Dexmedetomidine in MD
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
dexmedetomidine muscular dystrophy
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent — I now have comprehensive data. Let me compile the full answer.
Dexmedetomidine — Comprehensive Overview
(Interpreted as general clinical pharmacology + use in Monitored Anesthesia Care / MAC, ICU, and perioperative medicine. The sole PubMed hit on "muscular dystrophy" was a single case report [PMID 38855294], confirming there is no disease-specific evidence base — so this covers the complete drug profile relevant to any MD context.)
1. Mechanism of Action
Dexmedetomidine is a highly selective α₂-adrenoceptor agonist — the active S-enantiomer of medetomidine. Its selectivity ratio for α₂:α₁ receptors is approximately 1600:1, far exceeding clonidine.
- Sedation/hypnosis: via α₂ receptors in the locus coeruleus → activates endogenous sleep pathways, producing a state resembling physiologic NREM sleep
- Analgesia: via α₂ receptors at the spinal cord level (dorsal horn)
- Sympatholysis: reduces central noradrenergic outflow → decreased heart rate, BP, and plasma catecholamines
- Its effects are reversible with α₂-antagonists (e.g., atipamezole)
— Katzung's Basic and Clinical Pharmacology, 16th ed. | Miller's Anesthesia, 10th ed.
2. Pharmacokinetics
| Parameter | Value |
|---|---|
| Protein binding | ~94% (albumin + α₁-acid glycoprotein) |
| Metabolism | Hepatic — N-methylation, hydroxylation → conjugation |
| Excretion | Urine (95%), bile |
| Clearance | High |
| Elimination half-life | ~2 hours |
| Context-sensitive half-time | 4 min (after 10-min infusion) → 250 min (after 8-hour infusion) |
Renal impairment: Less protein binding → prolonged sedative effect. Hepatic impairment reduces clearance significantly.
— Katzung, 16th ed. | Barash Clinical Anesthesia, 9th ed.
3. Organ System Effects
CNS
- Sedation resembling natural sleep — patients are arousable and cooperative
- Anxiolysis, mild analgesia
- Minimal amnesia (vs. benzodiazepines)
- ↓ cerebral blood flow (CBF ~25%), without significant change in ICP or CMRO₂
- Potential for tolerance and dependence with prolonged use
- Anti-shivering properties (via α₂ activation in thermoregulatory center)
Cardiovascular
- Loading bolus: transient ↑ BP (peripheral α₂ vasoconstriction) → followed by ↓ HR (reflex + central vagal predominance)
- Infusion: ↓ HR, ↓ SVR, ↓ BP (moderate)
- Risk of severe bradycardia, heart block, sinus arrest — especially when combined with sympatholytic or vagotonic agents (e.g., neostigmine, β-blockers, digoxin)
- Response to atropine/anticholinergics is preserved
Respiratory
- Minimal respiratory depression — ventilatory response to CO₂ unchanged
- Small ↓ tidal volume, essentially no change in RR
- Upper airway obstruction can occur with deep sedation
- Preserves spontaneous respiration even at high doses (key advantage)
- Synergistic sedation when combined with other sedative-hypnotics
— Katzung, 16th ed. | Goldman-Cecil Medicine | Barash, 9th ed.
4. Clinical Uses
ICU Sedation (Primary Indication)
- First-line for short-term sedation of intubated/ventilated ICU patients
- Advantages over benzodiazepines:
- ↓ duration of mechanical ventilation
- ↑ patient comfort
- ↓ incidence and duration of perioperative delirium
- More cooperative behavior ("cooperative sedation")
Monitored Anesthesia Care (MAC) / Procedural Sedation
- Useful for awake fiberoptic intubation — cooperative, comfortable patient + dry mouth effect
- Painful procedures — analgesic properties supplement sedation
- Lower legislative restrictions vs. propofol in some jurisdictions
Comparison with Propofol in MAC:
| Feature | Propofol | Dexmedetomidine |
|---|---|---|
| Pain on injection | Yes | Minimal |
| Analgesia (subhypnotic) | Minimal | Yes |
| Amnesia (subhypnotic) | Significant | Insignificant |
| Onset | Rapid | 5–10 min |
| Bradycardia risk | Minimal | Significant |
| Non-anesthesiologist use restrictions | Yes | No |
| Recovery time | Shorter | Potentially longer (2h t½) |
— Barash, 9th ed.
Adjunct to General Anesthesia
- Reduces requirements for inhaled and IV anesthetics
- Dose: 0.5–1 mcg/kg loading over 10–15 min → infusion 0.2–0.7 mcg/kg/h
- Preoperative dexmedetomidine reduces fentanyl consumption in abdominal, cholecystectomy, and intraocular surgery
- Smooth emergence; sedative + analgesic effects persist into PACU without respiratory depression
Pediatrics (off-label)
- Intranasal dexmedetomidine 1 mcg/kg — preoperative anxiolysis
- ICU sedation in children
- Arousability preserved; sedation resembles natural sleep
— Barash, 9th ed. | Miller's, 10th ed.
Regional Anesthesia Adjunct
- Perineural injection as adjunct to brachial plexus block — may extend duration (evidence limited, not statistically significant in all studies)
5. Dosing
| Indication | Loading Dose | Maintenance Infusion |
|---|---|---|
| ICU sedation (intubated) | 1 mcg/kg over 10 min (optional) | 0.2–0.7 mcg/kg/h |
| Procedural sedation / awake intubation | 0.5–1 mcg/kg over 10–15 min | 0.2–0.7 mcg/kg/h |
| Adjunct to GA | 0.5–1 mcg/kg over 10–15 min | 0.2–0.7 mcg/kg/h |
| Intranasal (pediatric, off-label) | 1 mcg/kg | — |
Loading doses should be given slowly to minimize hemodynamic instability.
6. Adverse Effects & Contraindications
Adverse effects:
- Hypotension — most common; can persist for hours (limits PACU discharge)
- Bradycardia / Heart block / Sinus arrest — especially with vagotonic co-medications
- Transient hypertension with rapid bolus
- Dry mouth
- Tolerance/dependence with prolonged infusion
High-risk combinations:
- Sympatholytic agents (β-blockers, clonidine)
- Cholinergic agents (neostigmine, physostigmine)
- Other sedatives (synergistic respiratory depression risk)
Use with caution:
- Advanced heart block or sick sinus syndrome (without pacemaker)
- Severe hepatic impairment (↓ clearance)
- Renal impairment (↑ duration of effect)
- Hypovolemia
7. Dexmedetomidine in Muscular Dystrophy (MD) Context
There is no established protocol specifically for dexmedetomidine in muscular dystrophy. However, several properties make it particularly relevant:
- Avoids triggering malignant hyperthermia — unlike volatile agents and succinylcholine, which are contraindicated in Duchenne/Becker MD
- Preserves respiratory function — critical in patients with MD-related respiratory muscle weakness
- Cardiac safety: MD patients often have cardiomyopathy — dexmedetomidine's sympatholytic effect reduces myocardial oxygen demand, but its bradycardia risk requires careful monitoring
- One published case (PMID 38855294, 2024) describes combined general + regional anesthesia in a Duchenne MD patient with LVAD undergoing orthopedic surgery, where careful agent selection (avoiding triggers) was essential
For MD patients, dexmedetomidine fits within a total IV anesthesia (TIVA) or MAC approach avoiding volatile agents.
Summary
Dexmedetomidine's unique profile — cooperative sedation without respiratory depression, analgesia, sympatholysis, and anti-delirium properties — distinguishes it from all other sedatives. Its main limitations are slow onset and hemodynamic effects (bradycardia, hypotension), especially at loading doses. It is a cornerstone of ICU sedation strategy and increasingly used for procedural/MAC sedation and as a GA adjunct.
Sources: Katzung's Basic and Clinical Pharmacology, 16th ed. | Miller's Anesthesia, 10th ed. | Barash Clinical Anesthesia, 9th ed. | Goldman-Cecil Medicine, 2nd ed.
Double lumen ET tube
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for a comprehensive answer with images.
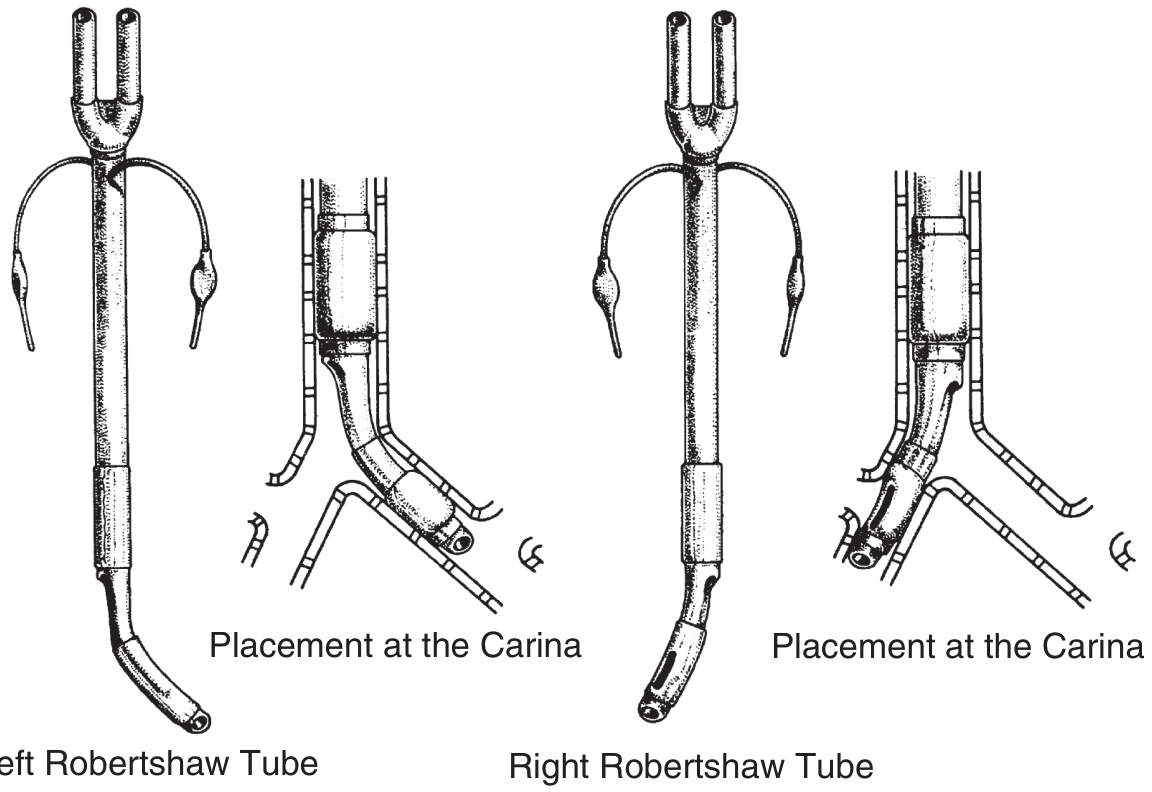
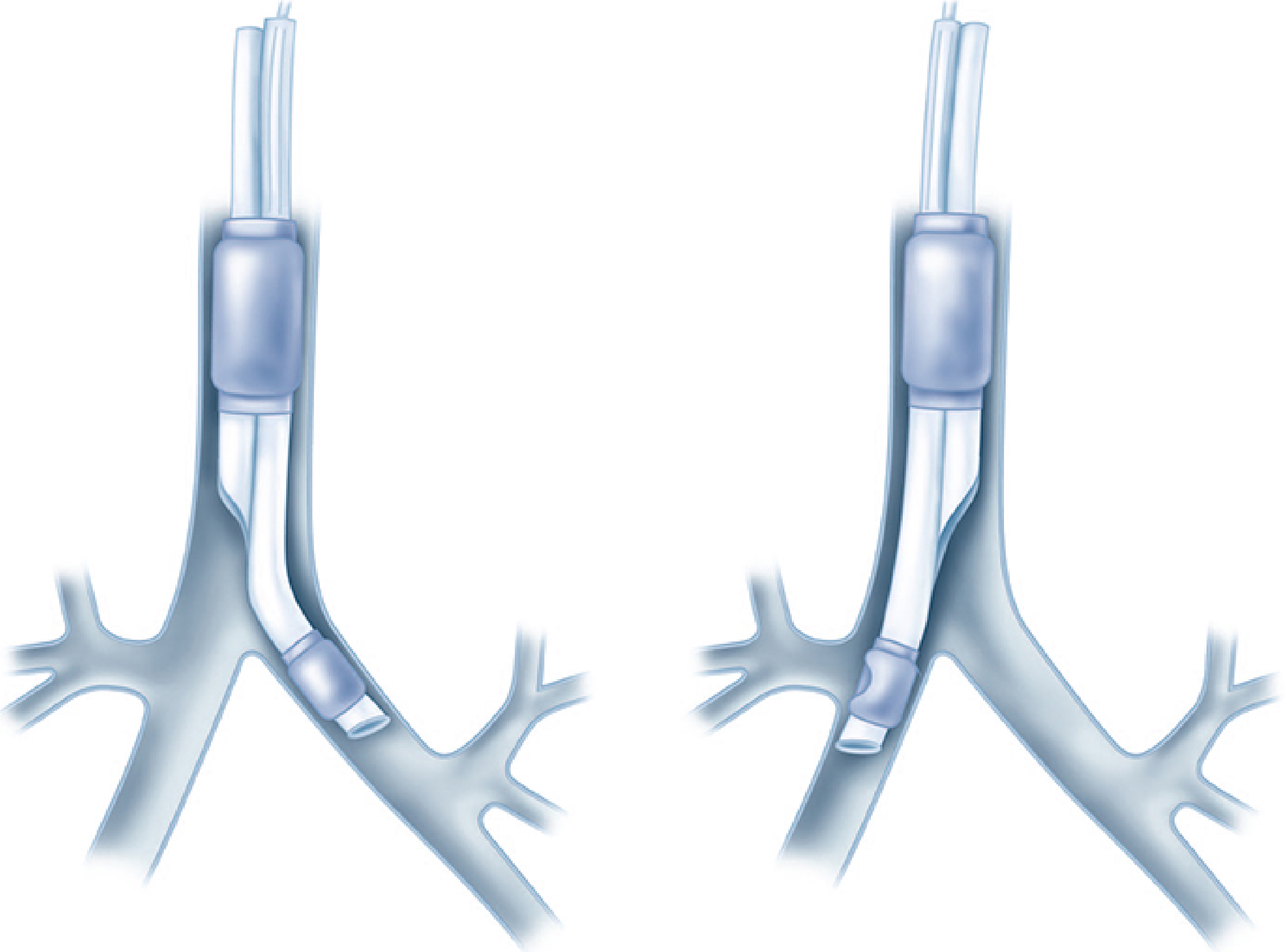
Double-Lumen Endotracheal Tube (DLT)
1. Design & Structure
A DLT has two side-by-side lumens — a longer bronchial lumen (seats in a mainstem bronchus) and a shorter tracheal lumen (terminates in the distal trachea). Each lumen has its own cuff:
- Tracheal cuff — proximal, seals the trachea
- Bronchial cuff (typically colored blue) — distal, seals the intubated bronchus
The two most common designs are:
- Left-sided DLT — bronchial lumen goes into the left mainstem bronchus (preferred for most cases)
- Right-sided DLT — bronchial lumen goes into the right mainstem bronchus; has a ventilation slot to preserve right upper lobe (RUL) ventilation
2. Indications
Absolute Indications (lung isolation mandatory)
- Protection of the healthy lung from contamination (e.g., massive hemoptysis, lung abscess, empyema, bronchopleural fistula)
- Unilateral pulmonary lavage (e.g., pulmonary alveolar proteinosis)
- Large bronchopleural or bronchopleural-cutaneous fistula
- Life-threatening hemorrhage from one lung
Relative Indications (surgical access)
- Thoracic aortic aneurysm repair
- Pneumonectomy, lobectomy, segmentectomy
- Esophageal surgery
- Thoracoscopy (VATS)
- Bilateral sympathectomy / bilateral procedures requiring independent lung ventilation
- Single lung transplantation
— Murray & Nadel's Respiratory Medicine | Barash Clinical Anesthesia, 9th ed.
3. Left vs. Right DLT — Which to Use?
Left-sided DLT is the default for nearly all cases because the left mainstem bronchus is longer (~5 cm), providing a greater margin of safety for positioning and less risk of RUL obstruction.
Indications for a Right-Sided DLT
| Indication |
|---|
| Distorted left mainstem bronchus anatomy (external/intraluminal tumor) |
| Descending thoracic aortic aneurysm compressing left bronchus |
| Left-sided tracheobronchial disruption |
| Left pneumonectomy* |
| Left-sided sleeve resection |
| Left single lung transplantation |
*A left-sided DLT or bronchial blocker can also be used for left pneumonectomy, but must be withdrawn before stapling the left bronchus.
The right mainstem bronchus is shorter (~1.5–2 cm from the carina to the RUL orifice), making right-sided DLT positioning technically demanding — the ventilation slot must precisely align with the RUL orifice. The margin of safety is only 1–8 mm.
— Miller's Anesthesia, 10th ed. | Morgan & Mikhail, 7th ed.
4. Size Selection
| DLT Size (Fr) | Typical Patient |
|---|---|
| 41 Fr | Tall adult male (>170 cm) |
| 39 Fr | Average adult male |
| 37 Fr | Average adult female / small male |
| 35 Fr | Small adult female |
| 32 Fr | Small female (<155 cm) |
Key rule: A properly sized left-sided DLT bronchial tip should be 1–2 mm smaller than the patient's left bronchus diameter (space for the deflated cuff). Chest X-ray and CT scan are valuable for size selection and detecting abnormal tracheobronchial anatomy before placement. Never advance a DLT against significant resistance — external diameter is much larger than a single-lumen ETT.
Depth formula (adults, teeth): ≈ 12 + (height in cm ÷ 10) cm
(Not reliable in patients of Asian descent <155 cm)
— Miller's Anesthesia, 10th ed.
5. Insertion Technique
- Laryngoscopy — MacIntosh (curved) blade preferred; provides more room to maneuver the large tube. Video laryngoscopy is also acceptable.
- Pass the DLT with the distal curvature concave anteriorly.
- Once the bronchial cuff clears the vocal cords, rotate 90° toward the target bronchus (counterclockwise for left-sided placement).
- Advance until resistance is felt (average depth ~29 cm at teeth) or advance over a fiberoptic bronchoscope placed through the bronchial lumen.
- Do not force — the cricoid ring diameter approximates the left mainstem bronchus diameter and is the narrowest point.
— Morgan & Mikhail, 7th ed. | Miller's Anesthesia, 10th ed.
6. Confirming Position — Clinical Protocol (Left-Sided DLT)
Auscultation alone is unreliable — fiberoptic bronchoscopy (FOB) is mandatory.
Step-by-step auscultatory check:
- Inflate tracheal cuff (5–10 mL) → check for bilateral breath sounds
- Unilateral = tube too far down
- Inflate bronchial cuff (1–2 mL)
- Clamp tracheal lumen → ventilate via bronchial lumen
- Should hear left-sided only breath sounds
- If right-sided sounds persist → bronchial opening still in trachea → advance tube
- If right-sided only → tube in right bronchus → reposition
- If left upper lobe silent → tube too far down left bronchus → withdraw
- Unclamp tracheal, clamp bronchial lumen → ventilate via tracheal lumen
- Should hear right-sided breath sounds
- Absent/diminished = bronchial cuff occluding distal trachea → withdraw
FOB confirmation (gold standard):
- Through tracheal lumen: carina visible; bronchial lumen entering left bronchus; blue bronchial cuff 5–10 mm below carina in left bronchus, not herniating over carina
- Through bronchial lumen: patent; left upper and lower lobe orifices visible
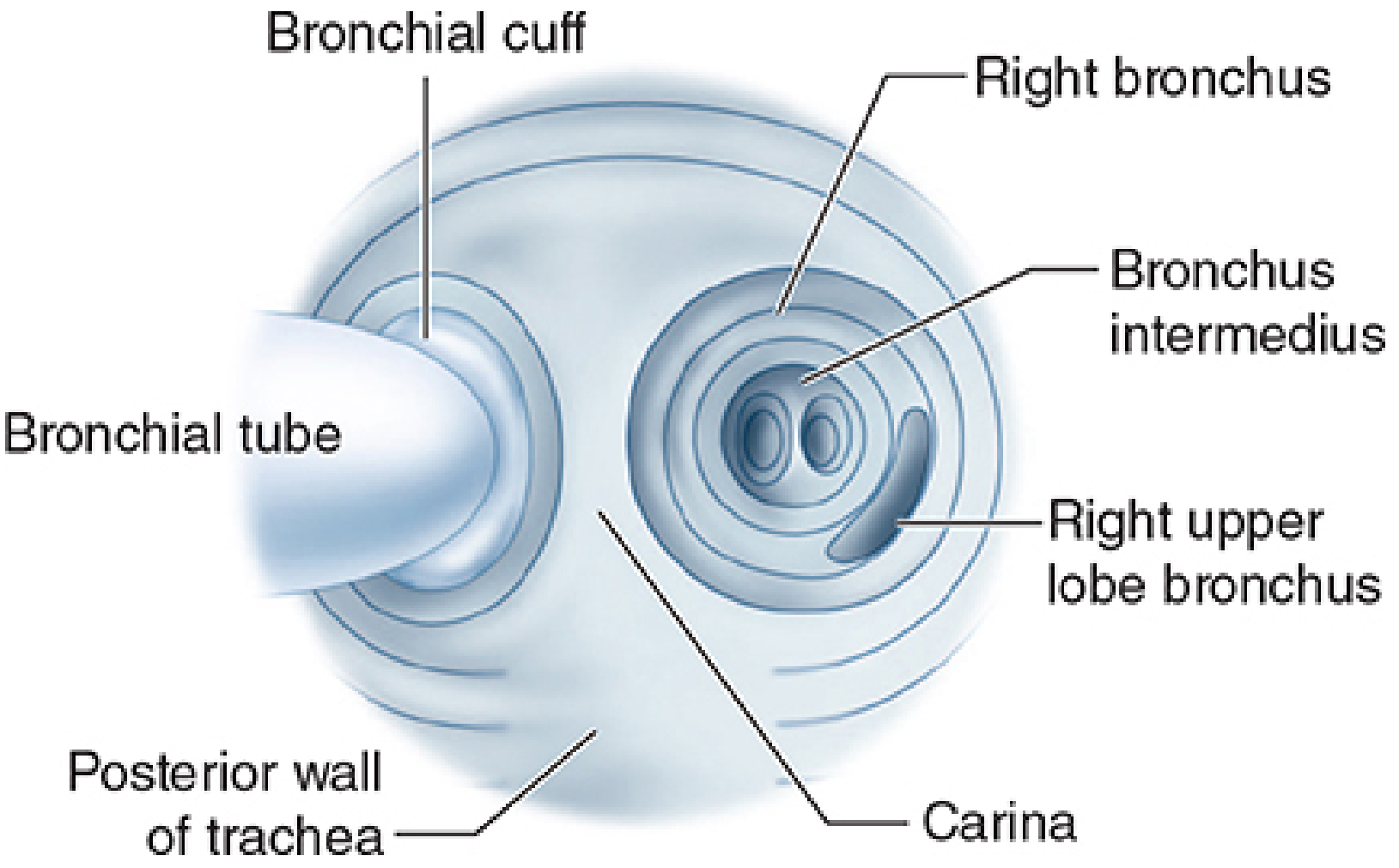
- Through right-sided DLT bronchial lumen: confirm RUL ventilation slot aligns with RUL orifice
- Re-confirm position after repositioning patient to lateral decubitus (tube can migrate)
— Morgan & Mikhail, 7th ed. | Miller's Anesthesia, 10th ed. | Barash, 9th ed.
7. Malposition Problems (6 Types)
| # | Malposition | Consequence | Correction |
|---|---|---|---|
| 1 | DLT in wrong bronchus | Wrong lung collapses; possible laceration | Withdraw and redirect |
| 2 | Too deep (both lumens bronchial) | Diminished/absent contralateral sounds | Withdraw until tracheal lumen is above carina |
| 3 | Not advanced enough (bronchial lumen above carina) | Bilateral sounds through bronchial lumen; no sound through tracheal | Advance further |
| 4 | RUL orifice occluded (right-sided DLT) | RUL atelectasis | Reposition slot to align with RUL |
| 5 | LUL orifice occluded (left-sided DLT) | LUL atelectasis | Withdraw slightly |
| 6 | Bronchial cuff herniation | Cuff obstructs carina | Deflate, reposition |
— Barash Clinical Anesthesia, 9th ed.
8. DLT vs. Bronchial Blocker (BB) — Comparison
| Feature | DLT | Bronchial Blocker |
|---|---|---|
| Lung collapse speed | Faster (open to atmosphere) | Slower |
| Suction to operative lung | Easy (large lumen) | Limited (small channel) |
| CPAP to operative lung | Easy | Possible through blocker lumen |
| Intraoperative dislodgement | Less common | More prone to dislodge |
| Bilateral independent ventilation | Yes | Not easily |
| Already intubated patient / difficult airway | Requires exchange | Preferred (through existing SLT) |
| Open sleeve resection / bronchial anastomosis | DLT (contralateral) | Interferes with surgical field |
| Lung protection from contamination | More reliable (high-volume cuff) | Less reliable (low-volume BB cuff) |
| Double lung transplant / bilateral procedure | Preferred | Not suitable |
Key rule: When both lungs need independent ventilation, or when protection from life-threatening contamination is required (hemoptysis, abscess) → DLT. When a patient is already intubated or has a difficult airway → bronchial blocker via existing single-lumen ETT (≥8.0 mm).
— Barash Clinical Anesthesia, 9th ed. | Murray & Nadel's Respiratory Medicine
9. One-Lung Ventilation (OLV) After DLT Placement
- Patient in lateral decubitus — operative ("up") lung isolated/collapsed; ventilated ("down") lung is dependent
- Start with FiO₂ 1.0 during OLV for safety margin
- Tidal volume: 5–6 mL/kg (lung-protective)
- Apply PEEP 5 cmH₂O to dependent lung
- If hypoxemia: apply CPAP 5–10 cmH₂O to non-dependent lung, or recruit dependent lung
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Barash Clinical Anesthesia, 9th ed. | Miller's Anesthesia, 10th ed. | Morgan & Mikhail's Clinical Anesthesiology, 7th ed.
Permissive hypercapnea
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"permissive hypercapnia" AND "mechanical ventilation"
Comprehensive content gathered. Compiling the full answer now.
Permissive Hypercapnia
1. Definition
Permissive hypercapnia (PHC) is a deliberate ventilatory strategy that accepts elevated arterial PCO₂ — and the resulting respiratory acidosis — as an intentional trade-off in order to avoid ventilator-induced lung injury (VILI) by using low tidal volumes and limiting airway pressures.
The hypercapnia is not the goal itself; it is a consequence of prioritizing lung-protective ventilation. Hence the term "permissive" — the clinician consciously allows CO₂ to rise rather than correcting it by increasing ventilation at the cost of injuring the lungs.
"Permissive hypercapnia accepts the consequences of deliberate hypoventilation to prioritize reduction of alveolar overdistension and airway pressures in patients with poor lung compliance." — Current Surgical Therapy, 14th ed.
2. Physiologic Rationale — Why Allow Hypercapnia?
The Problem: VILI
Mechanical ventilation with normal or large tidal volumes (>8–10 mL/kg) in diseased lungs causes:
- Volutrauma — alveolar overdistension from excessive volume
- Barotrauma — injury from high airway pressures (plateau pressure >30 cmH₂O)
- Atelectrauma — cyclic alveolar collapse and reopening with each breath
- Biotrauma — inflammatory mediator release triggering systemic injury
The Solution: Low Tidal Volume Ventilation
The ARDSNet trial established 6 mL/kg IBW as the protective tidal volume target, keeping plateau pressure ≤30 cmH₂O. This inevitably reduces alveolar ventilation and CO₂ clearance → CO₂ rises.
Rather than increasing the ventilatory rate (which may worsen dynamic hyperinflation, especially in obstructive disease) or increasing tidal volume (which re-inflicts VILI), the hypercapnia is accepted.
3. CO₂ Targets & pH Thresholds
| Parameter | Target |
|---|---|
| PaCO₂ | Up to 60–100 mmHg (tolerated range varies by context) |
| pH | ≥ 7.25 (widely cited minimum threshold) |
| Rate of CO₂ rise | Gradual — ≤10% increase per hour is better tolerated than acute rises |
- Gradual hypercapnia produces less severe acidemia than acute CO₂ elevation because renal compensation has time to partially buffer the pH
- pH <7.15 generally warrants intervention
- If renal compensation is inadequate: NaHCO₃ infusion or THAM (tromethamine) may be used — though evidence for their benefit is uncertain
"Most critical care practitioners adopt a pragmatic approach... targeting a pH greater than 7.25." — Miller's Anesthesia, 10th ed.
4. Clinical Indications
| Condition | Role of PHC |
|---|---|
| ARDS | Primary setting; core component of lung-protective ventilation (ARDSNet protocol) |
| Status asthmaticus (mechanically ventilated) | Prevents barotrauma by ↓ tidal volumes and RR, allowing adequate expiratory time |
| COPD exacerbation | Limits overdistension in dynamic hyperinflation |
| Neonatal respiratory failure | Used to minimize barotrauma in surfactant-deficient lungs |
| One-lung ventilation (thoracic surgery) | Low VT to non-operative lung may cause CO₂ accumulation |
In asthma: PHC minimizes tidal volume and RR to ↓ peak inspiratory pressures, allowing adequate expiratory time to prevent air trapping. Ketamine is the preferred induction agent (bronchodilator).
— Rosen's Emergency Medicine | Murray & Nadel's | Current Surgical Therapy, 14th ed.
5. Physiologic Effects of Hypercapnia
Potentially Protective
- Attenuates free radical–mediated lung injury (antioxidant effect at tissue level)
- Reduces pulmonary inflammation
- Vasodilatory effect on systemic vasculature
- Shifts oxygen–haemoglobin dissociation curve rightward (Bohr effect) → ↑ O₂ delivery to tissues
Potentially Harmful
| System | Effect |
|---|---|
| CNS | ↑ cerebral blood flow → ↑ ICP; neurologic dysfunction at severe levels |
| Cardiovascular | Myocardial depression; ↑ pulmonary vascular resistance; cardiac arrhythmias; RV dysfunction |
| Renal | ↓ renal blood flow |
| Acid-base | Severe acidemia (especially if superimposed on metabolic acidosis, e.g., lactic acidosis) |
| Alveolar epithelium | Some data suggest direct injurious effect |
| Immunologic | Impairs wound healing, cellular immune function |
"The magnitude of the acidaemia associated with permissive hypercapnia may be augmented if superimposed on metabolic acidosis, such as lactic acidosis. This combination is not uncommon in the critical care unit." — Brenner & Rector's The Kidney
6. Contraindications / Use with Caution
| Contraindication | Reason |
|---|---|
| Traumatic brain injury / ↑ ICP | CO₂ causes cerebral vasodilation → ↑ CBF → ↑ ICP → herniation |
| Cerebrovascular disease / acute stroke | Same mechanism |
| Severe pulmonary hypertension | CO₂ ↑ PVR → right heart strain |
| Severe right ventricular dysfunction | Hypercapnia impairs RV function |
| Acute renal insufficiency | Limits ability to buffer with renal compensation |
| Severe metabolic acidosis | Combined acidosis → pH can drop dangerously |
| Cardiac arrhythmias | Hypercapnia is proarrhythmic |
| Pregnancy | High maternal PCO₂ may impede CO₂ transfer from fetus → fetal acidemia |
7. Management of Acidosis During PHC
When pH falls despite PHC:
- Sodium bicarbonate (NaHCO₃) — IV infusion; commonly used, though evidence is uncertain; gives CO₂ as byproduct (must be able to exhale it)
- THAM (tromethamine) — buffers CO₂ without generating additional CO₂; useful when CO₂ elimination is impaired
- Goal: bring pH to ≥7.15–7.25, not to normalize bicarbonate or pH completely
8. Alternatives to Minimize Hypercapnia (When PHC Poorly Tolerated)
| Intervention | Mechanism |
|---|---|
| Prone positioning | Homogenizes V/Q → improves CO₂ clearance and oxygenation |
| ECCO₂R (extracorporeal CO₂ removal) | Decarboxylates blood extracorporeally; allows ultra-low tidal volume ventilation; used in severe ARDS, COPD exacerbations, bridge to transplant |
| ECMO (veno-venous) | Full respiratory support; for refractory ARDS (P/F ratio <60) |
| HFOV | Very low VT (<100 mL) at high frequency; alternative in select cases |
| Airway pressure release ventilation (APRV) | Maintains high constant pressure with brief releases; controversial evidence |
"Although permissive hypercapnia was previously thought to be benign, it has several physiologic consequences, and alternative interventions, including prone ventilation, ultralow tidal volume ventilation, ECMO, and ECCO₂R, are being used to minimize hypercapnia or even aim for normocapnia." — Comprehensive Clinical Nephrology, 7th ed.
9. Key Evidence
- ARDSNet (ARMA) trial — The landmark RCT showing 22% relative mortality reduction with VT 6 mL/kg IBW vs 12 mL/kg in ARDS. Notably, this trial treated respiratory acidosis aggressively (increased RR up to 35/min, used NaHCO₃); it did not deliberately pursue hypercapnia.
- The original pilot studies by Hickling et al. (1994) reported low mortality using low-volume, pressure-limited ventilation with PHC, providing the conceptual foundation.
- Uncertainty remains about whether hypercapnia itself is beneficial, harmful, or neutral — current evidence supports tolerating it as a side effect of lung-protective ventilation, not actively targeting it.
"Given the uncertainty about permissive hypercapnia, the original ARDSNet trial... treated respiratory acidosis aggressively. In the absence of other data, avoidance of hypercapnia where possible seems prudent." — Murray & Nadel's Respiratory Medicine
Summary
| Feature | Value |
|---|---|
| Core mechanism | Low VT (6 mL/kg IBW) + limit Pplat ≤30 cmH₂O → CO₂ rises |
| Accepted PaCO₂ | Up to ~100 mmHg (disease-dependent) |
| pH floor | ≥ 7.25 (broadly accepted); intervene at <7.15 |
| Primary indication | ARDS; also severe asthma, COPD, neonatal RDS |
| Absolute contraindications | ↑ ICP, TBI, severe RV dysfunction |
| Acidosis management | NaHCO₃, THAM |
| Escape strategy | ECCO₂R, ECMO, prone positioning |
Sources: Murray & Nadel's Respiratory Medicine | Miller's Anesthesia, 10th ed. | Current Surgical Therapy, 14th ed. | Brenner & Rector's The Kidney | Comprehensive Clinical Nephrology, 7th ed. | Rosen's Emergency Medicine
PEEP
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Excellent — I now have comprehensive content from across 6 textbooks. Compiling the full answer.
Positive End-Expiratory Pressure (PEEP)
1. Definition
PEEP is the maintenance of positive airway pressure above atmospheric after the completion of passive exhalation during mechanical ventilation. The ventilator's PEEP valve allows expiratory flow only when airway pressure exceeds the set PEEP level, thereby preventing alveolar pressure from returning to zero at end-expiration.
CPAP vs. PEEP:
- PEEP — positive end-expiratory pressure applied during mechanical (ventilator-cycled) breaths
- CPAP — continuous positive pressure applied during spontaneous breathing (invasive or noninvasive)
- In clinical practice the terms are often used interchangeably since most modern ventilators deliver a combination; strictly speaking they differ in whether breathing is controlled or spontaneous
— Morgan & Mikhail's Clinical Anesthesiology, 7th ed.
2. Physiologic Effects
A. Pulmonary Effects
Primary effect: ↑ Functional Residual Capacity (FRC)
| Mechanism | Result |
|---|---|
| Expansion of partially collapsed alveoli | ↓ Intrapulmonary shunt → ↑ PaO₂ |
| Keeps FRC above closing capacity | Prevents cyclic alveolar collapse (atelectrauma) |
| Improves lung compliance | ↓ Work of breathing |
| Redistributes extravascular lung water away from alveolar-capillary interface toward peribronchial/perihilar areas | Improves oxygenation in pulmonary edema |
| ↑ Alveolar volume for tidal delivery | Potentially ↓ VILI risk |
"The major effect of PEEP and CPAP on the lungs is to increase FRC. In patients with decreased lung volume, appropriate levels will increase FRC and tidal ventilation above closing capacity, improve lung compliance, and correct ventilation/perfusion abnormalities." — Morgan & Mikhail, 7th ed.
Important caveat — overdistension:
- PEEP does not uniformly recruit all lung units; it can overdistend well-aerated (non-dependent) regions while potentially failing to recruit collapsed dependent zones
- This is particularly relevant in focal lung disease (e.g., lobar pneumonia) where PEEP may simply over-distend healthy regions and worsen V/Q mismatch
- PEEP is most effective in diffuse parenchymal disease (ARDS, pulmonary edema)
PEEP does not reduce total extravascular lung water — it redistributes it.
B. Cardiovascular Effects
Increased intrathoracic pressure from PEEP has significant hemodynamic consequences:
| Effect | Mechanism |
|---|---|
| ↓ Venous return (preload) | ↑ Intrathoracic pressure compresses great veins |
| ↓ Cardiac output | Primarily from reduced RV preload |
| ↑ RV afterload | Alveolar overdistension compresses pulmonary capillaries → ↑ PVR |
| Cardiac compression | High PEEP can compress the right atrium directly |
| Elevated PCWP readings | Falsely elevated due to transmitted airway pressure |
| ↑ Alveolar dead space | Capillary compression diverts perfusion → areas with good ventilation but no perfusion |
"The major risks of PEEP are overdistention of the lung and hemodynamic consequences, such as decreasing cardiac output by decreasing venous return or increasing right ventricular afterload." — Goldman-Cecil Medicine
Clinical implication: Adequate volume resuscitation is essential before applying high PEEP; hypovolemia compounds the preload-reducing effect.
C. CNS Effects
- High PEEP → ↑ intrathoracic pressure → impedes cerebral venous drainage → ↑ ICP
- The "optimal PEEP for oxygenation may be the worst PEEP for cerebral venous drainage"
3. Indications
| Indication | Notes |
|---|---|
| ARDS | Core component of lung-protective ventilation; most evidence-based application |
| Pulmonary edema (cardiogenic & non-cardiogenic) | Redistributes edema fluid; ↓ shunt |
| Post-operative atelectasis | Prevents / recruits collapsed alveoli |
| General mechanical ventilation | 5 cmH₂O "physiologic PEEP" routinely added to compensate for loss of intrinsic PEEP/FRC after intubation |
| One-lung ventilation | Maintains FRC of dependent ventilated lung |
| CPAP (non-intubated) | Obstructive sleep apnea; acute cardiogenic pulmonary edema; NIV in COPD exacerbations |
4. PEEP Settings & Titration
Routine / Physiologic PEEP
- 5–8 cmH₂O routinely added to all mechanically ventilated patients to preserve FRC and compensate for the loss of intrinsic glottic PEEP (~3–5 cmH₂O) that normally exists in spontaneously breathing patients
In ARDS — ARDSNet FiO₂/PEEP Tables
Two ARDSNet PEEP strategies are used alongside VT of 6 mL/kg IBW:
Lower PEEP table (default strategy):
| FiO₂ | 0.3 | 0.4 | 0.4 | 0.5 | 0.5 | 0.6 | 0.7 | 0.7 | 0.7 | 0.8 | 0.9 | 0.9 | 0.9 | 1.0 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PEEP | 5 | 5 | 8 | 8 | 10 | 10 | 10 | 12 | 14 | 14 | 14 | 16 | 18 | 18–24 |
Higher PEEP table (for moderate-severe ARDS, typically PEEP ~5 cmH₂O higher than lower table for a given FiO₂)
Titration Methods
1. Plateau pressure method:
- Increase PEEP in steps → observe plateau pressure
- When plateau pressure stops increasing (lung is optimally recruited), peak and plateau may actually decrease as more lung volume is available
- Once plateau pressure rises disproportionately beyond the PEEP increment → overdistension; reduce PEEP
2. Compliance-guided (decremental PEEP) method:
- After recruitment maneuver, set PEEP to 20–25 cmH₂O
- Decrease PEEP stepwise; select PEEP that maximizes respiratory system compliance (ΔP = driving pressure = Pplat – PEEP)
- Promising physiologically but the largest RCT (ART trial, 2017) showed increased 28-day mortality with aggressive recruitment + compliance-titrated PEEP → now discouraged for routine use
3. Pressure-volume (P-V) loop method:
- Lower inflection point (LIP) on P-V curve = pressure at which collapsed alveoli begin recruiting
- Set PEEP above LIP to keep recruited alveoli open
- Upper inflection point = overdistension threshold; keep plateau below it
4. Esophageal manometry (transpulmonary pressure):
- Esophageal pressure ≈ pleural pressure; transpulmonary pressure = airway pressure − esophageal pressure
- Useful in obese patients, ascites, chest wall edema where chest wall compliance is reduced (allows higher PEEP safely)
- Large RCT (EPVent-2) showed no mortality difference vs. empiric PEEP — not standard practice
5. Clinical endpoint method:
- Increase PEEP until: (a) PaO₂ ceases to improve, (b) CO₂ rises (overdistension sign), or (c) BP drops
- Reduce if complications emerge; volume-resuscitate if hemodynamics limit the desired PEEP
"Optimal PEEP can be determined... the clini cian must readily identify the plateau in the plateau pressure trend." — Roberts & Hedges' Clinical Procedures in Emergency
5. Intrinsic PEEP (Auto-PEEP / iPEEP)
Intrinsic PEEP is end-expiratory alveolar pressure above the set external PEEP, caused by incomplete exhalation before the next breath begins.
Causes
- Obstructive disease (asthma, COPD) — high airway resistance + high compliance = long expiratory time constant (τ = R × C)
- Short expiratory time — high RR, high I:E ratio, large VT
- Dynamic airway collapse — expiratory flow limitation even with adequate time
Time constant = Resistance (cmH₂O/L/s) × Compliance (L/cmH₂O)
- ~3 time constants needed for complete exhalation
- Example: R = 10 cmH₂O/L/s, C = 0.05 L/cmH₂O → τ = 0.5 s → needs ~1.5 s to empty
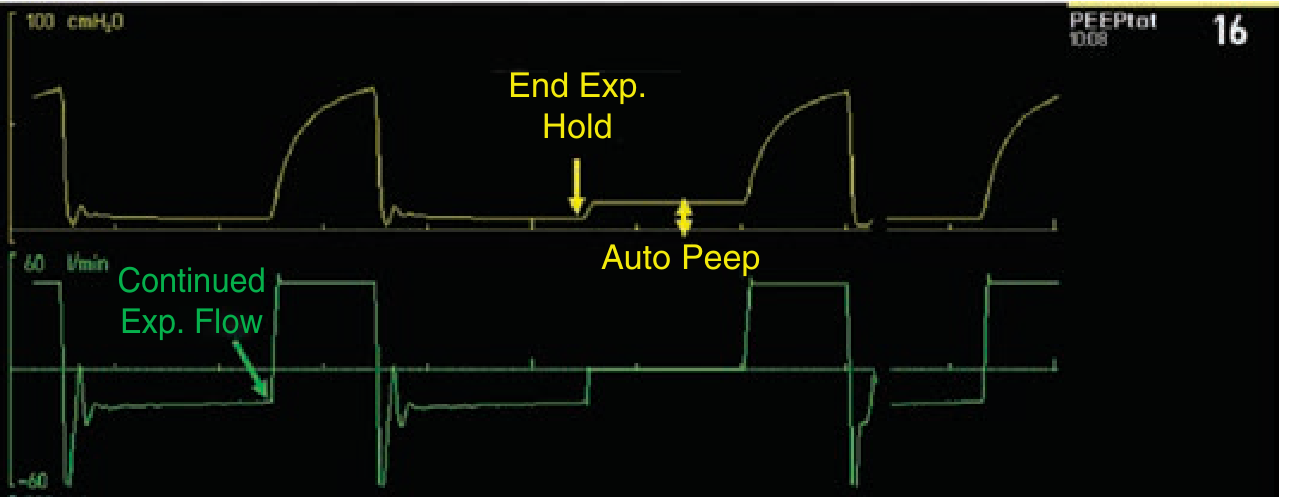
Detection
- Flow-time curve: expiratory flow does not return to zero before the next breath
- Expiratory hold maneuver: measure pressure during expiratory occlusion = total PEEP − set PEEP = iPEEP
- Clinical signs: unexpectedly ↑ airway pressures, ↓ compliance, hypotension
Consequences
- ↑ Intrathoracic pressure → ↓ venous return → hypotension / ↓ CO
- ↑ Work of breathing (patient must generate sufficient effort to overcome iPEEP before triggering the ventilator)
- Contributes to VILI (dynamic hyperinflation)
- Can cause hemodynamic collapse if severe (treat by briefly disconnecting from ventilator to allow full exhalation)
Management
- Reduce RR and/or VT
- Extend expiratory time (adjust I:E ratio → ≥1:3 or 1:4)
- Bronchodilators (↓ resistance)
- Apply external PEEP ≤ iPEEP to reduce inspiratory trigger threshold (makes triggering easier without ↑ end-expiratory lung volume)
"Theoretically, for the spontaneously breathing patient, extrinsic PEEP applied to counteract intrinsic PEEP should not cause an increase in EELV until extrinsic PEEP exceeds intrinsic PEEP." — Miller's Anesthesia, 10th ed.
6. Adverse Effects
| Adverse Effect | Mechanism |
|---|---|
| ↓ Cardiac output | ↓ Venous return, ↑ RV afterload |
| Hypotension | Especially in hypovolemia |
| Barotrauma / pneumothorax | Overdistension at high PEEP |
| ↑ ICP | Impaired cerebral venous drainage |
| ↑ Alveolar dead space | Capillary compression in overdistended units → ↑ PaCO₂ |
| Worsening V/Q mismatch | In focal disease (PEEP diverts flow to injured regions) |
| False elevation of PCWP | Transmitted airway pressure artifact |
| Auto-PEEP generation | If I:E ratio or compliance is unfavorable |
7. Recruitment Maneuvers (RMs)
Applied alongside PEEP to re-open collapsed alveoli:
Standard RM: CPAP 40 cmH₂O × 40 seconds (or 30 cmH₂O × 30 seconds)
Incremental PEEP titration RM: ↑ PEEP by 2–5 cmH₂O every 3–5 min until compliance worsens or hemodynamics deteriorate
Evidence:
- Multiple RCTs show RMs + high PEEP improve oxygenation but do not reduce mortality in ARDS
- The ART trial (2017): aggressive RM + compliance-titrated PEEP → increased 28-day mortality — use with caution
- RMs are not benign: transient hypotension, desaturation, dyssynchrony, rare tension pneumothorax
"A more recent study... the group that received recruitment maneuvers and titrated PEEP displayed increased 28-day all-cause mortality." — Murray & Nadel's Respiratory Medicine
Current consensus: Higher PEEP (vs. lower PEEP) is safe and improves oxygenation in ARDS, but there is no mortality benefit. In the absence of strong evidence, individualized PEEP selection based on patient response and hemodynamic tolerance is recommended.
8. PEEP in Specific Contexts
| Context | PEEP Approach |
|---|---|
| ARDS (diffuse) | 8–15+ cmH₂O per FiO₂/PEEP table; titrate by compliance/hemodynamics |
| ARDS (focal, e.g., lobar pneumonia) | Low PEEP — high PEEP worsens V/Q mismatch |
| Obese patients / ascites / chest wall edema | Higher PEEP may be safe (chest wall compliance reduced); esophageal manometry can guide |
| COPD / asthma | Caution — high iPEEP already present; external PEEP ≤ iPEEP to lower trigger threshold; avoid over-inflation |
| One-lung ventilation | 5 cmH₂O PEEP to dependent lung; avoid in COPD (risk of auto-PEEP stacking) |
| TBI / ↑ ICP | Keep PEEP as low as clinically tolerable; high PEEP impairs cerebral venous drainage |
| RV failure / severe pulmonary HTN | Use with great caution — PEEP ↑ PVR → worsens RV afterload |
| Cardiogenic pulmonary edema | CPAP/PEEP beneficial — redistributes edema fluid, ↓ preload/afterload, improves oxygenation |
Summary Table
| Feature | Value |
|---|---|
| Definition | Positive airway pressure maintained after passive exhalation |
| Primary effect | ↑ FRC → alveolar recruitment → ↓ shunt → ↑ PaO₂ |
| Starting PEEP (most patients) | 5 cmH₂O ("physiologic") |
| ARDS range | 5–20+ cmH₂O depending on FiO₂ requirements |
| pH floor with PEEP | Maintain Pplat ≤30 cmH₂O |
| Auto-PEEP formula | iPEEP = Total PEEP − Set PEEP (measured on expiratory hold) |
| Key hemodynamic concern | ↓ CO from ↓ venous return (ensure adequate volume) |
| Mortality benefit in ARDS? | Low VT (6 mL/kg) = YES; higher PEEP vs. lower PEEP = NO (equal mortality, better oxygenation) |
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7th ed. | Miller's Anesthesia, 10th ed. | Murray & Nadel's Respiratory Medicine | Goldman-Cecil Medicine | Current Surgical Therapy, 14th ed. | Rosen's Emergency Medicine | Roberts & Hedges' Clinical Procedures in Emergency | Barash Clinical Anesthesia, 9th ed.
AUTO PEEP
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Both images are excellent. Compiling the comprehensive answer now.
Auto-PEEP (Intrinsic PEEP / Dynamic Hyperinflation)
Synonyms: Auto-PEEP | Intrinsic PEEP (iPEEP) | Dynamic hyperinflation | Breath stacking | Occult PEEP
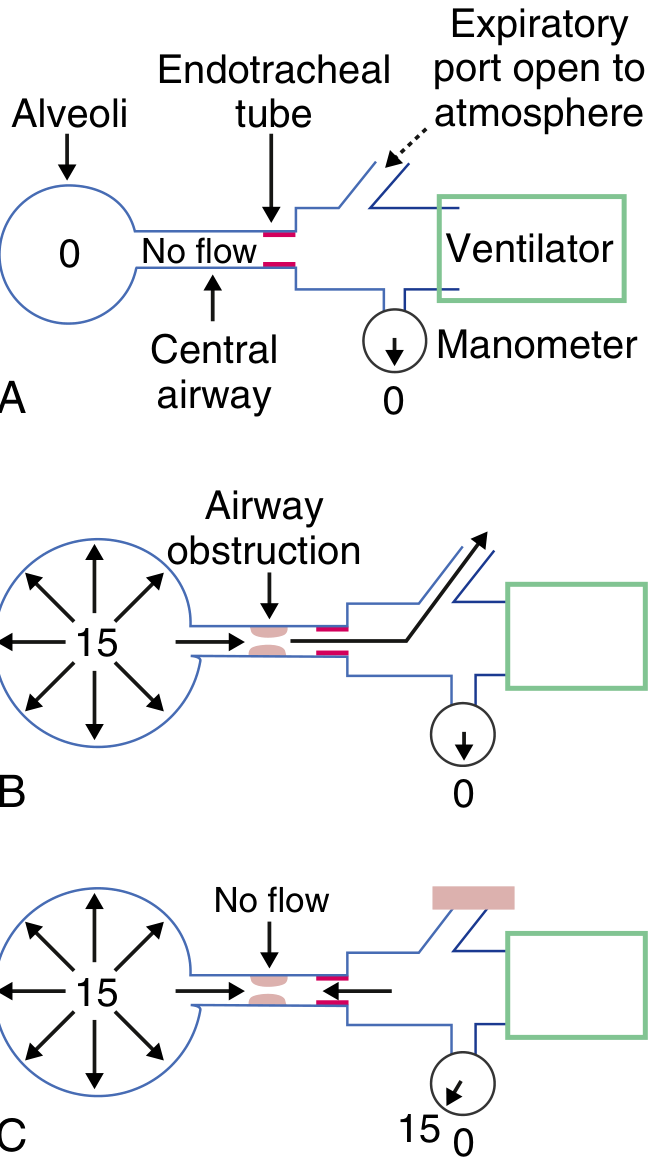
1. Definition
Auto-PEEP = the difference between alveolar pressure and airway opening pressure at end-expiration, arising when exhalation is incomplete before the next breath begins.
It represents trapped gas — air that should have been exhaled remains in the alveoli, elevating end-expiratory lung volume (EELV) above the static functional residual capacity (FRC). This is dynamic hyperinflation.
"Auto-PEEP is defined as the difference between alveolar pressure and airway opening pressure at end expiration... associated with dynamic hyperinflation, which is an increase in the end-expiratory lung volume above the value that would be obtained if there was complete exhalation to the static FRC." — Goldman-Cecil Medicine
Key distinction: Auto-PEEP is not visible on the ventilator pressure manometer during normal cycling — the pressure drop occurs across the obstructed airways, upstream of the measurement point. The ventilator circuit reads only set PEEP while alveolar pressure is substantially higher.
2. Pathophysiology
The Expiratory Time Constant
Complete exhalation requires approximately 3 time constants (τ):
τ = Resistance (R) × Compliance (C)
- Normal: R ≈ 5 cmH₂O/L/s, C ≈ 0.05 L/cmH₂O → τ = 0.25 s → needs ~0.75 s to fully empty
- COPD: R ↑↑, C ↑↑ → τ = 0.5–1.0 s+ → needs 1.5–3+ seconds
If the ventilator delivers the next breath before 3τ have elapsed, the residual volume accumulates — breath stacking — and auto-PEEP builds.
Two Mechanisms of Incomplete Exhalation
| Mechanism | Example |
|---|---|
| Insufficient expiratory time | High RR, short I:E ratio, large VT, high minute ventilation |
| Expiratory flow limitation | COPD (dynamic airway collapse, ↓ elastic recoil), asthma (bronchospasm), mucous plugging — flow ceases even with adequate time |
The second mechanism (flow limitation) is particularly insidious — even if you lengthen expiratory time, a biphasic flow pattern occurs: rapid initial emptying → sudden cessation of flow due to airway collapse, regardless of remaining time.
3. Causes / Risk Factors
| Category | Specific Conditions |
|---|---|
| Obstructive lung disease | COPD, asthma, bronchospasm — most common cause |
| Ventilator settings | High respiratory rate, high tidal volume, short expiratory time, high I:E ratio (e.g., 1:1 or inverse) |
| High minute ventilation demand | Sepsis, fever, metabolic acidosis, agitation |
| Airway obstruction | Mucous plugging, ETT kinking, biting |
| Increased compliance | Emphysema (high compliance + flow limitation) |
| One-lung ventilation | Reduced lung volume receiving full VT |
4. Detection & Measurement
Bedside Clinical Signs
- Expiratory flow on the flow-time waveform does not return to zero before the next breath (most sensitive continuous sign)
- Unexpectedly ↑ peak airway pressures without change in VT (↑ resistance)
- Unexpectedly ↓ apparent compliance (falsely low, because total PEEP is underestimated)
- Hypotension — especially after intubation
- Failure to trigger — patient makes efforts but ventilator does not register them (ineffective efforts)
- Tachycardia, agitation in a spontaneously breathing patient "fighting" the ventilator
Gold Standard: End-Expiratory Hold Maneuver
- Patient must be passive (no spontaneous breathing effort)
- Press expiratory hold button on the ventilator
- Airway is occluded at end-expiration → alveolar, central airway, and circuit pressure equilibrate
- Read the pressure displayed on the manometer
Auto-PEEP = Total PEEP (measured) − Set PEEP
Dynamic Hyperinflation Volume
- Prolonged expiration (20–30 seconds to atmosphere) → volume of additional gas released = degree of dynamic hyperinflation
Unreliable in Spontaneously Breathing Patients
- Expiratory hold requires complete passivity; spontaneous efforts during the hold falsely lower the measured value
- Ineffective triggering efforts (>10% of breaths in ~25% of PSV patients) suggest significant auto-PEEP
5. Consequences
Hemodynamic
| Effect | Mechanism |
|---|---|
| ↓ Venous return | ↑ Mean intrathoracic pressure compresses great veins → ↓ preload to RV |
| ↓ Cardiac output | Reduced RV filling → reduced LV output |
| ↑ RV afterload | Overdistended alveoli compress pulmonary capillaries → ↑ PVR |
| Hypotension / circulatory collapse | Especially severe immediately post-intubation (vasodilating sedatives + reduced venous tone compound preload loss) |
| Falsely elevated PCWP | Transmitted airway pressure artifact |
"Auto-PEEP and the attendant dynamic hyperinflation increase pleural pressure and right atrial pressure, thereby leading to a decrease in the driving pressure for venous return. This can be magnified immediately after intubation because compensatory mechanisms are impaired by pharmacologic agents used for intubation." — Goldman-Cecil Medicine
Respiratory
| Effect | Mechanism |
|---|---|
| Increased work of breathing | Patient must first overcome auto-PEEP before any inspiratory flow is generated → inspiratory threshold load |
| Ineffective triggering | Ventilator does not sense inspiratory effort until patient pressure exceeds auto-PEEP + set trigger threshold |
| ↑ Peak airway pressure | Total PEEP is higher than expected for a given VT |
| Falsely low compliance | Compliance calculated using set PEEP underestimates total PEEP → overestimates stiffness |
| Barotrauma | Dynamic hyperinflation → overdistension → pneumothorax, pneumomediastinum |
| VILI | Breath stacking compounds volutrauma and barotrauma |
| ↑ Dead space | Overdistended units compress capillaries → V/Q mismatch |
6. Management
The fundamental goals are: ↓ minute ventilation, ↑ expiratory time, ↓ airway resistance.
Immediate / Emergency (Hemodynamic Collapse)
"If hypotension occurs, disconnect the patient from the ventilator for 15–20 seconds" — allows complete exhalation, immediate relief of dynamic hyperinflation → BP recovers
This is the fastest diagnostic test and treatment simultaneously.
Ventilator Setting Adjustments
| Intervention | Rationale |
|---|---|
| ↓ Respiratory rate | Most effective way to ↑ expiratory time; slow rate to 10–14/min for obstructive disease |
| ↓ Tidal volume | Reduces volume to exhale; auto-PEEP ∝ VT |
| ↑ Inspiratory flow rate | Shortens inspiratory time → more time available for expiration within the same cycle |
| ↑ I:E ratio (e.g., 1:3, 1:4) | Lengthens expiratory time fraction |
| Tolerate hypercapnia | Accept permissive hypercapnia (pH ≥7.20) rather than increasing RR to normalize PaCO₂ — increasing RR is counterproductive in obstructive disease |
| Avoid inverse ratio ventilation | Shortens expiratory time → worsens air trapping |
"Increasing the respiratory rate is counterproductive because it shortens the exhalation time, leading to an additional breath prior to the lungs completely emptying." — Tintinalli's Emergency Medicine
Pharmacologic
| Drug | Rationale |
|---|---|
| Bronchodilators (β₂-agonists, anticholinergics) | ↓ Airway resistance → faster emptying → ↓ τ |
| Systemic corticosteroids | ↓ Airway inflammation in COPD/asthma |
| Adequate sedation ± neuromuscular blockade | Eliminates active expiratory muscle contraction (which can worsen air trapping) and reduces O₂ demand / CO₂ production |
External PEEP to Counteract Auto-PEEP (in spontaneously breathing patients)
When a patient is actively breathing against auto-PEEP, they must generate sufficient effort to overcome iPEEP before the ventilator triggers. Applying external PEEP ≤ iPEEP offloads this threshold:
- Reduces inspiratory trigger work without adding to end-expiratory lung volume
- Rule: Set external PEEP ≤ 75–85% of measured iPEEP
- Do not apply external PEEP exceeding iPEEP — this will increase EELV and worsen hyperinflation
"Theoretically, for the spontaneously breathing patient, extrinsic PEEP applied to counteract intrinsic PEEP should not cause an increase in EELV until extrinsic PEEP exceeds intrinsic PEEP." — Miller's Anesthesia, 10th ed.
7. Auto-PEEP in COPD / Asthma — Specific Approach
These patients have flow limitation (not just high resistance) — they exhibit effort-independent expiratory flow cessation. Management priorities:
| Setting | Target |
|---|---|
| Respiratory rate | 10–14 breaths/min |
| Tidal volume | 6–8 mL/kg IBW |
| I:E ratio | ≥1:3 (preferably 1:4 or longer) |
| Inspiratory flow | 60–80 L/min (high flow → short insp. time) |
| PEEP (set) | 0–5 cmH₂O initially; may apply up to ~85% of iPEEP to assist triggering |
| PaCO₂ | Tolerate hypercapnia; target pH ≥7.20 |
| Bronchodilators | Aggressive nebulized β₂-agonists + ipratropium |
8. Summary
| Feature | Details |
|---|---|
| Definition | Alveolar pressure > airway opening pressure at end-expiration due to incomplete exhalation |
| Synonyms | Intrinsic PEEP, iPEEP, dynamic hyperinflation, breath stacking |
| Calculation | Auto-PEEP = Total PEEP (end-expiratory hold) − Set PEEP |
| Primary cause | Obstructive lung disease + insufficient expiratory time |
| Key detection | Flow-time waveform (flow ≠ 0 before next breath); end-expiratory hold maneuver |
| Hemodynamic effect | ↓ Venous return → ↓ CO → hypotension (can cause circulatory collapse) |
| Respiratory effect | ↑ Work of breathing, ineffective triggering, barotrauma, VILI |
| Emergency Rx | Disconnect from ventilator 15–20 sec |
| Definitive Rx | ↓ RR, ↓ VT, ↑ flow rate, ↑ I:E, bronchodilators, tolerate permissive hypercapnia |
| External PEEP role | Apply ≤ iPEEP to reduce trigger threshold in spontaneously breathing patients |
Sources: Goldman-Cecil Medicine | Miller's Anesthesia, 10th ed. | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine | Roberts & Hedges' Clinical Procedures in Emergency | Current Surgical Therapy, 14th ed.
This is a shared conversation. Sign in to Orris to start your own chat.