Turp syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
TURP syndrome transurethral resection
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive review of TURP Syndrome:
TURP Syndrome
Definition
TURP syndrome describes a constellation of symptoms arising from systemic absorption of large volumes of hypotonic, nonelectrolyte irrigation fluid during transurethral resection of the prostate (or similar endoscopic procedures). It is essentially an iatrogenic form of water intoxication combining circulatory fluid overload, dilutional hyponatremia/hypoosmolality, and solute toxicity from the irrigant.
- Incidence: mild-to-moderate cases 0.78-1.4%; overall <1%
- Mortality: up to 25% in severe cases (serum Na⁺ <120 mEq/L)
- Onset: 15 minutes to 24 hours after resection begins
Mechanism / Pathophysiology
Irrigation fluid is absorbed through opened prostatic venous sinuses. On average, 10-30 mL/min of fluid is absorbed per minute of resection, making prolonged procedures especially dangerous.
Factors governing absorption rate:
- Height of irrigation bag above the table (hydrostatic pressure)
- Degree of bladder distension
- Extent of venous sinus opening
- Duration of resection
Three interrelated pathophysiologic arms:
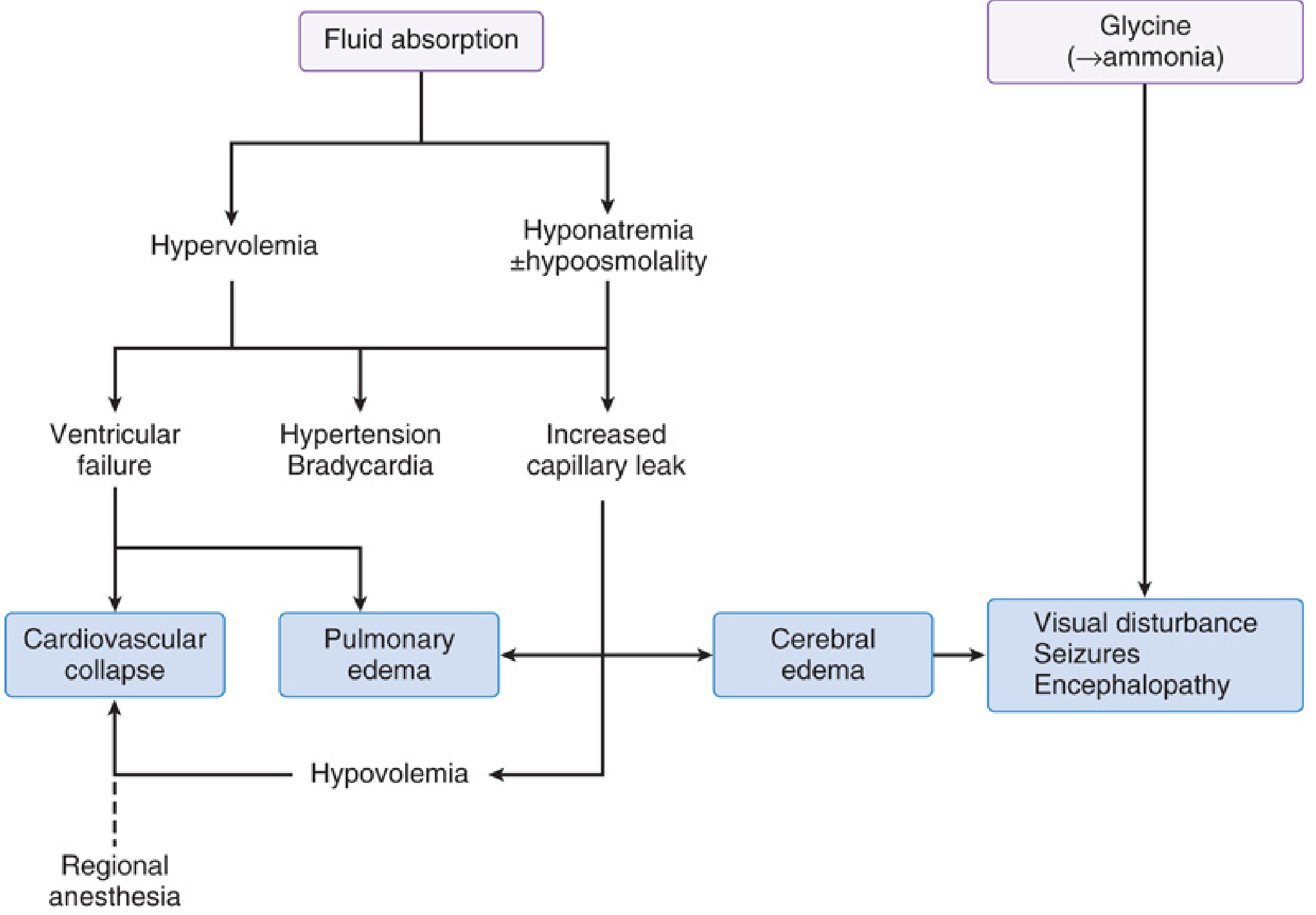
1. Hypervolemia
- Acute volume expansion → hypertension + bradycardia initially
- Ventricular failure + pulmonary edema in patients with reduced cardiac reserve
- Hypertension + hyponatremia cause osmotic/hydrostatic water shift out of vasculature → pulmonary edema → hypovolemic shock (paradoxical late hypotension)
- Regional anesthesia further aggravates hypotension
2. Hyponatremia / Hypoosmolality
- Dilutional hyponatremia from hypotonic fluid absorption
- Acute hypoosmolality drives free water into brain → cerebral edema
- CNS symptoms correlate with rapidity of fall:
- <120 mEq/L: restlessness, confusion, hypotension, pulmonary edema, CHF
- <115 mEq/L: ECG changes (widened QRS, ventricular ectopy, ST elevation)
- <110 mEq/L: seizures, loss of consciousness
- ~100 mEq/L: respiratory and cardiac arrest
3. Solute toxicity (depends on irrigant used)
Irrigating Solutions and Their Toxicities
| Solution | Osmolality | Toxicity |
|---|---|---|
| Glycine 1.5% | 230 mOsm/L | Transient blindness (retinal inhibitory NT), hyperammonemia (glycine → ammonia), cardiac T-wave changes |
| Sorbitol 2.7% + Mannitol 0.54% | 195 mOsm/L | Hyperglycemia (sorbitol), intravascular volume expansion (mannitol) |
| Distilled water | 0 mOsm/L | Massive hemolysis - largely abandoned |
| Normal saline (bipolar TURP) | Isotonic | No hyponatremia; risk of volume overload only |
Electrolyte solutions cannot be used in monopolar TURP as they disperse the diathermy current.
Glycine-Specific Toxicity
- Glycine is an inhibitory neurotransmitter in the retina - causes transient blindness with sluggish/nonreactive pupils (vs. cerebral edema where pupillary reflexes are normal)
- Acts on NMDA receptors (allosteric activation) - lowers seizure threshold
- Metabolized hepatically to ammonia → encephalopathy, nausea/vomiting within 1 hour post-op
- CNS toxicity appears when serum ammonia >100 μmol/L; coma possible at higher levels
Clinical Manifestations
Cardiovascular
- Early: hypertension, bradycardia (volume overload)
- Late: hypotension, pulmonary edema, congestive heart failure, cardiovascular collapse
CNS / Neurological
- Headache, restlessness, confusion, agitation
- Visual disturbances (transient blindness - glycine)
- Seizures, coma
- Encephalopathy (ammonia)
Respiratory
- Dyspnea, cyanosis, pulmonary edema
Other
- Nausea, vomiting
- Arrhythmias
- Hemolysis (if hypotonic solutions used)
Risk Factors
- Large prostate (>45 g) requiring longer resection
- Resection time >90 minutes
- High irrigation bag pressure
- High intravesical pressure
- Extensive venous sinus opening
- Large irrigation volumes used
- Use of hypotonic irrigants
Diagnosis
TURP syndrome is a clinical diagnosis supported by:
- Serum sodium (check if symptoms arise intraoperatively or postoperatively)
- Serum osmolality
- Serum ammonia (if glycine irrigant used)
- ECG monitoring (QRS widening, ST changes)
- Monitoring fluid balance: irrigant instilled vs. drained
Treatment
Treatment is guided by severity and intravascular volume status:
| Severity | Management |
|---|---|
| Mild | Fluid restriction + IV furosemide (loop diuretic to excrete free water) |
| Severe hyponatremia with seizures/coma | Hypertonic saline (3% or 5% NaCl) - correct Na⁺ cautiously |
| Seizures | Midazolam 2-4 mg IV; Mg²⁺ (counteracts glycine's NMDA activation and dilutional hypomagnesemia) |
| Airway compromise | Endotracheal intubation to prevent aspiration |
| Normal/near-normal osmolality | Hemodialysis preferred over hypertonic saline |
| Hypoxemia/hypoperfusion | Treat supportively |
Caution with hypertonic saline: Correct Na⁺ no faster than 8-10 mEq/L per 24 hours to avoid osmotic demyelination syndrome.
Prevention
- Use bipolar TURP with isotonic saline irrigation (eliminates hyponatremic risk)
- Monitor fluid balance continuously; stop surgery if >750-1000 mL absorbed (females) or >2000 mL (males)
- Limit resection to <90-120 minutes
- Keep intravesical pressure <15-25 mmHg
- Use regional anesthesia (spinal/epidural) - the awake patient can report symptoms early, allowing earlier detection
- Warm irrigation solutions (also prevents hypothermia)
Anesthetic Preference
Regional (spinal) anesthesia is preferred for TURP because:
- Patient remains awake - early CNS symptoms (confusion, visual changes) can be reported
- Sensory level can be monitored to detect significant fluid shifts
- Associated with lower 30-day mortality vs. general anesthesia in large database studies
- Neuraxial anesthesia does NOT affect blood loss or postoperative cognitive function vs. general anesthesia
Modern Context
Advances in surgical technique have markedly reduced TURP syndrome:
- Bipolar TURP uses normal saline - eliminates hyponatremia risk (volume overload risk remains)
- Laser ablation, radiofrequency ablation, photodynamic and thermal therapy, cryotherapy
- These alternatives have reduced both incidence and severity of TURP syndrome significantly
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1303-1304 | Miller's Anesthesia, 10e, pp. 8471-8476, 6372-6374
This is a shared conversation. Sign in to Orris to start your own chat.