rapidly = "lid-lifter" growth)
Macroscopic: No pigment initially → grey-brown with age
C. Rhizopus Reproductive Structures (for exam diagram)
RHIZOPUS spp. - Key Features to Draw
COLUMELLA (dome-shaped)
___
/ \
| Spo | <- SPORANGIUM (round, filled with sporangiospores)
|rng. |
\___/
|
| <- SPORANGIOPHORE (unbranched stalk)
|
======|====== <- STOLON (horizontal runner)
| |
[///] [///] <- RHIZOIDS (root-like structures at base)
*** PRESENT in Rhizopus (absent in Mucor)
Key distinguishing features of Rhizopus vs Mucor:
- Rhizopus: RHIZOIDS present at base of sporangiophore ✓
- Mucor: NO rhizoids ✗
"The sporangium of this mold has released its sporangiospores but remains attached to the supporting sporangiophore, and rhizoids are apparent at the base of the sporangiophore." - Jawetz, Melnick & Adelberg's Medical Microbiology
3. Clinical Diagnosis
Rhinocerebral (Rhino-Orbital-Cerebral) Mucormycosis in a Diabetic with DKA
Why this patient is uniquely susceptible:
Mechanism 1 - Metabolic Acidosis (DKA):
The acidosis causes dissociation of iron from sequestering proteins (transferrin, ceruloplasmin) → free iron in serum → Mucorales use iron directly for enhanced survival and virulence. The ketone body β-hydroxybutyrate also upregulates host cell receptors (GRP78) that the fungus binds to, enabling tissue penetration.
Mechanism 2 - Hyperglycemia:
Even without acidosis, hyperglycemia contributes via four mechanisms:
- Glycosylation of iron-sequestering proteins, disrupting normal iron sequestration
- Upregulation of GRP78 (mammalian receptor) enabling Mucorales tissue penetration
- Induction of defects in phagocytic (neutrophil and macrophage) function
- Enhanced CotH expression - a Mucorales-specific protein that mediates host cell invasion by binding GRP78
"The acidosis causes dissociation of iron from sequestering proteins, resulting in enhanced fungal survival and virulence. The ketoacid β-hydroxybutyrate also increases expression of host and fungal receptors that result in fungal adherence and penetration into tissues." - Harrison's 22e
Clinical Progression of Rhinocerebral Mucormycosis:
- Spores inhaled → germinate in nasal mucosa/sinuses
- Hyphae invade blood vessel walls → angioinvasion → thrombosis → tissue necrosis (explains the dark/dusky serosanguineous discharge)
- Spread from sinuses → orbit (proptosis, ophthalmoplegia) → brain (cranial nerve palsies, altered sensorium - as seen here)
- Classic finding: Black eschar on nasal mucosa or palate (due to infarction)
4. Treatment
Treatment requires four simultaneous steps (failure to do all four rapidly = death):
Step 1: Early Antifungal Therapy (URGENT - start before diagnosis confirmed)
Drug of choice: Liposomal Amphotericin B (L-AmB)
- Dose: 5-10 mg/kg/day IV (lipid formulation preferred over deoxycholate AmB due to better safety profile)
- Mechanism: Binds ergosterol in fungal membrane → pore formation → cell lysis
- Do NOT delay - every day of delay doubles mortality
Step-down / combination therapy:
- Isavuconazole - effective alternative once stable; oral bioavailability allows step-down
- Posaconazole - oral step-down therapy after clinical improvement
- Note: Voriconazole has NO activity against Mucorales (and prior voriconazole use is actually a risk factor for breakthrough mucormycosis)
"Multiple studies have found that earlier initiation of polyene-based therapy improves survival of patients with mucormycosis... delaying treatment for mucormycosis with amphotericin B for 6 or more days after diagnosis is associated with a twofold increase in mortality." - Murray & Nadel's Textbook of Respiratory Medicine
Step 2: Surgical Debridement (URGENT)
- Wide surgical excision of all infected, necrotic tissue is mandatory
- Endoscopic sinus surgery + debridement of necrotic nasal/orbital tissue
- Repeat debridement often necessary
- Black eschar on palate or turbinates should be removed
- Surgery is as important as antifungals - neither alone is sufficient
Step 3: Reverse the Underlying Predisposing Condition
- Correct DKA aggressively: IV insulin, IV fluids, electrolyte replacement
- Bring blood glucose under tight control
- Treat metabolic acidosis - this removes the primary growth advantage of the fungus
- Stop any immunosuppressive medications if possible
Step 4: Adjunctive Measures
- Iron chelation: Avoid deferoxamine (serves as a xenosiderophore for Mucorales); consider deferasirox
- Hyperbaric oxygen (adjunct in some centers - improves phagocyte function in acidotic tissue)
- Nutritional support
- Multidisciplinary team: Infectious disease, ENT/surgery, ophthalmology, endocrinology
5. Prognosis
Mucormycosis has one of the highest mortality rates of all fungal infections:
| Form | Approximate Mortality |
|---|---|
| Rhinocerebral (with DKA, treated) | 40-60% |
| Rhinocerebral (with cerebral involvement) | >80% |
| Disseminated | >90% |
| Pulmonary | ~50-80% |
Favorable prognostic factors:
- Early diagnosis and treatment
- Localized (non-cerebral) disease
- Successful surgical debridement
- Rapid correction of DKA/hyperglycemia
- No dissemination at presentation
Poor prognostic factors:
- Cerebral involvement (altered sensorium - as in this patient)
- Bilateral disease
- Delayed diagnosis (>6 days)
- Hematogenous dissemination
- Cavernous sinus thrombosis
This patient has altered sensorium suggesting cerebral involvement, making the prognosis guarded to poor without immediate aggressive intervention.
"Optimizing the chances for successful treatment of mucormycosis requires four steps: (1) early initiation of therapy; (2) surgical debridement, when possible; (3) rapid reversal of underlying predisposing risk factors, if possible; and (4) proceeding to treat underlying malignancy, if present, without waiting." - Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.