Seminar on Pulse examination
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have comprehensive material from multiple authoritative sources. Let me compile the full seminar.
Seminar on Pulse Examination
1. Introduction
The pulse is a palpable pressure wave transmitted through the arterial wall, generated by ventricular systole ejecting blood into the aorta. Examination of the pulse is one of the oldest and most fundamental clinical skills - it provides a direct window into cardiovascular hemodynamics before any investigation is ordered.
"In the clinical evaluation of cardiovascular disorders, the physical examination is a reflection of underlying hemodynamics. A well-performed physical examination is necessary to provide an initial clinical impression of the type and severity of cardiac disease."
- Fuster and Hurst's The Heart, 15th Edition
2. Sites of Pulse Examination
Peripheral pulses that should be assessed routinely include:
| Site | Vessel | Clinical Use |
|---|---|---|
| Radial (wrist) | Radial artery | Rate, rhythm, character |
| Carotid (neck) | Common carotid | Best for contour/character |
| Brachial (antecubital fossa) | Brachial artery | Useful in obese necks, carotid disease |
| Femoral (groin) | Femoral artery | Peripheral vascular disease, coarctation |
| Popliteal (behind knee) | Popliteal artery | Lower limb ischaemia |
| Dorsalis pedis (dorsum of foot) | Dorsalis pedis | PVD screening |
| Posterior tibial (behind medial malleolus) | Posterior tibial | PVD screening |
| Temporal | Temporal artery | Temporal arteritis |
Key point: Simultaneous palpation of the radial and femoral pulses detects radio-femoral delay - a hallmark of coarctation of the aorta. One of the two pedal pulses may be absent in up to 10% of normal subjects, but the pair should be symmetric.
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Carotid precautions:
- Never examine both carotids simultaneously (risk of syncope/cerebral ischaemia)
- Never press hard - can precipitate carotid sinus hypersensitivity and syncope, especially in the elderly
- Always auscultate for a bruit before palpating
3. Technique of Palpation
Radial Pulse
The radial pulse is examined at the wrist, using the index and middle fingertips placed over the radial artery lateral to the flexor carpi radialis tendon. The thumb should never be used (has its own pulse).
Brachial Pulse
Rest the patient's elbow on the examiner's palm. Palpate with the thumb; the brachial pulse is deeper than others. Gently extend/flex the arm to improve palpation.
Carotid Pulse
Palpate with the right fingerpads; mobilize the sternocleidomastoid muscle laterally. Once the artery is identified, assess amplitude and contour.
- Fuster and Hurst's The Heart, 15th Edition
Allen's Test: Assesses integrity of the palmar arch before radial artery cannulation - compress both radial and ulnar arteries, release the ulnar, and assess return of colour.
4. Characteristics of the Normal Pulse
Six key features are assessed systematically:
| Feature | What It Indicates |
|---|---|
| Rate | Fast or slow |
| Rhythm | Regular or irregular |
| Volume | Reflects pulse pressure (systolic - diastolic BP) |
| Character / Contour | Waveform shape - reflects stroke volume, ejection velocity, vascular compliance, SVR |
| Tension / Force | Diastolic (tension) and systolic (force) blood pressure |
| Condition of arterial wall | e.g., atherosclerotic thickening, thickened, tortuous wall |
- S Das, A Manual on Clinical Surgery, 13th Edition
5. Rate
- Normal: 60-100 beats/minute
- Tachycardia: >100 bpm - seen in fever, shock, thyrotoxicosis, anaemia, anxiety, heart failure
- Bradycardia: <60 bpm - seen in heart block, hypothyroidism, athletic training, vasovagal
6. Rhythm
- Regular: Normal sinus rhythm
- Regularly irregular: e.g., Wenckebach (Mobitz Type I), coupled extrasystoles (bigeminy)
- Irregularly irregular: Atrial fibrillation (the single most common cause), multiple ectopics
Pulse deficit: In atrial fibrillation, the apical rate exceeds the peripheral rate because some beats are too weak to be transmitted peripherally. Always compare apex beat with radial pulse simultaneously.
7. Normal Arterial Pulse Waveform
The arterial pulse waveform has:
- Anacrotic limb (upstroke): Rapid rise in pressure during ventricular ejection
- Systolic peak
- Dicrotic notch: Caused by closure of the aortic valve; separates systole from diastole
- Dicrotic limb (downstroke): Passive fall during diastole
The character and contour of the pulse depend on:
- Stroke volume
- Ejection velocity
- Vascular compliance
- Systemic vascular resistance
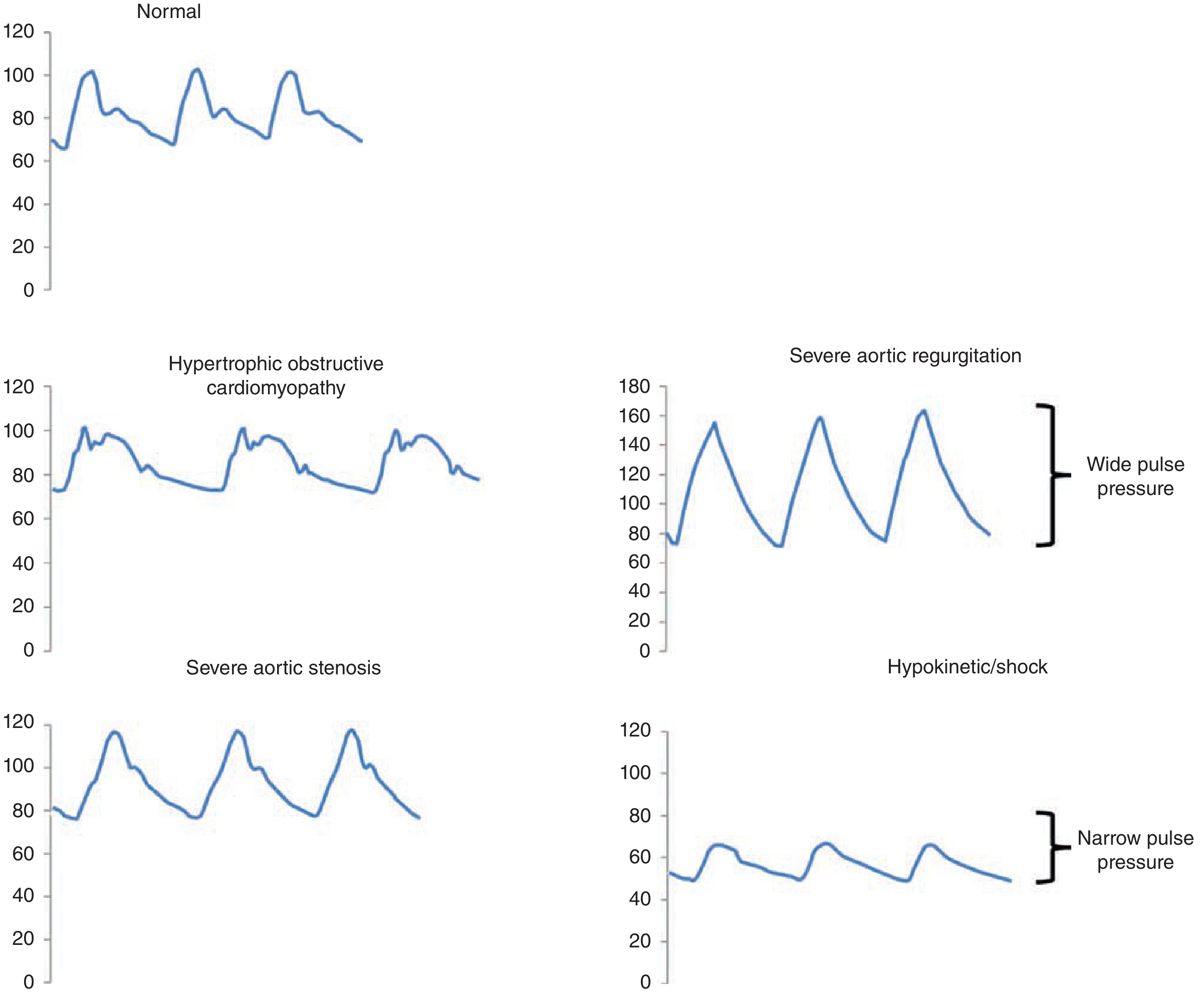
Fig. Normal arterial pulse waveform (top left) vs. Hypertrophic obstructive cardiomyopathy (middle left), Severe aortic stenosis (bottom left), Severe aortic regurgitation (top right - wide pulse pressure and collapsing), Hypokinetic/shock (bottom right - narrow pulse pressure). - Fuster and Hurst's The Heart, 15th Ed.
8. Abnormal Pulse Characters
8.1 Pulsus Parvus et Tardus ("Slow-rising, Low Amplitude")
- Small (parvus) and late-peaking (tardus) pulse
- Slurred upstroke, delayed peak, reduced amplitude
- Classic lesion: Severe Aortic Stenosis
- Also seen in: subvalvular/supravalvular aortic stenosis, fixed LV outflow obstruction
- On Doppler: mirrors the delayed contour as prolonged systolic ejection time
8.2 Water Hammer Pulse (Corrigan's Pulse / Collapsing Pulse)
- Bounding pulse with sharp rise and rapid collapse
- Due to: increased stroke volume + wide pulse pressure (high systolic, low diastolic)
- Classic lesion: Severe Aortic Regurgitation
- Also seen in: thyrotoxicosis, patent ductus arteriosus, AV fistulae, severe anaemia
- Clinical test: Raise the arm above the head while palpating the radial pulse - the collapsing quality becomes more apparent
8.3 Bisferiens Pulse ("Two Peaks in Systole")
- Two systolic peaks palpable in a single cardiac cycle
- Seen in:
- Severe aortic regurgitation (often with mixed aortic valve disease)
- Hypertrophic obstructive cardiomyopathy (HOCM) - spike-and-dome pattern: rapid first peak (percussion wave from initial unobstructed ejection), then a second tidal wave after mid-systolic obstruction sets in
- Patients on intra-aortic balloon counterpulsation (IABP) - second pulse is diastolic
8.4 Anacrotic Pulse
- Notch or shoulder felt on the ascending limb of the pulse (anacrotic notch)
- Seen in severe aortic stenosis
- The upstroke is slow and interrupted
8.5 Dicrotic Pulse
- Exaggeration of the dicrotic notch, palpable as a second wave on the descending limb
- Seen in: septic shock, severe peripheral vasoconstriction, hypovolemic shock, cardiac tamponade
- Usually associated with hypotension and narrow pulse pressure
8.6 Pulsus Alternans
- Beat-to-beat alternation in pulse amplitude (one strong, one weak) in a regular rhythm, independent of respiration
- Mechanism: cyclic changes in intracellular calcium and action potential duration
- Classic lesion: Severe LV systolic dysfunction (also aortic stenosis)
- An ominous sign - suggests very profound ventricular systolic dysfunction
- May be associated with T-wave alternans on ECG, which increases arrhythmic risk
- Different from pulsus paradoxus - variations are NOT respirophasic
8.7 Pulsus Paradoxus
- Fall in systolic BP >10 mmHg during inspiration
- A misnomer - a small drop (<10 mmHg) with inspiration is actually normal
- Mechanism: Exaggerated interventricular dependence during inspiration
- Classic lesion: Cardiac tamponade
- Also seen in: Constrictive pericarditis, massive pulmonary embolism, severe obstructive lung disease (asthma/COPD), tension pneumothorax, hemorrhagic shock
- Measurement: Inflate BP cuff above systolic pressure. Deflate slowly. Note the pressure at which Korotkoff sounds first appear (expiration only) and the pressure at which they are heard with every beat. Difference >10 mmHg = paradoxus. Deflation must be slow.
- Pulsus paradoxus may be palpable at the brachial or femoral artery when >15 mmHg
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025); Fuster and Hurst's The Heart, 15th Ed.
9. Pulse Waveform Diagrams (Carotid)
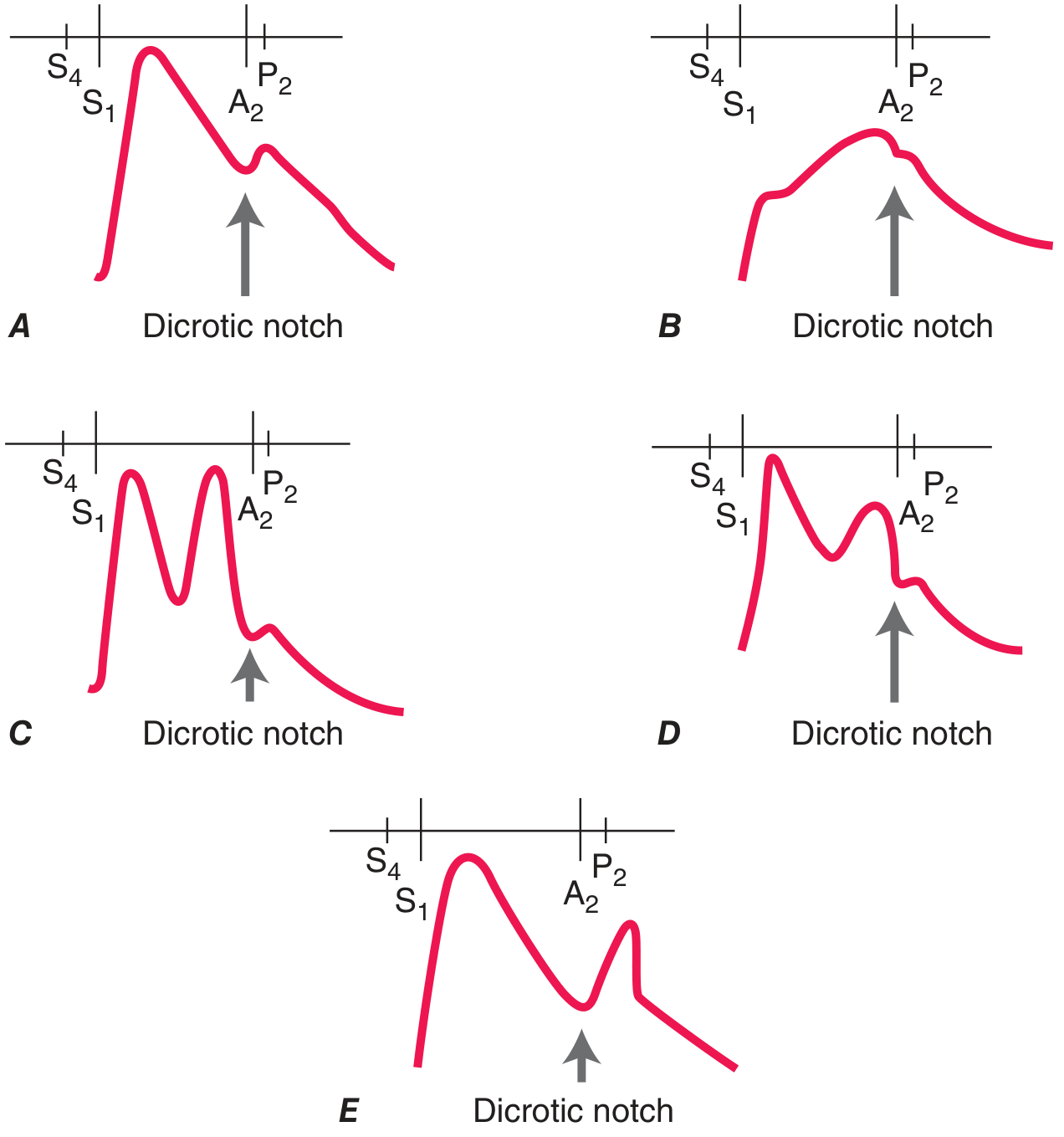
A: Normal (with dicrotic notch) | B: Aortic Stenosis - slow upstroke, reduced peak (parvus et tardus) | C: Bisferiens pulse - two systolic peaks in severe AR | D: Bisferiens pulse in HOCM (spike-and-dome) | E: Dicrotic pulse - exaggerated dicrotic wave
10. Pulse Volume and Amplitude
Pulse amplitude is an indirect measure of cardiac output - it is proportional to stroke volume.
| Amplitude | Possible Causes |
|---|---|
| Low amplitude (no AS) | Reduced cardiac output: severe LV dysfunction, severe mitral stenosis, constrictive pericarditis |
| Bounding / High amplitude | Aortic regurgitation, thyrotoxicosis, anaemia, fever, PDA, AV fistulae, high output states |
| In shock | Decreased amplitude + hyperdynamic (tachycardia) |
- Fuster and Hurst's The Heart, 15th Ed.
11. Jugular Venous Pulse (JVP)
The JVP reflects right atrial pressure and right heart hemodynamics. It is distinct from the arterial pulse.
Differentiating JVP from Carotid Pulse
| Feature | JVP (Venous) | Carotid (Arterial) |
|---|---|---|
| Palpability | Not palpable | Palpable |
| Compression | Disappears with light proximal pressure | Cannot be compressed |
| Number of waveforms | Two upstrokes (a and v) | Single upstroke |
| Response to respiration | Becomes more prominent on inspiration | No change |
| Response to posture | Falls on sitting up | Unchanged |
Normal JVP Waveform: a, c, v Waves; x, y Descents
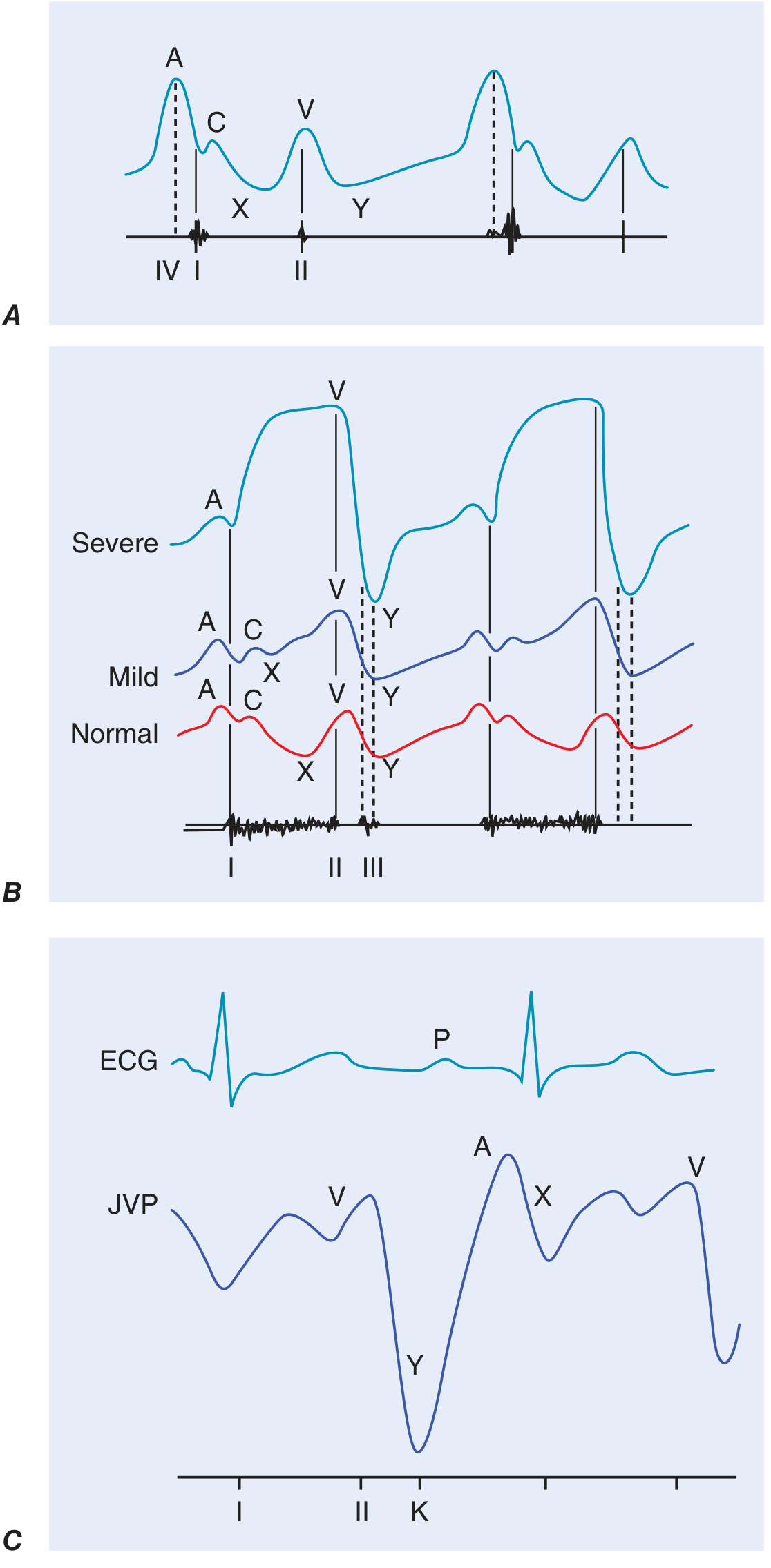
Fig. A: Normal JVP with a, c, v waves and x, y descents. B: JVP in tricuspid regurgitation (giant v wave with loss of x descent). C: JVP in constrictive pericarditis (prominent y descent - Friedreich's sign)
| Component | Origin | Timing |
|---|---|---|
| a wave | Right atrial contraction | Pre-systolic (after P wave on ECG) |
| c wave | Tricuspid valve closure + carotid pulsation artifact | Early systole (after QRS) |
| x descent | Atrial relaxation + descent of tricuspid valve toward apex | Systole |
| v wave | Passive venous filling of right atrium (atrial diastole) | Late systole |
| y descent | Tricuspid valve opening → blood empties into RV | Early diastole |
JVP Abnormalities
Giant a wave: Right atrial contraction against resistance
- Tricuspid stenosis, pulmonary hypertension, pulmonary stenosis, right ventricular hypertrophy
Cannon a wave: RA contracts against closed tricuspid valve
- Complete heart block (irregular cannon waves), nodal/ventricular tachycardia, ventricular ectopics
Absent a wave: No effective atrial contraction
- Atrial fibrillation
Giant v wave / CV wave: Tricuspid regurgitation (TR)
- Regurgitant flow back into RA during systole; in severe TR, merges with a wave
Prominent x descent: Cardiac tamponade (x descent preserved/prominent, y descent blunted or absent)
Prominent y descent: Constrictive pericarditis (rapid early ventricular filling) - "Friedreich's sign"
- Also: severe TR (rapid ventricular filling after large v wave)
Kussmaul's sign: Paradoxical rise in JVP on inspiration
- Normal: JVP falls on inspiration (increased venous return is accommodated)
- Kussmaul's sign: JVP rises on inspiration - seen in constrictive pericarditis, restrictive cardiomyopathy (and can be seen in RV infarction)
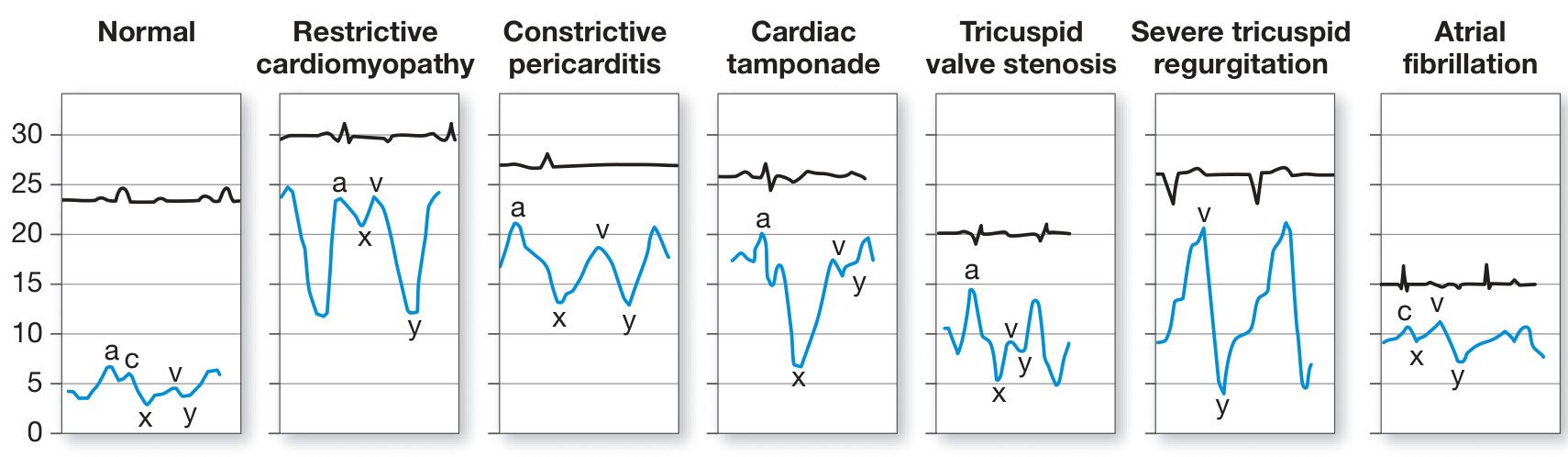
Fig. JVP waveforms: Normal | Restrictive cardiomyopathy | Constrictive pericarditis | Cardiac tamponade | Tricuspid stenosis | Severe tricuspid regurgitation | Atrial fibrillation. - Fuster and Hurst's The Heart, 15th Ed.
12. Estimation of JVP / CVP
Landmark: The angle of Louis (manubriosternal junction) lies 5 cm above the mid-right atrium, regardless of body position.
Measurement:
CVP (cm H₂O) = Vertical height of JVP pulsation above the angle of Louis + 5 cm
Normal: <3 cm above the angle of Louis at 45° (i.e., total CVP <8 cm H₂O)
Rapid bedside estimation at 90° (sitting):
- No visible pulsation = CVP < 8 cm H₂O (normal)
- Pulsation at clavicle = ~10 cm H₂O
- Mid-neck = ~15 cm H₂O
- Angle of jaw = ~20 cm H₂O
Important caveats:
- In very high CVP (constrictive pericarditis), the pulsation may not be visible until patient is standing
- In very low CVP, patient may need to be almost supine before pulsations appear
- Hepatojugular reflux: Sustained pressure on the liver for 10-15 seconds causes a transient rise in JVP >4 cm - suggests elevated central venous pressure or right heart failure
- Fuster and Hurst's The Heart, 15th Ed.
13. Special Pulse Patterns - Summary Table
| Pulse | Description | Classic Cause |
|---|---|---|
| Pulsus parvus et tardus | Small + slow-rising | Severe aortic stenosis |
| Water hammer (Corrigan's) | Bounding, collapsing | Severe aortic regurgitation |
| Bisferiens | Two systolic peaks | AR + AS mixed, HOCM |
| Anacrotic | Shoulder on upstroke | Severe aortic stenosis |
| Dicrotic | Exaggerated dicrotic notch | Septic/hypovolemic shock |
| Pulsus alternans | Alternating amplitude, regular | Severe LV systolic dysfunction |
| Pulsus paradoxus | Inspiratory drop >10 mmHg systolic | Cardiac tamponade |
| Pulsus bigeminus | Alternating strong-weak beats, irregular | Bigeminal ectopics |
| Jerky pulse | Rapid rise | HOCM (dynamic obstruction) |
14. Clinical Correlations
Coarctation of the aorta: Radio-femoral delay - femoral pulse arrives later than the radial pulse (normally they are simultaneous). Upper limb hypertension + absent/delayed lower limb pulses.
Peripheral Arterial Disease: Absent or diminished pedal pulses, rest pain, claudication. Level of absent pulse localizes the obstruction.
Cardiac Tamponade: Tachycardia + pulsus paradoxus + elevated JVP with preserved x descent and blunted y descent (Beck's triad: hypotension, muffled heart sounds, elevated JVP).
Constrictive Pericarditis vs. Tamponade:
- Both: elevated JVP, pulsus paradoxus (tamponade > constrictive)
- Constrictive: prominent y descent + Kussmaul's sign; Tamponade: absent y descent, preserved x descent
Aortic Regurgitation (Corrigan's pulse): Multiple peripheral signs result from the wide pulse pressure - visible carotid pulsations (Corrigan's sign), pistol-shot femorals (Traube's sign), capillary pulsations in nailbed (Quincke's sign), head bobbing (de Musset's sign).
15. Key Points for Examinations
- The pulse rate, rhythm, volume, character, and condition of the vessel wall must all be systematically assessed
- Carotid pulse gives the best information about contour (character)
- Pulsus paradoxus is measured with a BP cuff - a difference >10 mmHg between expiratory and all-cycle systolic is pathological
- Pulsus alternans = regular rhythm + alternating amplitude = severe LV dysfunction
- JVP is measured from the angle of Louis + 5 cm (total CVP)
- Kussmaul's sign (JVP rises on inspiration) = constrictive pericarditis / restrictive cardiomyopathy
- A prominent y descent favours constriction; absent y descent with prominent x favours tamponade
- Bisferiens pulse - two systolic peaks - seen in HOCM (spike and dome) and severe AR
Sources:
- Fuster and Hurst's The Heart, 15th Edition - Physical Examination: Arterial and Venous Pulse
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Cardiovascular Examination
- S Das, A Manual on Clinical Surgery, 13th Edition - Physical Examination
- Goldman-Cecil Medicine, International Edition - Auscultation and Jugular Veins
- Miller's Anesthesia, 10th Edition - Arterial Pulse Waveform Analysis
This is a shared conversation. Sign in to Orris to start your own chat.