Distinguished between infection of foreskin of penis between viral ,fungal , bacteria
balanitis foreskin infection viral fungal bacterial differential diagnosis clinical features
Infections of the Foreskin (Prepuce/Posthitis) and Glans (Balanitis/Balanoposthitis): Viral vs. Fungal vs. Bacterial
1. FUNGAL Infections (Most Common)
Causative Organisms
- Candida albicans - by far the most common single pathogen
- Other Candida spp. less frequently
Risk Factors
- Diabetes mellitus (recurrent candidal balanitis should prompt blood glucose testing)
- Poor hygiene, tight foreskin (phimosis)
- Antibiotic use (disrupts normal flora)
- Immunosuppression (HIV, steroids)
- Sexual contact with partner who has vaginal candidiasis
Clinical Features
- Erythema of the glans and inner prepuce - often vivid red
- Satellite lesions: small pustules or papules around the main erythematous patch (characteristic of Candida)
- Thick, curdy (cottage-cheese-like) white discharge under the foreskin
- Soreness and itch - often more itch than pain
- Skin may appear glazed or shiny
- Unpleasant cheesy odour from smegma accumulation
Diagnosis
- KOH (potassium hydroxide) preparation of swab - shows pseudohyphae and yeast buds
- Swab culture on Sabouraud's agar
Treatment
- First-line: Topical clotrimazole or miconazole cream to glans and prepuce
- Oral: Fluconazole 150 mg single dose for moderate-severe cases; 2-3 doses 72 hours apart for severe/recurrent cases
- Hygiene measures (gentle retraction, washing, drying)
- Recurrent cases: investigate for diabetes
2. BACTERIAL Infections (Second Most Common)
Causative Organisms
- Streptococcus spp. (beta-haemolytic strep most common aerobic cause)
- Staphylococcus aureus
- Pseudomonas spp.
- Neisseria gonorrhoeae (STI-associated)
- Chlamydia trachomatis (STI-associated)
- Gardnerella vaginalis
- Mycoplasma genitalium
- Bacteroides spp.
- Other mixed anaerobes
- Treponema pallidum (syphilis) - presents as a painless chancre
Clinical Features - General Bacterial
- Warmth, erythema, and oedema of glans, foreskin, and sometimes penile shaft
- Purulent, malodorous discharge on foreskin retraction
- Excoriation and tenderness
- Foul smell specifically suggests anaerobic infection
- Discharge, lymphadenopathy, or urethral discharge raises suspicion for STI
Specific Bacterial Presentations
| Organism | Key Feature |
|---|---|
| Streptococcus | Bright erythema, tender, rapid spread possible |
| Anaerobes (Bacteroides) | Foul-smelling discharge, necrotic appearance in severe cases |
| N. gonorrhoeae | Purulent urethral discharge + dysuria; penile oedema |
| T. pallidum (syphilis) | Painless, indurated ulcer (chancre) on prepuce/glans; regional lymphadenopathy |
| Gardnerella | Fishy odour, grey discharge; similar to BV-equivalent |
Diagnosis
- Swab for culture and sensitivity (aerobic + anaerobic)
- STI screen (gonorrhoea, chlamydia, syphilis serology, RPR) if STI suspected
- Urinalysis if dysuria present
Treatment
- Mixed flora / mild: Topical bacitracin + hygiene measures
- Anaerobic infection: Oral metronidazole 500 mg twice daily x 7 days, or clindamycin 300 mg three times daily x 7 days
- Aerobic/streptococcal: Cephalexin (especially in children, 25-50 mg/kg/day divided doses x 7 days)
- Gonorrhoea: Ceftriaxone IM 500 mg + azithromycin
- Syphilitic chancre: Benzathine penicillin G IM
- Severe cellulitis: IV antibiotics and urological consultation
3. VIRAL Infections (Least Common among infectious causes)
Causative Organisms
- Herpes Simplex Virus (HSV-2, less often HSV-1) - most common viral cause
- Human Papillomavirus (HPV) - causes condylomata acuminata (genital warts)
- Molluscum contagiosum
HSV (Genital Herpes)
- Pathognomonic feature: Grouped erythematous vesicles on a red base, on the glans and prepuce
- Vesicles rapidly rupture to form shallow, painful ulcers with erythematous edges
- Pain is prominent - burning/stinging (unlike syphilitic chancre)
- May have prodrome: local tingling, burning before vesicle eruption
- Tender inguinal lymphadenopathy
- Dysuria if urethral involvement
- Recurrent episodes less severe than primary infection (virus remains latent in dorsal root ganglia)
- Systemic symptoms (fever, malaise) more pronounced in primary infection
HPV (Condylomata Acuminata / Genital Warts)
- Soft, flesh-coloured, cauliflower-like papules on the prepuce, coronal sulcus, and glans
- Usually painless unless secondarily infected
- May coalesce into large warty masses
- Diagnosis: clinical (aceto-white test with 5% acetic acid)
- Treatment: Podophyllin, imiquimod cream, cryotherapy, or surgical excision
Molluscum Contagiosum
- Caused by a poxvirus
- Pearly, dome-shaped papules with central umbilication on penile skin and prepuce
- Usually asymptomatic, multiple lesions
- Treatment: cryotherapy, curettage
Quick Comparison Table
| Feature | Fungal (Candida) | Bacterial | Viral (HSV) |
|---|---|---|---|
| Commonest pathogen | C. albicans | Strep spp., anaerobes | HSV-2 |
| Discharge | White, curdy, cheesy | Purulent, grey-green | Serous (from ulcers) |
| Odour | Cheesy/yeasty | Foul (anaerobes) | Absent/mild |
| Primary lesion | Erythema + satellite pustules | Erythema, oedema, pus | Grouped vesicles -> ulcers |
| Pain | Itch >> pain | Pain, warmth, tenderness | Significant pain/burning |
| Lymphadenopathy | Absent | Present if STI (gonorrhoea) | Present (tender inguinal nodes) |
| Systemic symptoms | Absent | Usually absent (fever if severe) | Fever, malaise (primary HSV) |
| Recurrence | Yes (especially with DM) | Less common | Yes (latent ganglionic virus) |
| Key risk factor | Diabetes, antibiotics | Poor hygiene, STI exposure | Unprotected sex |
| Diagnosis test | KOH prep, culture | Swab culture, STI screen | HSV PCR, Tzanck smear |
| Treatment | Clotrimazole/fluconazole | Metronidazole/cephalexin/ceftriaxone | Acyclovir/valacyclovir |
Key Clinical Pearls
- Recurrent Candida balanitis in an adult should always prompt fasting blood glucose to rule out diabetes mellitus.
- Foul smell = anaerobe - think Bacteroides, treat with metronidazole.
- Grouped vesicles = HSV until proven otherwise; never squeeze or incise them.
- A painless indurated ulcer on the prepuce = syphilis (chancre) until serology proves otherwise.
- Infections frequently show mixed flora (fungal + bacterial co-infection); broad-spectrum coverage with topical antifungal + antibiotic may be needed empirically.
- Balanoposthitis can be the sole presenting sign of diabetes - always consider in adult males presenting with recurrent cases.
- Persistent or treatment-refractory balanitis warrants biopsy to exclude premalignant (Erythroplasia of Queyrat) or malignant conditions.
Make a visual poster comparing fungal vs bacterial vs viral foreskin infections
A clean, professional medical education poster titled "Foreskin Infections: Fungal vs Bacterial vs Viral" with three clearly separated columns on a white background. Column 1 - FUNGAL (orange/amber color theme): Header: "FUNGAL (Candida albicans)" with a mushroom/fungal icon - Pathogen: Candida albicans (most common) - Appearance: Vivid red erythema, satellite pustules, glazed shiny skin - Discharge: White, curdy, cottage-cheese-like - Odour: Cheesy/yeasty - Symptoms: Itch > Pain, soreness - Risk Factors: Diabetes, antibiotics, poor hygiene - Diagnosis: KOH prep - pseudohyphae - Treatment: Clotrimazole cream / Fluconazole 150mg oral Column 2 - BACTERIAL (red/crimson color theme): Header: "BACTERIAL (Mixed Flora)" with a bacteria icon - Pathogens: Streptococcus, Staphylococcus, Anaerobes, Gardnerella, Gonorrhoea, Syphilis - Appearance: Erythema, warmth, oedema, purulent exudate - Discharge: Purulent, grey-green - Odour: Foul (anaerobes) - Symptoms: Pain, tenderness, warmth - Key sign: Painless indurated ulcer = Syphilis (chancre) - Diagnosis: Swab culture + STI screen - Treatment: Metronidazole / Cephalexin / Ceftriaxone Column 3 - VIRAL (blue/teal color theme): Header: "VIRAL (HSV / HPV)" with a virus particle icon - Pathogens: HSV-2 (herpes), HPV (warts), Molluscum - Appearance: Grouped vesicles → painful ulcers (HSV); cauliflower warts (HPV); pearly umbilicated papules (Molluscum) - Discharge: Serous - Odour: Absent - Symptoms: Burning pain, prodrome tingling (HSV) - Systemic: Fever + malaise in primary HSV - Diagnosis: HSV PCR swab; aceto-white test (HPV) - Treatment: Acyclovir / Valacyclovir (HSV); Cryotherapy (HPV) Bottom row: A comparison summary table with rows for Discharge, Odour, Pain Level, Lymphadenopathy, Recurrence, Key Diagnostic Test Top of poster: Large bold title in dark navy. Color-coded column headers. Medical illustration style, clear fonts, professional clinical poster aesthetic suitable for a hospital or medical school.
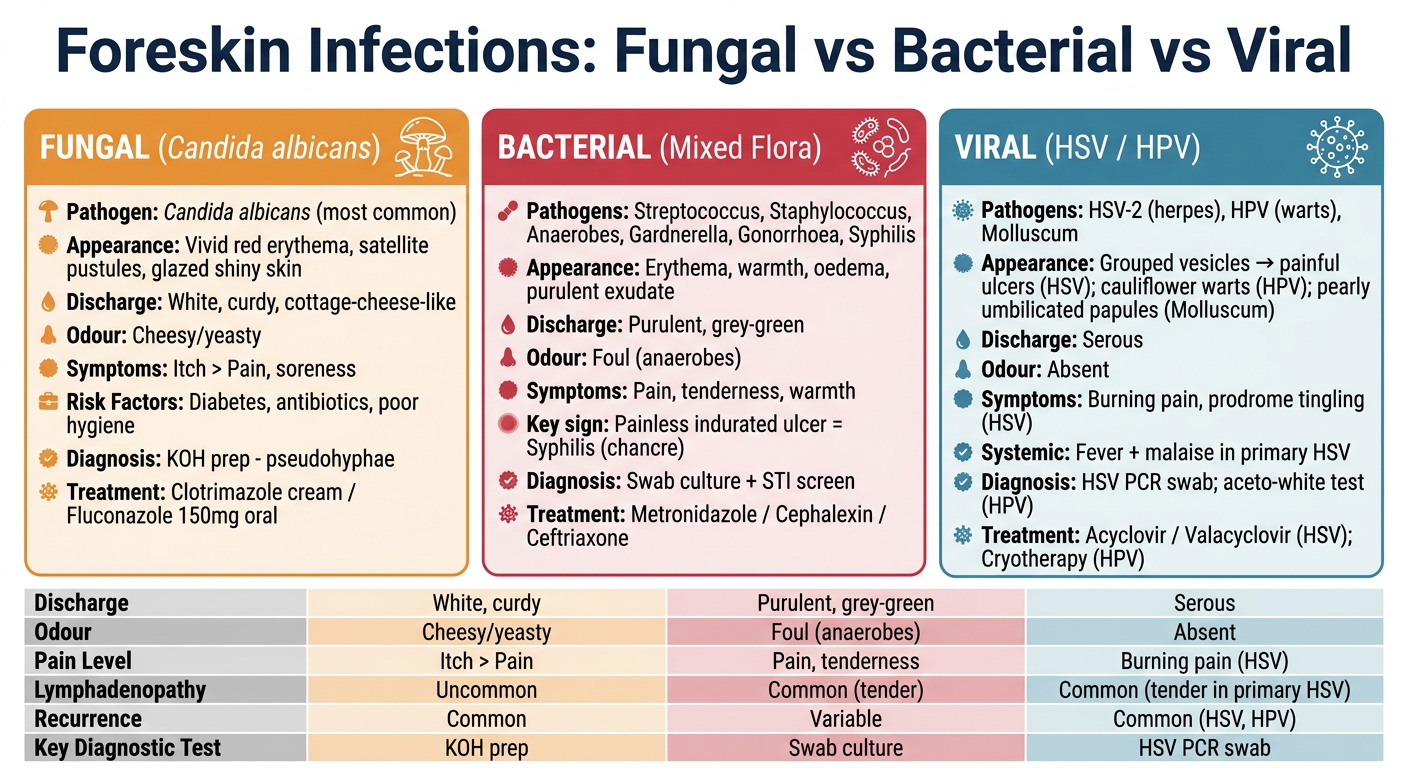
- Orange - Fungal (Candida): itchy, curdy white discharge, satellite pustules, linked to diabetes
- Red - Bacterial (Mixed Flora): purulent/foul discharge, warmth and swelling, includes STI pathogens like gonorrhoea and syphilis
- Blue - Viral (HSV/HPV): grouped vesicles turning to painful ulcers (HSV), cauliflower warts (HPV), with a burning prodrome
Vatakantaka
Vatakantaka Ayurveda heel spur plantar fasciitis symptoms treatment
Vatakantaka plantar fasciitis Agnikarma Ayurveda
Vatakantaka (वातकण्टक)
Etymology & Concept
Modern Correlation
Anatomy (Modern Understanding)
- Originates at the medial calcaneal tuberosity (heel bone)
- Fans out across the sole of the foot
- Inserts into the proximal phalanges (toes)
Ayurvedic Pathology (Samprapti)
| Ayurvedic concept | Meaning |
|---|---|
| Primary dosha | Vata aggravation (cold, dry, mobile qualities) |
| Secondary dosha | Kapha anubandha (Kapha obstructing Vata) - causes heaviness, stiffness, structural changes like heel spur |
| Affected dhatu | Snayu (ligaments/fascia), Asthi (bone), Sandhi (joint) |
| Site | Parshni (heel), Khaduka Pradesh, Gulfa Sandhi (ankle) |
| Nidana (causes) | Ati Shrama (overexertion), walking on uneven surfaces, excess standing, ill-fitting footwear, aggravated Vata diet |
Symptoms
Classic Presentation (both Ayurvedic & Modern)
- Stabbing, pricking, thorn-like pain in the heel
- Worst in the morning (first steps out of bed) or after prolonged rest - classic "post-static dyskinesia"
- Pain lessens with movement initially, then returns with prolonged standing or walking
- Tenderness at the medial calcaneal tuberosity on palpation
- Stiffness of the foot after inactivity
- In chronic/Kapha-dominant cases: mild swelling, heaviness, possible calcaneal spur on X-ray
Red Flags (consider alternative diagnosis)
- Bilateral heel pain - consider rheumatoid arthritis, ankylosing spondylitis, Reiter syndrome
- Pain in younger patients - consider calcaneal stress fracture
- Night pain, systemic symptoms - consider tarsal tunnel syndrome, osteomyelitis
Differential Diagnosis (Modern)
| Condition | Distinguishing Feature |
|---|---|
| Plantar fasciitis | Medial calcaneal tubercle tenderness, worse morning |
| Heel pad atrophy | Diffuse heel tenderness, older patients |
| Calcaneal stress fracture | Squeeze test positive, X-ray/MRI confirms |
| Entrapment of lateral plantar nerve (Baxter's nerve) | Tenderness along nerve course |
| Retrocalcaneal bursitis | Posterior heel pain, Achilles area |
| Tarsal tunnel syndrome | Tingling/numbness, positive Tinel's sign |
Treatment
Ayurvedic Treatments
- Heated metal probe (Panchadhatu Shalaka or Swarna Shalaka) applied to the most tender points of the heel
- Creates focal heat (Ushna, Tikshna guna) - counteracts Vata's cold/dry nature and breaks Kapha obstruction
- Done in multiple sittings; progressively reduces morning pain
- Considered the most effective Ayurvedic intervention for this condition, especially chronic cases
- Padabhyanga (foot massage with medicated oils like Mahanarayan taila, Ksheerabala taila)
- Vata-shamana (Vata-pacifying) property; reduces pain and stiffness
- Leech therapy or venesection at the site
- Reduces local inflammatory load
- Vata-pacifying formulations: Mahayogaraja guggulu, Rasnasaptaka kwatha, Dashamoola kashayam
- Basti (medicated enema) in systemic Vata vitiation
- Warm, unctuous (oily/ghee-rich) foods
- Avoid cold, dry, raw foods
- Warm water consumption
- Good supportive footwear
- Avoid prolonged standing, walking on hard/uneven surfaces
Modern Medical Treatment
- Plantar fascia stretching exercises - most evidence-based intervention
- Calf stretching (tight heel cord is a key risk factor)
- Ice/ice massage to the heel
- Heel cushioning / orthotic devices
- NSAIDs - for analgesia (not true anti-inflammation, as the condition is degenerative)
- Night splints - maintain stretch during sleep
- Corticosteroid injection - short-term relief; risk of plantar fascia rupture and fat pad necrosis with repeated injections
- Autologous blood injection / PRP - under investigation
- Extracorporeal shock wave therapy (ESWT) - mixed results
- Dry needling
- Physical therapy
- Partial plantar fascia release
Comparison: Ayurvedic vs. Modern Parallel
| Feature | Ayurveda (Vatakantaka) | Modern Medicine |
|---|---|---|
| Cause | Vata aggravation, excess exertion | Microtears at calcaneal insertion of plantar fascia |
| Key symptom | Kantaka Ruja (thorn-like pain) in heel | Stabbing plantar heel pain |
| Morning pain | Explained by increased Vata after rest | Post-static dyskinesia |
| Structural change | Kapha-vruta Vata - ossification | Calcaneal spur on X-ray |
| Primary treatment | Agnikarma (thermal therapy) | Stretching, orthotics, ESWT |
| Heat therapy | Agnikarma (direct heat application) | ESWT (acoustic energy) |
| Oil/massage | Padabhyanga | Physical therapy, ultrasound |