Explain explain hyponatremia pathophysiology of hyponatremia as well as hypervolemic hypo natremia and hypovolemic hyponatremia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from Harrison's 22E, Goldman-Cecil, and Brenner & Rector. I have enough to construct a thorough, well-cited answer. Let me compile everything.
Hyponatremia: Pathophysiology, Hypervolemic, and Hypovolemic Forms
Definition
Hyponatremia is defined as a plasma sodium (Na+) concentration <135 mM (mmol/L). It is the most common electrolyte disorder in hospitalized patients, occurring in up to 22% of inpatients. - Harrison's Principles of Internal Medicine 22E
General Pathophysiology
The Core Concept: Water Excess Relative to Sodium
Hyponatremia is almost never simply "too little sodium" - it is almost always too much water relative to sodium. The serum Na+ concentration reflects the ratio of total body solute to total body water. When water accumulates in excess of sodium, the ratio falls and hyponatremia results.
The two physiological "effectors" that govern serum osmolality are:
- Arginine Vasopressin (AVP) - the primary antidiuretic hormone (also called ADH)
- Thirst - which drives water intake
Defects in one or both of these defense mechanisms cause most cases of hyponatremia. - Harrison's 22E
The Role of AVP (ADH) - Central Mechanism
Hyponatremia is almost always the result of:
- Increased circulating AVP and/or
- Increased renal sensitivity to AVP
- ...combined with free water intake
AVP acts on renal V2 receptors in the collecting duct, inserting aquaporin-2 (AQP2) water channels, driving water reabsorption from the tubular lumen into the medullary interstitium. The result is concentrated urine and dilutional hyponatremia as body water expands.
Two Mechanisms Causing Impaired Water Excretion
According to Brenner & Rector's The Kidney, chronic hyponatremia due to defective renal water excretion has two root causes:
- Low distal delivery of filtrate to the diluting segment of the nephron
- Occurs when GFR is reduced or fractional NaCl reabsorption in the proximal tubule (PT) is increased
- Increased PT reabsorption is driven by a decreased Effective Arterial Blood Volume (EABV)
- Actions of vasopressin on the inner medullary collecting duct (via renal water pores, RWP)
- AVP drives water reabsorption along the osmotic gradient created by the hypertonic medullary interstitium
Key teaching point: Decreased EABV can result from an actual total-body NaCl deficit (true hypovolemia) OR from a low cardiac output / splanchnic vasodilation state (as in heart failure or cirrhosis) - in both cases, the kidney "perceives" underfilling and responds accordingly. - Brenner & Rector's The Kidney
Brain Adaptation and Risk of Osmotic Demyelination
This understanding is critical for management:
- Acute hyponatremia (<48 hours): Brain cells swell due to osmotic water influx - causing cerebral edema, headache, seizures, coma, and potentially death
- Chronic hyponatremia (>48 hours): Brain cells adapt by exporting effective osmoles - mainly K+ (and accompanying anions) and organic solutes (taurine, myoinositol). This returns brain cell volume toward normal
- Risk of rapid correction: If Na+ is corrected too rapidly in chronic hyponatremia, cerebral vascular endothelial cells shrink, the blood-brain barrier opens, lymphocytes/complement/cytokines enter the brain, oligodendrocytes are damaged, and osmotic demyelination syndrome (ODS) results - Brenner & Rector's The Kidney
Classification by Volume Status
The underlying pathophysiology of the AVP response differs by ECFV (extracellular fluid volume). Hyponatremia is therefore classified into three groups:
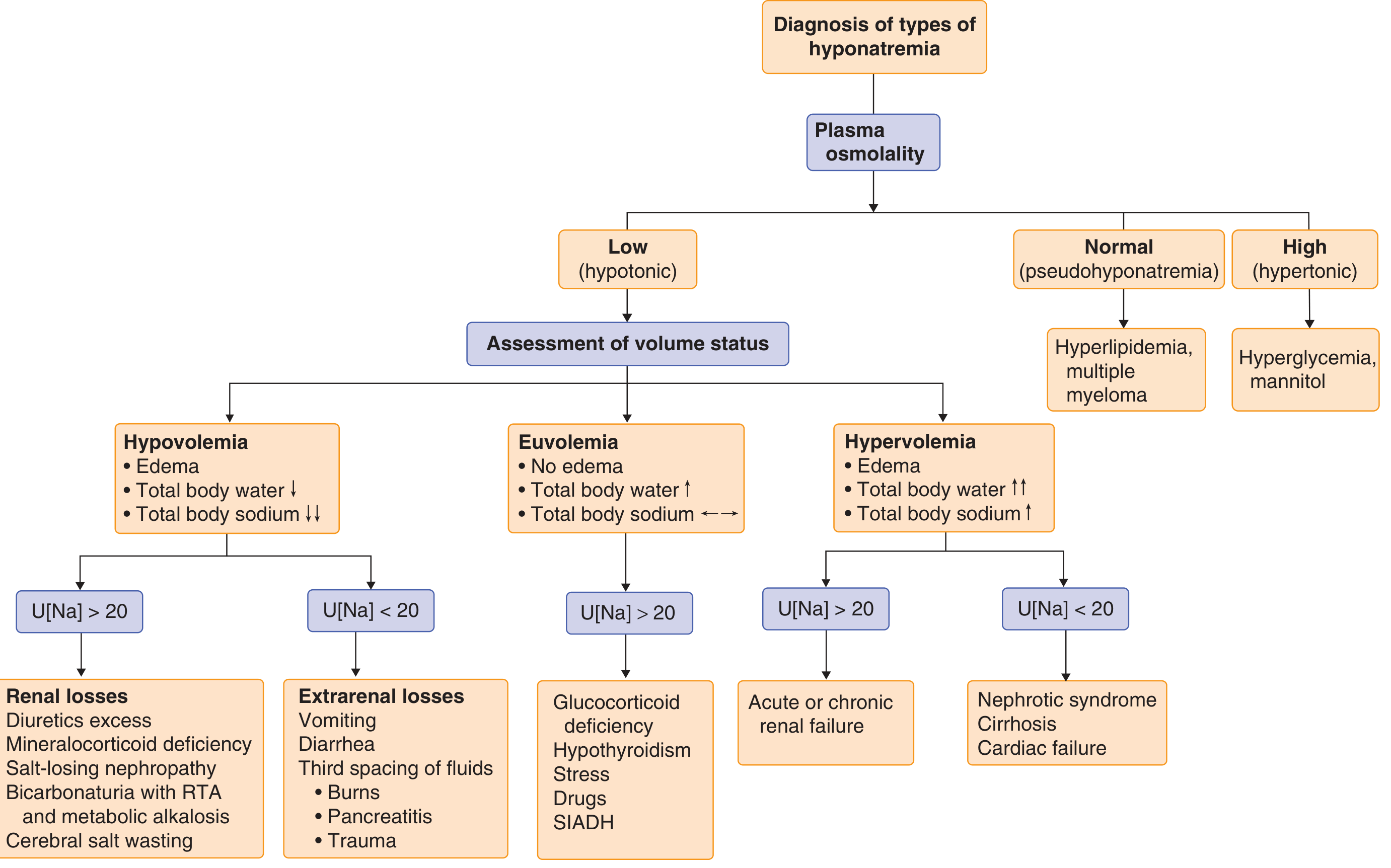
Diagnostic approach to hyponatremia. From Goldman-Cecil Medicine
Hypovolemic Hyponatremia
Pathophysiological Mechanism
In hypovolemic hyponatremia, there is true total-body sodium deficit (Na+ loss greater than water loss), leading to:
- Volume depletion triggers baroreceptor activation
- Non-osmotic (volume-mediated) AVP release from the posterior pituitary - this is a "non-osmotic" AVP stimulus, where the body sacrifices osmolality to preserve volume
- Thirst activation drives the patient to drink water (often hypotonic)
- Renal water retention via V2 receptor activation
- Net result: water is retained but sodium is not replaced at the same rate - Na+ concentration falls
"Hypovolemia causes a marked neurohumoral activation, increasing circulating levels of AVP. The increase in circulating AVP helps preserve blood pressure via vascular and baroreceptor V1A receptors and increases water reabsorption via renal V2 receptors; activation of V2 receptors can lead to hyponatremia in the setting of increased free water intake." - Harrison's 22E
Causes
Extrarenal losses (Urine Na+ typically <20 mM):
- Gastrointestinal losses: vomiting, diarrhea, tube drainage (secretory diarrhea is Na+-rich)
- Insensible losses: sweating (especially when replaced with plain water), burns
- Third spacing: ascites, pancreatitis, trauma, ileus
Renal losses (Urine Na+ typically >20 mM):
- Thiazide diuretics - block NaCl cotransporter in cortical diluting segment; impair urinary dilution; lead to polydipsia; this is the most common pharmacological cause
- Mineralocorticoid deficiency (Addison's disease / primary adrenal insufficiency) - lack of aldosterone causes inappropriate urinary Na+ wasting; suspect when hyperkalemia + hyponatremia + hypotension coexist with high urine Na+
- Salt-losing nephropathies - reflux nephropathy, interstitial nephritis, post-obstructive uropathy, medullary cystic disease, ATN recovery phase
- Cerebral salt wasting (CSW) - rare, associated with subarachnoid hemorrhage, TBI, craniotomy, encephalitis; characterized by inappropriate renal Na+ wasting + clinical hypovolemia (distinguish from SIADH, which is euvolemic)
Key Laboratory Findings
| Parameter | Extrarenal Losses | Renal Losses |
|---|---|---|
| Urine Na+ | <20 mM | >20 mM |
| Volume status | Hypovolemic (may look euvolemic) | Hypovolemic |
| Response to normal saline | Rapid Na+ correction (AVP suppressed) | Variable |
| BUN/Creatinine | Elevated (prerenal) | Variable |
A urine Na+ <20 mM (in the absence of hypervolemic causes) predicts a rapid rise in plasma Na+ in response to IV normal saline, as saline infusion suppresses AVP, inducing a water diuresis. - Harrison's 22E
Special note on Thiazides
Thiazides are unique in that they:
- Block NaCl reabsorption in the cortical diluting segment (not the medullary concentrating mechanism)
- Therefore, the kidney loses its ability to dilute urine but retains its ability to concentrate urine
- Any hypotonic fluid ingested is retained while salt is lost - leading to hyponatremia
- Can mimic SIADH clinically; presentations can be indistinguishable without careful history - Goldman-Cecil Medicine
Hypervolemic Hyponatremia
Pathophysiological Mechanism
In hypervolemic hyponatremia, there is total-body excess of both Na+ AND water, but water excess is proportionately greater. The paradox is that despite whole-body sodium excess (visible as edema), the kidneys are avidly retaining sodium and water. Why? Because the effective arterial blood volume (EABV) is reduced, even though total body fluid is expanded.
The mechanism mirrors hypovolemic hyponatremia in its final common pathway - decreased EABV triggers the same neurohumoral cascade - but the reason for the reduced EABV is different:
"The pathophysiology of hyponatremia in the sodium-avid edematous disorders (congestive heart failure [CHF], cirrhosis, and nephrotic syndrome) is similar to that in hypovolemic hyponatremia, except that arterial filling and circulatory integrity is decreased due to the specific etiologic factors (e.g., cardiac dysfunction in CHF, peripheral vasodilation in cirrhosis)." - Harrison's 22E
The Common Neurohumoral Cascade
Regardless of the specific etiology, the same pathway is activated:
Reduced EABV →
- Baroreceptor activation (carotid sinus, aortic arch, renal afferent arterioles)
- ↑ Renin-Angiotensin-Aldosterone System (RAAS) → Na+ retention → edema worsens
- ↑ Sympathetic nervous system activation → renal vasoconstriction, ↓ GFR
- ↑ Non-osmotic AVP release → V2 receptor activation → water retention > Na+ retention
- ↑ Thirst → increased water intake
- Net: Na+ is retained but water is retained even more → plasma Na+ falls → hyponatremia
Causes and Specific Mechanisms
1. Congestive Heart Failure (CHF)
- Reduced cardiac output → reduced stroke volume → arterial underfilling
- Despite high total body Na+ and water (edema, pleural effusions), arterial baroreceptors "sense" inadequate filling
- The degree of hyponatremia in CHF reflects the degree of neurohumoral activation and is an independent prognostic indicator for mortality
2. Cirrhosis
- Splanchnic vasodilation (due to nitric oxide and other vasodilators released by the diseased liver) causes arterial underfilling
- Portal hypertension promotes fluid shift into peritoneal space (ascites)
- Both mechanisms reduce EABV → same neurohumoral cascade as in CHF
- Hyponatremia in cirrhosis is a sign of advanced disease and carries poor prognosis
3. Nephrotic Syndrome
- Massive urinary protein loss → hypoalbuminemia → reduced plasma oncotic pressure → fluid shifts from intravascular to interstitial space
- Intravascular volume depletion → decreased EABV → AVP release, RAAS activation
- "Underfill theory" of nephrotic edema
4. Advanced Renal Failure (Acute or Chronic)
- Unique among hypervolemic causes: urine Na+ is >20 mM (kidney cannot conserve Na+ due to tubular damage)
- Hyponatremia results from the kidney's inability to excrete the water load (loss of diluting ability)
- Total solute excretion is impaired
Key Laboratory Findings
| Parameter | CHF / Cirrhosis / Nephrotic | Renal Failure |
|---|---|---|
| Urine Na+ | <10 mM (very avid Na+ retention) | >20 mM |
| Edema | Present | Present |
| RAAS | Markedly activated | Variable |
| BNP (CHF) | Elevated | Variable |
"Urine Na+ concentration is typically very low, i.e., <10 mM, even after hydration with normal saline; this Na+-avid state may be obscured by diuretic therapy. The degree of hyponatremia provides an indirect index of the associated neurohumoral activation and is an important prognostic indicator in hypervolemic hyponatremia." - Harrison's 22E
Summary Comparison Table
| Feature | Hypovolemic | Hypervolemic |
|---|---|---|
| Total body Na+ | Decreased | Increased |
| Total body water | Decreased (less than Na+) | Markedly increased |
| EABV | Truly decreased | Functionally decreased |
| AVP stimulus | True volume depletion | Arterial underfilling |
| Urine Na+ (extrarenal) | <20 mM | <10 mM |
| Urine Na+ (renal cause) | >20 mM | >20 mM (renal failure) |
| Edema | Absent | Present |
| Causes | GI losses, diuretics, adrenal insufficiency, CSW, burns | CHF, cirrhosis, nephrotic syndrome, renal failure |
| RAAS | Activated | Activated |
| Treatment goal | Volume resuscitation + correct cause | Free water restriction + treat underlying disease |
Sources
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 56 - Fluid and Electrolyte Disorders
- Goldman-Cecil Medicine, Chapter 102 - Disorders of Sodium and Water Homeostasis
- Brenner and Rector's The Kidney, 2-Volume Set, Concepts 9 and 10 - Hyponatremia
This is a shared conversation. Sign in to Orris to start your own chat.