Thymoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
thymoma classification management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Here is a complete overview:
Thymoma
Definition
Thymoma is a tumor of thymic epithelial cells and accounts for 80-85% of all thymic neoplasms. By convention, the term "thymoma" is restricted to epithelial-cell tumors; other thymic neoplasms (germ cell tumors, lymphomas, carcinoids) are classified separately. Thymomas are the most common neoplasm of the anterosuperior mediastinum in adults and are generally considered malignant tumors even when appearing histologically bland.
- Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
Epidemiology
- Peak incidence: third to fifth decades of life (median age ~54 years)
- Males and females affected equally
- Rare in children
- Arise predominantly in the anterior-superior mediastinum; rarely in neck, thyroid, pulmonary hilum, or posterior mediastinum
Classification
WHO Histologic Classification (most widely used clinically)
| Type | Epithelial Cell Morphology | Lymphocyte Content | Behavior |
|---|---|---|---|
| A | Spindle/oval (medullary type) | Sparse | Most indolent |
| AB | Mixed medullary + cortical | Mixed | Indolent |
| B1 | Predominantly cortical | Abundant lymphocytes | Low-grade |
| B2 | Cortical | Moderate | Intermediate |
| B3 | Polygonal, epithelial-rich | Few lymphocytes | Most aggressive thymoma |
| Thymic carcinoma | Overtly malignant cytology | Variable | Most aggressive (separate category) |
A simpler clinically practical classification divides thymomas into three types:
- Cytologically benign and noninvasive (encapsulated)
- Cytologically benign but invasive or metastatic
- Cytologically malignant (thymic carcinoma)
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Sabiston Textbook of Surgery
Histopathology
Macroscopy: Lobulated, firm, gray-white masses up to 15-20 cm. May show cystic necrosis and calcification. Most are encapsulated; 20-25% penetrate the capsule.
Microscopy:
- Noninvasive thymomas: medullary-type epithelial cells (elongated/spindle-shaped) with sparse thymocytes
- Mixed type: polygonal cortical epithelial cells + dense thymocyte infiltrate
- Invasive thymomas: histologically may look identical to benign forms - invasion is the key malignant feature
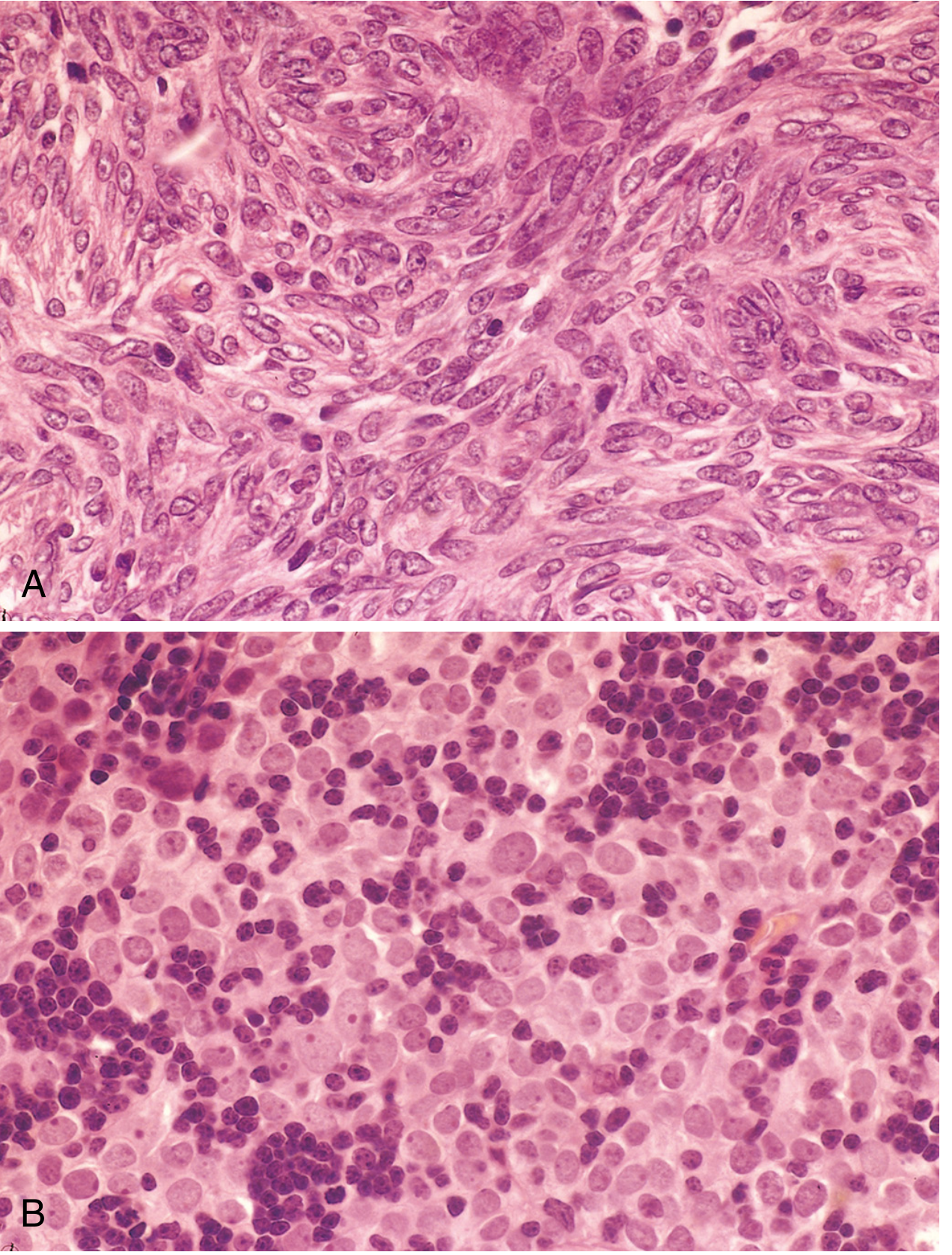
Fig. 13.43 - Thymoma histology. (A) Benign (medullary type): bland spindle/oval epithelial cells in a swirling pattern, few lymphocytes. (B) Malignant thymoma: polygonal epithelial cells with round/oval nuclei, numerous immature T-cell thymocytes interspersed - this tumor was locally invasive into lung and pericardium.
AJCC TNM Staging (8th Edition)
| Stage | Definition |
|---|---|
| T1a | Encapsulated or unencapsulated, with/without extension into mediastinal fat |
| T1b | Extension into mediastinal pleura |
| T2 | Pericardium involvement |
| T3 | Lung, brachiocephalic vein, SVC, chest wall, phrenic nerve, or hilar pulmonary vessels |
| T4 | Aorta, arch vessels, main pulmonary artery, myocardium, trachea, or esophagus |
| N0 | No nodal involvement |
| N1 | Anterior (perithymic) nodes |
| N2 | Deep intrathoracic or cervical nodes |
| M0 | No distant metastasis |
| M1a | Separate pleural or pericardial nodule(s) |
| M1b | Pulmonary intraparenchymal nodule or distant organ metastasis |
This replaced the older Masaoka-Koga staging system as the standard with AJCC 8th edition.
- Sabiston Textbook of Surgery
Clinical Features
About one-third of patients are asymptomatic (incidental discovery). One-third have local symptoms from compression/invasion:
- Cough, dyspnea, chest pain
- Superior vena cava syndrome
- Hemoptysis
The remaining patients present with paraneoplastic/systemic syndromes due to immunologic mechanisms.
Associated Paraneoplastic Syndromes
| Syndrome | Frequency |
|---|---|
| Myasthenia gravis (MG) | 40-50% of thymoma patients |
| Pure red cell aplasia | Less common |
| Hypogammaglobulinemia (Good syndrome) | Less common |
| Systemic lupus erythematosus | Rare |
| Thymoma-associated multiorgan autoimmunity | Rare |
Conversely, only 5-15% of MG patients have a thymoma. Importantly, AChR antibodies are present in ~60% of thymoma patients even without neurologic symptoms - hence all thymoma patients should have preoperative AChR-Ab testing.
Diagnosis
- CT scan is the primary imaging modality: well-circumscribed, solid anterior mediastinal mass
- Features suggesting thymoma: solid mass without low-density areas of fat/cysts (which would suggest teratoma)
- MRI: more sensitive than CT for mediastinal invasion when CT is equivocal
- Fat plane obliteration on imaging suggests mediastinal invasion; pleural thickening/nodularity/effusion indicates pleural invasion
- FDG-PET: SUVmax >12.85 strongly suggests lymphoma rather than thymoma
- Biopsy is usually not necessary for small, typical-appearing resectable masses - proceed directly to surgery
- Biopsy is needed when the tumor is unresectable, lymphoma is strongly suspected, or neoadjuvant therapy is planned (core needle biopsy: ~60% success; surgical biopsy: ~90% success)
- AChR antibody levels - diagnostic of MG and strongly supports thymoma
Treatment
Surgery
- Complete surgical resection is the cornerstone of treatment for all resectable thymomas
- Thymectomy must include the entire thymus gland plus all accessible mediastinal fatty-areolar tissue (to remove ectopic thymic tissue and reduce recurrence)
- Phrenic nerve preservation is integral
- For MG patients: surgery when weakness is adequately controlled; use anticholinesterase inhibitors, plasmapheresis, or IVIG perioperatively
For Invasive/Advanced Disease
- Neoadjuvant chemotherapy + radiation followed by surgery for potentially resectable invasive tumors
- Resection/reconstruction of involved structures (SVC, innominate vein) can prolong survival in selected patients
- Resection of "droplet" pleural metastases may also be beneficial
Adjuvant Therapy
- Adjuvant radiation: sometimes used after complete resection for stage II and higher (data conflicting)
- For stage III or IV: combined chemotherapy and radiotherapy
Unresectable Disease
- Chemotherapy and/or radiotherapy as primary treatment
Key Points Summary (Grainger & Allison's Diagnostic Radiology)
- Most common thymic tumor in adults
- Usually benign or low-grade malignant thymic epithelial tumors
- Average age of diagnosis: 50 years
- Myasthenia gravis in up to 50%
- Capsular absence or extension = invasive nature
- Complete obliteration of adjacent fat planes = mediastinal invasion
- MRI superior to CT when invasion is equivocal
Sources
This is a shared conversation. Sign in to Orris to start your own chat.