Narrow band imaging and ELS classification. MS ent University exam pattern for 20 marks.
Reading File
Finding Sources
Finding Sources
Searching the Web
NBI narrow band imaging ELS classification laryngoscopy ENT exam
Reading File
Reading Web Page
https://docs.bvsalud.org/biblioref/2025/05/1340011/the-impac…
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the material needed for a comprehensive 20-mark MS ENT university exam answer. Let me compile it.
Narrow Band Imaging (NBI) and ELS Classification
MS ENT University Exam Answer - 20 Marks
DEFINITION AND PRINCIPLE OF NBI (4 marks)
Narrow Band Imaging (NBI) is an optical image enhancement technology (a form of "biologic endoscopy") that uses specific wavelengths of light to enhance visualization of mucosal and submucosal vascular structures, allowing detection of early neoplastic changes without dyes or stains.
Physical Basis
White light contains the full visible spectrum. NBI uses mechanical optical filters to narrow the broadband white light to two specific wavelengths:
| Band | Wavelength | Color | Tissue Target |
|---|---|---|---|
| First | 415 nm (range 400-430 nm) | Blue | Superficial capillaries (mucosal surface) |
| Second | 540 nm (range 525-555 nm) | Green | Submucosal vascular pattern |
Both wavelengths correspond to absorption peaks of hemoglobin. Because hemoglobin strongly absorbs these wavelengths, blood vessels appear as dark brown/black structures sharply contrasted against the green-brown mucosal background. This creates high-contrast visualization of even the finest microvascular detail.
- Blue light (415 nm) - short wavelength, shallower penetration - highlights mucosal capillaries (appears brown)
- Green light (540 nm) - deeper penetration - highlights submucosal veins (appears cyan/turquoise)
Key Concept: IPCL (Intraepithelial Papillary Capillary Loops)
Normal laryngeal epithelium contains IPCLs - tiny capillary loops that run longitudinally (in 2D) within the vocal fold epithelium. In malignant transformation, neoangiogenesis occurs and new vessels grow perpendicularly (into the 3rd dimension), becoming tortuous, irregular, and dilated. NBI visualizes these changes with much higher sensitivity than white-light endoscopy (WLE).
APPLICATIONS OF NBI IN ENT (3 marks)
- Early laryngeal cancer detection - detects submucosal vascular patterns under leukoplakia that WLE cannot; increases sensitivity for laryngeal cancer by ~23% over WLE
- Biopsy guidance - directs biopsy to most "suspicious" vascular areas, improving diagnostic yield in laryngeal and hypopharyngeal lesions
- Assessment of leukoplakia - identifies areas of malignant transformation hidden beneath white plaques
- Intraoperative margin assessment - used during transoral laser microsurgery (TLM) to reduce superficial positive margins by ~85%
- Recurrent respiratory papillomatosis (RRP) - differentiates papilloma from malignant lesions based on turning point angles of perpendicular IPCL changes
- Post-treatment surveillance - follow-up of patients treated for laryngeal cancer
Compared to WLE: NBI detects 18% more true-positive laryngeal cancer lesions and maintains high specificity (~96%).
NBI CLASSIFICATION SYSTEMS (5 marks)
A. Ni et al. Classification (2011) - Most Widely Used
Classified IPCL morphology in the larynx into 5 types:
| Type | IPCL Features | Clinical Significance |
|---|---|---|
| Type I | Thin, oblique, arborescent vessels; NO IPCLs visible | Normal |
| Type II | IPCLs not visible; oblique/arborescent vessels with larger diameter | Benign lesion |
| Type III | White mucosa covers IPCLs - prevents their visualization | Benign (leukoplakia) |
| Type IV | IPCLs visible as dark brown spots | Pre-malignant |
| Type V (Va, Vb, Vc) | Irregular, tortuous, dilated IPCLs with various morphologies | Malignant |
Reported performance: Sensitivity 89%, Specificity 93%, PPV 91%, NPV 92%, Accuracy 90%.
B. ELS (European Laryngological Society) Classification (2015) - Simpler, Practical
Proposed in 2015 as a simplified two-pattern system that is more practical for daily clinical use.
The ELS classification divides vascular patterns into just two categories based on the dimension of vascular growth:
1. LONGITUDINAL PATTERN (Benign)
- Vessels remain in two dimensions (length and width of the vocal fold)
- Features: ectasia, increased vessel density, increased vessel branching
- Vessels run parallel/longitudinal to the vocal fold long axis
- Associated with BENIGN lesions - polyps, nodules, Reinke's edema, contact granuloma
2. PERPENDICULAR PATTERN (Malignant/Pre-malignant)
- Vessels grow in the third dimension (perpendicular to the mucosal surface)
- These represent true IPCLs visible as dot-like or loop structures
- Two sub-types based on the angle of turning points:
- Gentle/regular turning angles → Recurrent Respiratory Papillomatosis (RRP)
- Irregular/chaotic turning angles → Pre-malignant or malignant lesions (SCC)
Reported performance: Sensitivity 100%, Specificity 95%, PPV 100%, NPV 96% (Sifrer et al.)
COMPARISON: NI et al. vs ELS CLASSIFICATION (2 marks)
| Feature | Ni et al. (2011) | ELS (2015) |
|---|---|---|
| Number of types | 5 (I-V) | 2 (Longitudinal / Perpendicular) |
| Complexity | More detailed, complex | Simpler, practical |
| Clinical use | Research, detailed analysis | Routine clinical use |
| Sub-differentiation | Va, Vb, Vc for malignant types | Uses turning point angle for RRP vs SCC |
| Sensitivity | 89% | 100% |
| Specificity | 93% | 95% |
The ELS classification is preferred for routine clinical use as it is the simplest and most practical for identifying various laryngeal lesions.
ENDOSCOPIC IMAGES
Fig 1: True vocal fold scar at anterior commissure
(A) White Light Imaging - vascular pattern poorly defined; (B) NBI - submucosal vessels sharply delineated in brown/cyan contrast
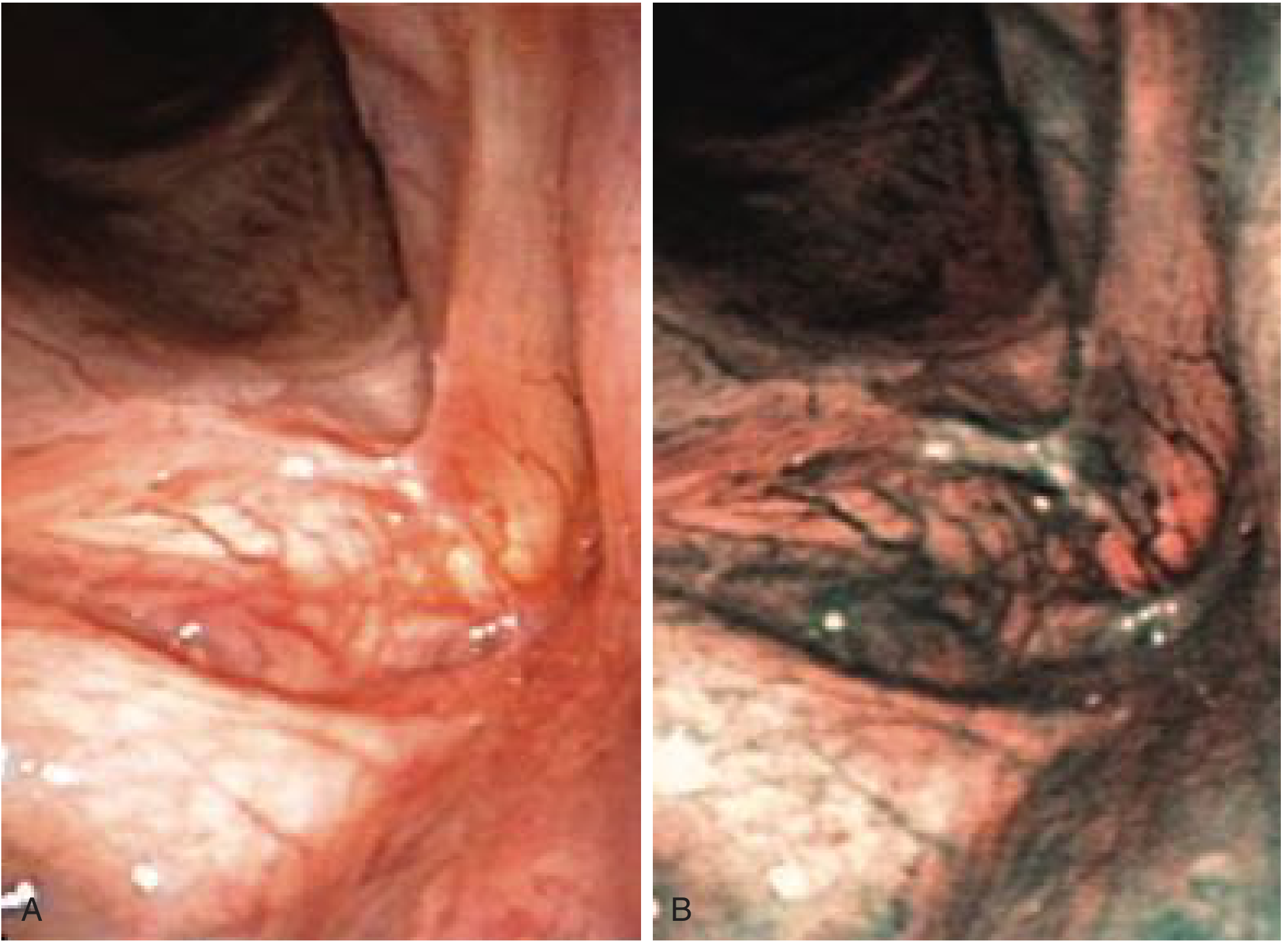
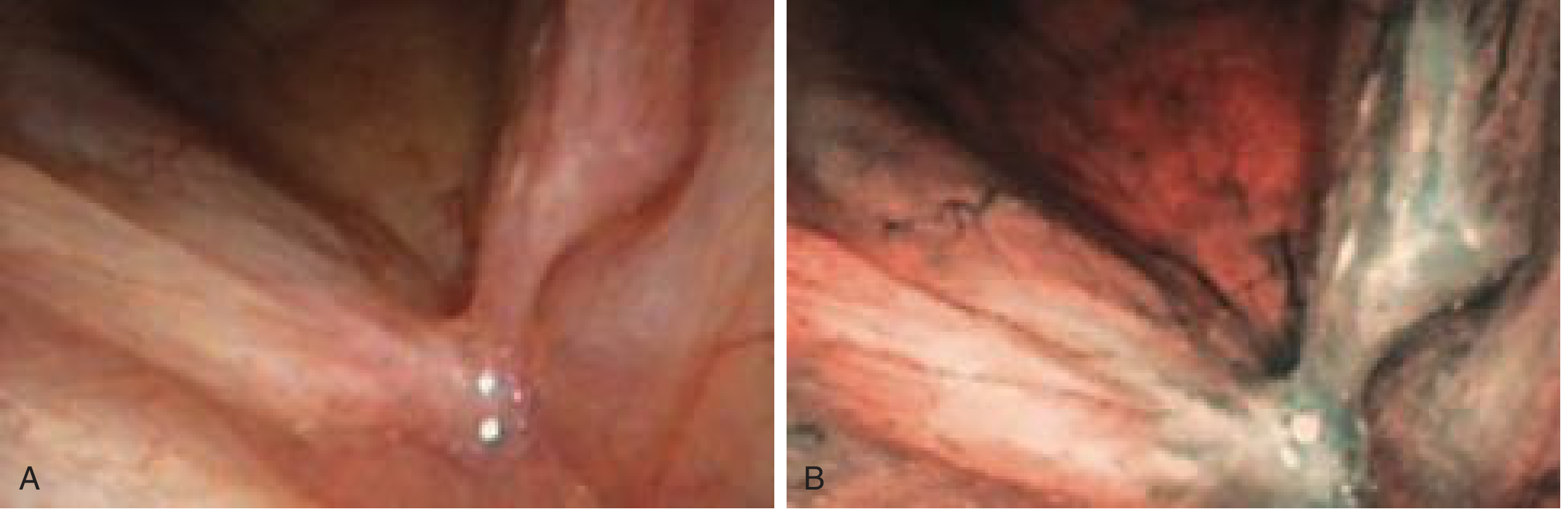
Fig 2: Carcinoma in situ, left true vocal fold
(A) White Light Imaging - subtle mucosal change; (B) NBI - abnormal perpendicular IPCL pattern clearly visible as dark tortuous vessels
ADVANTAGES OF NBI OVER WLE (2 marks)
- No dyes or contrast agents needed - purely optical, no drug administration
- Real-time imaging at standard endoscopy - no extra time or setup
- Better visualization of lesions covered by thick white plaques (leukoplakia)
- Guides targeted biopsy - reduces sampling error
- Helps define surgical margins intraoperatively (reduces positive margins by ~85%)
- Cost-effective - built into standard Olympus endoscopy systems at no extra cost
- Differentiates papilloma from SCC based on IPCL turning point morphology
LIMITATIONS (2 marks)
- Significant learning curve - requires training in IPCL pattern recognition
- Reduced sensitivity for advanced/bulky lesions - thick overlying tissue limits penetration
- NBI appearance of some benign conditions can mimic malignancy (e.g., laryngeal amyloidosis, histoplasmosis)
- Not a substitute for biopsy - histopathology remains the gold standard
- Performance varies with resolution of the endoscope - best with HDTV systems
- Limited utility for lesions <1 cm (early superficial lesions in practice)
RECENT EVIDENCE (2 marks)
A 2021 validation study (PMID 33710441) confirmed that the ELS classification for NBI vascular changes in glottic lesions is a highly reliable tool whose systematic use allows better diagnostic evaluation. Studies pooled across institutions (Rzepakowska et al., Sifrer et al., Volgger et al.) show consistent performance:
- Preoperative NBI: Sensitivity 84-100%, Specificity 73-97%, Accuracy 83-98%
- Intraoperative NBI: Sensitivity 98-100%, Accuracy 85-95%
SUMMARY TABLE FOR QUICK RECALL
| Parameter | Detail |
|---|---|
| Technology | Optical bandpass filter; no dye |
| Wavelengths | 415 nm (blue) + 540 nm (green) |
| Target structure | IPCL (Intraepithelial papillary capillary loops) |
| Key finding in malignancy | Perpendicular vessel growth (3rd dimension) |
| Ni classification | 5 types (I to V) |
| ELS classification | 2 patterns: Longitudinal (benign) / Perpendicular (malignant) |
| ELS - perpendicular sub-types | Regular turning angle = RRP; Irregular = pre-malignant/SCC |
| Sensitivity (ELS) | 100% |
| Specificity (ELS) | 95% |
| Gold standard | Still histopathology/biopsy |
Sources: Cummings Otolaryngology Head & Neck Surgery (7th ed), Ch. 54; Saraniti et al., International Archives of Otorhinolaryngology 2021; ELS NBI Validation Study; PMC9895569
This is a shared conversation. Sign in to Orris to start your own chat.