Audiometry
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the complete, well-structured answer.
Audiometry
Audiometry is the systematic measurement of hearing sensitivity and function. It encompasses a battery of tests that characterize hearing thresholds, middle ear function, cochlear status, and central auditory processing. The following is a structured overview drawn from K.J. Lee's Essential Otolaryngology, Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, Cummings Otolaryngology Head and Neck Surgery, and Shambaugh Surgery of the Ear.
1. Pure-Tone Audiometry (PTA)
Pure-tone audiometry is the foundation of audiometric testing. It determines hearing thresholds (the lowest level at which the patient responds at least 50% of the time) for sinusoidal tones at specified frequencies.
Key Parameters
- Frequencies tested: Octave intervals from 250 to 8000 Hz (i.e., 250, 500, 1000, 2000, 4000, 8000 Hz). Inter-octave frequencies (750, 1500, 3000, 6000 Hz) are added when there is a 25 dB or greater difference between adjacent octave thresholds, or for ototoxicity monitoring and hearing aid fitting.
- Bone conduction (BC) testing is performed when air-conduction (AC) thresholds are 15 dB HL or greater.
- Standards governing PTA include ISO 8253-1:2010 and IEC 60645-1:2017.
Reliability Factors (K.J. Lee's)
- Sound-treated booth (quiet enough to measure 0 dB HL)
- Annual equipment calibration
- Trained audiologist
- Clear otoscopic inspection before testing
- Proper earphone/bone oscillator placement
- Developmentally appropriate patient instructions
The Audiogram
The pure-tone audiogram is a graph with frequency (Hz) on the logarithmic x-axis and hearing level (dBHL) on the y-axis (0 dBHL = average threshold of otologically normal young adults). Levels are plotted descending downward (greater loss = lower on graph).
Standard symbols:
| Ear | AC (Unmasked) | AC (Masked) | BC (Unmasked) | BC (Masked) |
|---|---|---|---|---|
| Right (red) | O | △ | < | [ |
| Left (blue) | X | □ | > | ] |
The "speech banana" is a shaded zone on the audiogram (125-8000 Hz, 20-60 dBHL) representing conversational speech sounds, used for patient counselling.
2. Masking
When testing one ear, the opposite (non-test) ear may pick up the signal through skull vibration - this is crossover. The loss of sound energy crossing the skull is interaural attenuation (IA):
| Transducer | IA |
|---|---|
| Supra-aural earphones (AC) | 40-65 dB (frequency-dependent) |
| Insert earphones (AC) | 70-90 dB |
| Bone conduction | 0-10 dB |
Rules for when to mask (K.J. Lee's):
- Air conduction: Mask the non-test ear whenever the AC stimulus to the test ear exceeds the BC threshold of the non-test ear by 40 dB.
- Bone conduction: Mask the non-test ear whenever the difference between the AC threshold of the test ear and the BC threshold exceeds 10 dB (i.e., an air-bone gap is present).
The preferred masker for pure tones is narrow-band noise centered on the test frequency; for speech, speech-spectrum noise is used.
3. Degree of Hearing Loss
Adult Classification (Roeser et al., used widely)
| PTA Range (dBHL) | Degree |
|---|---|
| 0-25 | Within normal limits |
| 26-40 | Mild |
| 41-55 | Moderate |
| 56-70 | Moderately severe |
| 71-90 | Severe |
| 91+ | Profound |
Pediatric Classification (Northern & Downs, 2002)
| Range (dBHL) | Degree |
|---|---|
| 0-15 | Within normal limits |
| 15-25 | Slight |
| 25-30 | Mild |
| 30-50 | Moderate |
| 50-70 | Severe |
| 70+ | Profound |
(A child's scale is more conservative because hearing loss, even mild, impairs speech and language acquisition)
British Society of Audiology (BSA, 2011) - based on average of 250, 500, 1000, 2000, 4000 Hz:
- Mild: 21-40 dB
- Moderate: 41-70 dB
- Severe: 71-95 dB
- Profound: 96 dB and above
AMA Formula for Percentage Hearing Loss (medicolegal)
- Average thresholds at 500, 1000, 2000, 3000 Hz per ear.
- Subtract 25.
- Multiply by 1.5 → gives % hearing loss per ear.
- Binaural: (better ear % × 5 + worse ear %) ÷ 6.
4. Types of Hearing Loss
| Type | Air Conduction | Bone Conduction | Air-Bone Gap |
|---|---|---|---|
| Conductive | Elevated | Normal | Present (≥10 dB) |
| Sensorineural (SNHL) | Elevated | Elevated equally | Absent (<10 dB) |
| Mixed | Elevated | Elevated (but less) | Present |
Carhart notch: A characteristic dip at 2 kHz in the bone-conduction thresholds (≥10 dB between 0.5 and 4 kHz). Associated with otosclerosis and otitis media with effusion (OME); it is a mechanical artefact of the middle ear pathology, not true sensorineural loss. It resolves after successful middle ear surgery. - Scott-Brown's Otorhinolaryngology, Vol. 2
5. Speech Audiometry
Speech audiometry supplements pure-tone testing to assess the functional impact of hearing loss and for rehabilitation monitoring.
Speech Awareness/Detection Threshold (SAT/SDT)
- Lowest level at which the patient detects the presence of speech (not necessarily understands it).
- Used when SRT cannot be obtained (infants, cognitive impairment, language barrier).
- Should be within 10 dB of the best pure-tone threshold anywhere across 250-8000 Hz.
Speech Recognition Threshold (SRT)
- Lowest level (dBHL) at which the patient correctly repeats spondees (bisyllabic words with equal stress on both syllables, e.g., "railroad," "sidewalk") in 50% of presentations.
- Should be within 10 dB of the pure-tone average (PTA) at 500, 1000, 2000 Hz. In steeply sloping audiograms, a best two-frequency PTA may better corroborate the SRT.
Word (Speech) Recognition Score (WRS/SRS) - formerly Speech Discrimination
- Presented at 25-35 dB above SRT (sensation level, SL) to obtain maximum score.
- Uses phonetically balanced (PB) word lists where phoneme occurrence mirrors connected speech.
| WRS Score | Interpretation |
|---|---|
| 90-100% | Normal |
| 76-88% | Slight difficulty |
| 60-74% | Moderate difficulty |
| 40-58% | Poor |
| ≤40% | Very poor |
Current role of speech audiometry: Primarily rehabilitation outcome assessment for hearing aids and cochlear implants. Its former role in distinguishing cochlear from retrocochlear lesions (acoustic neuroma) has been largely superseded by MRI. - Scott-Brown's
6. Immittance Audiometry (Tympanometry + Acoustic Reflexes)
Tympanometry
An objective test measuring the mobility (compliance/admittance) of the tympanic membrane as a function of applied external canal air pressure. Compliance is expressed in millimhos (mMho) or equivalent air volume (cm³/mL); pressure in dekapascals (daPa).
Tympanogram Types:
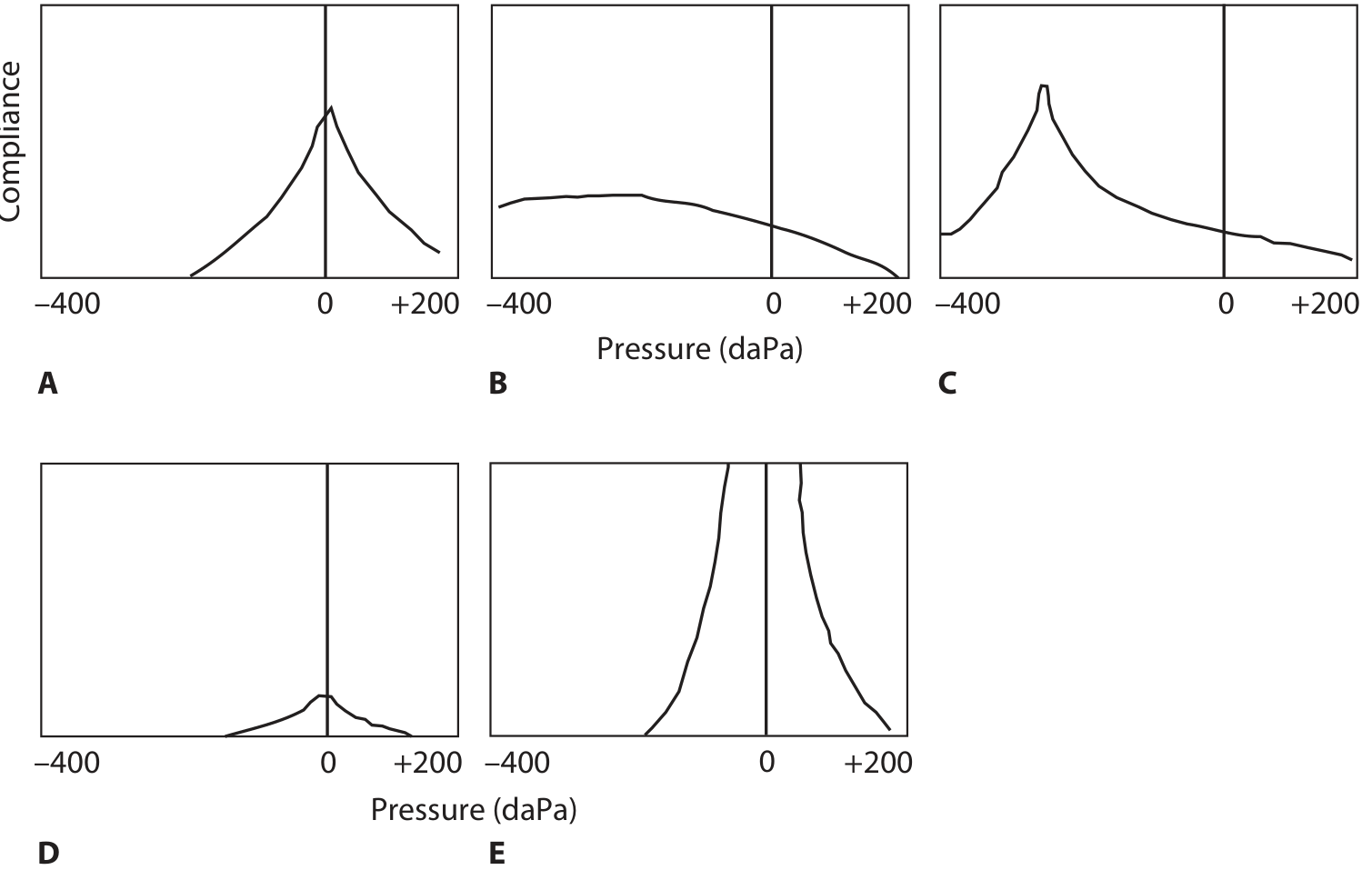
Tympanogram types A-E. A = normal; B = flat (OME or perforation); C = negative middle ear pressure; D (As) = reduced compliance (otosclerosis); E (Ad) = increased compliance (ossicular discontinuity). - K.J. Lee's Essential Otolaryngology
| Type | Peak Pressure | Peak Compliance | Clinical Significance |
|---|---|---|---|
| A | -100 to +100 daPa | Normal | Normal middle ear |
| As (A shallow) | Normal range | Low | Otosclerosis, scarred TM, malleus fixation |
| Ad (A deep) | Normal range | High (hypercompliant) | Ossicular chain discontinuity, flaccid TM |
| B | No clear peak | Flat/very low | OME (normal canal volume), perforation/PE tube (large canal volume) |
| C | < -100 daPa (adults), < -150 daPa (children) | Normal-low | Eustachian tube dysfunction, retracted TM |
Acoustic Reflex Testing
- Measures the lowest stimulus level eliciting the stapedial reflex (bilateral contraction of stapedius in response to loud sound).
- Normal acoustic reflex thresholds: 70-100 dB HL.
- Ipsilateral reflex arc: Acoustic nerve → ipsilateral CN → trapezoid body → ipsilateral facial motor nucleus → facial nerve → stapedius.
- Contralateral reflex arc: Acoustic nerve → ipsilateral CN → contralateral medial superior olive → contralateral facial motor nucleus → contralateral stapedius.
- Reflex is absent when: (1) significant conductive pathology in the recording ear, or (2) hearing loss ≥65 dB HL in the stimulated ear.
7. Otoacoustic Emissions (OAEs)
OAEs are low-level acoustic signals generated by outer hair cells (OHCs) of the cochlea and transmitted outward through the middle ear to the ear canal, where they are recorded by a sensitive microphone. They are an objective, non-invasive "window" into cochlear (OHC) function. They do not require behavioral responses and can be used in neonates and sleeping patients.
Pathway of energy: OHC → basilar membrane → cochlear fluids → oval window → ossicles → tympanic membrane → external ear canal.
Key limitation: OAEs are absent (or reduced) in conductive hearing loss, because the conductive mechanism blocks both inward and outward sound transmission. Normal middle ear function must be confirmed before interpreting absent OAEs.
Types of OAEs
| Type | Stimulus | Clinical Use |
|---|---|---|
| Spontaneous OAEs (SOAEs) | None (self-generated) | Present in 35-60% of normals; absence is non-diagnostic; rarely used clinically |
| Transient-evoked OAEs (TEOAEs) | Brief clicks or tone bursts | Neonatal hearing screening; cochlear hearing better/worse than ~30-40 dB at each octave band |
| Distortion Product OAEs (DPOAEs) | Two simultaneous tones (f1 and f2) | Cochlear function by frequency; monitoring ototoxicity; useful when TEOAE is borderline |
- If TEOAEs are present, cochlear (OHC) function is intact up to ~30-40 dB HL.
- TEOAEs are absent in cochlear SNHL >30-40 dB, but present in purely neural (retrocochlear) lesions.
- This distinction (absent OAEs + normal ABR vs. present OAEs + abnormal ABR) helps identify auditory neuropathy spectrum disorder (ANSD).
8. Auditory Brainstem Response (ABR)
The ABR is a surface-recorded averaged electrophysiological response representing auditory pathway activity from the cochlear nerve to the midbrain, occurring within 10 ms of stimulation. - Cummings Otolaryngology
Wave Generators
| Wave | Neural Generator |
|---|---|
| I | Distal cochlear nerve |
| II | Proximal cochlear nerve (near porus acusticus) |
| III | Cochlear nucleus complex |
| IV | Superior olivary complex |
| V | Lateral lemniscus (midbrain) |
Uses
- Threshold estimation (especially in infants, non-cooperative patients) - using click or frequency-specific tone pip stimuli.
- Neurodiagnosis - retrocochlear pathology (acoustic neuroma): prolonged I-III and I-V interpeak latencies.
- Intraoperative monitoring during surgeries near auditory structures (CPA tumors, cochlear implant).
Technical Notes
- 1000-3000 sweeps averaged per condition; responses must be replicated.
- Electrode placement: vertex (non-inverting), ipsilateral and contralateral earlobes (inverting), forehead (ground).
- Band-pass filter: 100 Hz (high-pass) to 1000-3000 Hz (low-pass).
- Audiometric evaluation must always precede ABR to set appropriate stimulus levels.
9. Special Audiometric Techniques
| Test | Purpose |
|---|---|
| High-frequency audiometry (up to 16-20 kHz) | Monitoring ototoxic drug effects before standard frequencies are affected |
| Bekesy audiometry | Distinguish cochlear from retrocochlear (now largely replaced by ABR/MRI) |
| SISI (Short Increment Sensitivity Index) | Tests for recruitment (cochlear lesion) |
| Tone decay test | Detects adaptation/fatigue (retrocochlear lesion) |
| Behavioral observation audiometry (BOA) | Infants <6 months |
| Visual reinforcement audiometry (VRA) | Infants 6 months to 2.5 years |
| Play audiometry (conditioned play) | Children 2.5-5 years |
| Conventional PTA | Children ≥3.5 years (obtainable in ~95%) |
10. Screening Audiometry
Per ISO 8253-1:2010, screening audiometry produces a pass/fail outcome rather than defined thresholds. Automated audiometry is commonly used for occupational/industrial hearing surveillance.
Summary: The Audiometric Test Battery
| Test | What It Measures | Requires Behavior? |
|---|---|---|
| Pure-tone audiometry | Hearing sensitivity by frequency | Yes |
| Speech audiometry | Functional hearing for speech | Yes |
| Tympanometry | Middle ear mobility/pressure | No |
| Acoustic reflexes | Stapedial reflex arc integrity | No |
| OAEs | Outer hair cell function | No |
| ABR | Auditory pathway electrophysiology | No |
Sources: K.J. Lee's Essential Otolaryngology, pp. 296-314; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, Ch. 51; Cummings Otolaryngology Head and Neck Surgery, Ch. 134; Shambaugh Surgery of the Ear.
This is a shared conversation. Sign in to Orris to start your own chat.