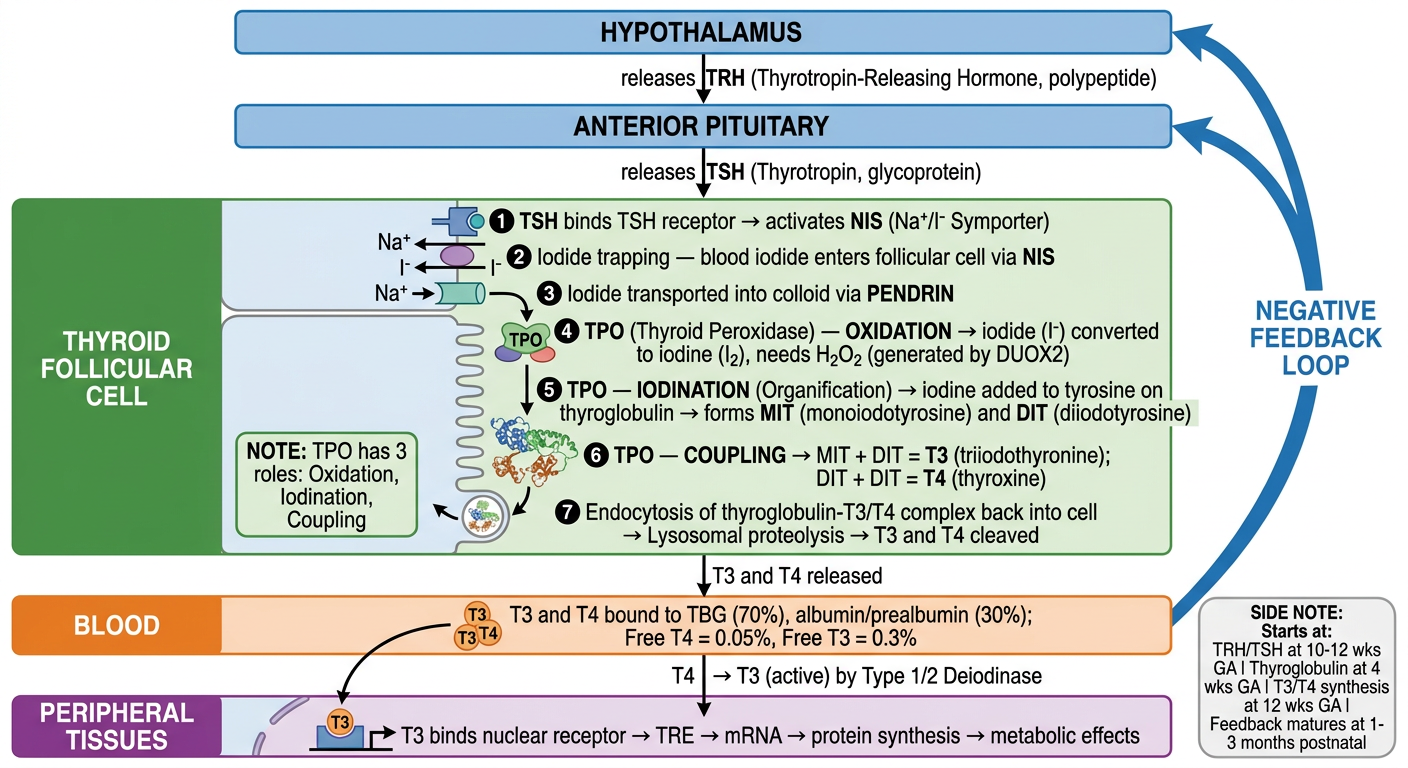
Sorry here is the entire notes 04. HYPOTHYROIDISM MY NOTES Watch Video Lecture on RAAONLINE APP Specialty: Pediatrics Course: Endocrinology Faculty: Dr. Abinaya.K.A Duration: 31 mins Hypothyroidism: Insufficient circulating thyroid hormone, Deficient production due to defect in thyroid gland (primary). OR Reduced thyrotropin stimulation(TSH) (central or secondary). Congenital or aquired. Congenital Hypothyroidism: Causes: Most common cause: Thyroid Dysgenesis. (Hypoplastic (on Aplastic) Next: dyshormonogenesis. nonogenesis. (Synthetic defect in the Thyroid hormone synthesis) Mostly detected on newborn screening programmes. Severe cases only: manifests in 1" week of life. Epidemiology: 1 in 4000 infants worldwide. Etiologic Classification of Congenital Hypothyroidism: Primary hypothyroidism: Thyroid dysgenesis: hypothyrodism due to a developmental anomaly of thyroid gland (Thyroid ectopia, hypoplasia, hemiagenesis). Associated mutations: (These account for only 2% of thyroid * dysgenesis cases; 98%unknown). TTF-2, NKX2.1, NKX2.5, PAX-9. Thyroid dyshormonogenesis: hypothyroidism due to impaired hormone production. Associated mutations: Sodium-iodide symporter defect. Thyroid peroxidase defects. Hydrogen peroxide generation defects (DUOX2, DUOXA2 gene mutations). MY NOTES Pendrin defect (Pendred Syndrome). Thyroglobulin defect ⚫lodotyrosine deiodinase defect (DEHALI, SECISBP2 gene mutations). Resistance to TSH binding or signaling. Associated mutations: TSH Receptor Defect. G-protein mutation: pseudohypoparathyroidism type la. Central hypothyroidism (syn: Secondary hypothyroidism): Isolated TSH deficiency (TSH ẞ subunit gene mutation), pituitary is Thyrotropin-releasing hormone deficiency. Isolated, pituitary stalk interruption syndrome (PSIS), hypothalamic lesion, e,g hamartoma. hormom is releand but rezistent) Thyrotropin-releasing hormone resistance( TRH receptor gene mutation. Hypothyroidism due to deficient transaction factors involved in pituitary development or function. HESXI, LHX3, LHX4, PITI, PROPI gene mutations. Peripheral hypothyroidism: Thyroxin production where Resistance to Thyroid hormone. Thyroid receptor & mutation. Abnormalities of thyroid hormone transport. Allan- Herndon-Dudley syndrome (monocarboxylase transporter 8 (MCT8) gene mutation). Primary Hypothyroidism: Thyroid Dysgenesis: Most Common Cause (80-85%). 33% cases: no thyroid tissue- Agenesis. 64% cases: rudiments are present (Hypoplasia) or ectopic Location. M:F-2:1. Cause: unknown. Can be sporadic or familial. 342 unable to secrete The toy author hormons Some tres TSH dif defcunty (y prolack) at pititary Undu deuclopent 343 Genes Involved: NKX 2.1 (TTF1). FOXE 1 (TTF2) PAX 8. TSHR gene. GNAS (G protein stimulatory alpha subunit). LNKX 2.1: Expressed in thyroid, lung & CNS. Recessive mutations of NKX2.1 gene causes: thyroid dysgenesis, respiratory distress & chorea, ataxia. Despite early treatment. 2. FOXEI: Thyroid dysgenesis, spiky or curly hair, cleft palate. Choanal atresia, bifid epiglottis. BAMFORTH-LAZARUS syndrome. 3. TSHR gene: Elevated TSH levels but dean'i ad on thyroid 50 Ti Ty wil be low 4. GNAS: Pseudohypoparathyroidism Type la. Impaired signaling of the TSH receptor, Dyshormonogenesis: 15% of cases of congenital hypothyroidism. 1 in 30000-50000 live births. Recessive inheritance. GOITRE is almost always present. Types: Defective iodide transport. Pendred syndrome. Defects of iodide organification. Defects of thyroglobulin synthesis. →Defects in deiodination. Figure 1: Goitre in Congenital Hypothyroidism MY NOTES Thyroid development Derivative of foregue outpouching of forgur nar baseren Recom of Il descenas douin and and comes to be thyesid carstage and Thyrotropin reciating hormone (TRH) (polype hormone) secreted from Hypothalamus TSH (glycoprotein) purchas from ant-pitutary TRH and TSH Secretan begins at 10-12 wkI OF GA Thyroglobulin synthess begin at weeks of G Ts & Ty Synther begy at 12 weeks of GA Development and JH migration to Normal Site & mediated by Special transcription factors - NEX2-1, FOXE 1 and PAX 8 maturation of the hypothalamic-pituitary thepsid axis occuo Over the 2nd halt of gestation. but feedback relation an not mature Unta 1-3 monks of postnatal life- Thyroid Hormone Synthesis: Hypothalamic-Pituitary-Thyroid Axis Hypothalam Anterior Pituitary Gland Thyroid Chand ↓ Target Tissues Table 1: Thyroid hormone synthesis Process Step 1. TRH Release Hypothalamus releases TRH onto Anterior Pituitary 2. TSH Release Anterior Pituitary releases TSH onto Thyroid Gland Thyroglobulin Production Iodide Uptake Iodide Oxidation 3. Thyroid Hormone Synthesis Thyroglobulin Jodination MIT/DIT Coupling Thyroglobulin Proteolysis 4. Thyroid Hormone Release Thyroid Gland releases TH; TH circulates in blood Figure 2: Thyroid Hormone Synthesis Structure/Enzyme Involved Hypothalamus Anterior Pituitary Gland Thyroid Follicular Cells Sodium/iodide Symporter Thyroid Peroxidase (TPO) Thyroid Peroxidase (TPO) Thyroid Peroxidase (TPO) Protease ↓ Thyroxine-Binding Globulin (TBG) Thyroid Hormone Synthesis Pathway: Step 1: TSH binds to TSH receptors on thyroid follicular cells, which enhances thyroglobulin production in the follicular cell and release into the colloid of the follicle. Thyroid Hormone Synthesis Circulation -(Jodine) MY NOTES Jardine Jodide() Actten of T While entering cen cytoprasan Teronica Uting Jouthase T-metabolically Dit Tacts is t nucleus where Thyroid hormone produces Thyroid hormone response elemino (TRE) It franscription MRNA synisers of new proteing These new proteks prodie Varous metabol Effects in the Cas Tend to affeer grown, development of cel 344 Figure 3: Steps of Thyroid Hormone Synthesis. Details in the videos PEDIATRIC PULSE-EXAM NOTES ENDOCRINOLOGYHormona Svethesis Pathway Mep 2 7X11 increases the expression and activity of Na+/- Symporters, which increases iodide uptake from the blood into the thyroid follicular cell (lodide Trapping), lodide is transported imo the colloid via Pendrim. MY NOTES Thyrbit Hormone Synthesa H₂OL peroxide Thyroid Hormone Synthesis Pathway: Step 3: Thyroid peroxidase (TPO) oxidizes iodide into iodine (Iodide Oxidation). Thyroid Hormone Synthesis circulation Thyed foltich Colto of FOIECE 3 →→ Relean T 0 (Regulated by Tie) Thyroid Hormone Synthesis Pathway Step 4: Thyroid peroxidase (TPO) places iodine on thyroglobulin tyrosine amino acids (Organification or iodination) to form monoiodotyrosine (MIT) and diiodotyrosine (DIT). Thyroid Hormone Synthesis Jodination: Iothe + tyrosine present in ↓ combines to fom MIT MIT Coupling forms DIT lodide Sodian 345 Thyraid Hormone Synthesis Pathways Step 5: Thyroid perosidase (TPO) combines monoiodotyrosine (MIT) and diiodotyrosine (DIT) to form T3 and 14 (Coupling). Thyroid poruxidase has 3 roles: Oxidation, Jodination, Coupling (3 Stars) Thyroid Hormone Synthesi - Thyroid Hormone Synthesis Pathway: Step 6: Thyroglobulin with 13 and T4 bound to it,re-enters the thyroid follicular cell (Endocytosis) and 13 and T4 are cleaved using lysosomal proteases. Thyroid Hormone Synthesis Thyroid Hormone Synthesis Pathway: Step 7: 13 and T4 are released into the bloodstream where they act on target tissues. Most T3 and T4 is bound to thyroxine-binding globulin (TBG). 70-1. of Ty 50% of Ts Cliculating are bound to TBS 30% of Ti $ του of are bound to Albumin and/or pre albumin (Transthyretio) 346 Thyroid Hormone Synthesis Todide MY NOTES D2T+H27 about 11 to the Co receptor 210-12サッ greater affinity then Je of Ty it second by periphenet teve fo Using Jodotyrosine detodinase Type 112 This de Jodinen Conven active Brain (particulary Fitentary gland metabolically acha nem rich in Type 2 deod Entry of Ty and Ty in to car is fecititated by specifi thyroid hormone transporice sep cip. Mono Carboxylate Transpone (MCT-8) TBG is thyroid Tran protein which is predict by liver which came and back to 7, TGT ng protein e hormone levels inlood Free Tu-0-054 Free -0.3 Defective lodide Transport: MY NOTES Very rare disorder. Crused by mitations in sodium-indide symporter (NIS). Responsible for concentrating indide in thyroid gland NIS symporter Found in salivary gland also. Common in Japan. Uptake of radio iodine & pertechnetate is LOW This condition responds to large doses of potassium lodide, but Jevothyroxine is preferred. Pendred Syndrome: AR Sensorineural Deafness & Goiter. hypothymiduam Mutations in Pendringene. MOA: responsible for chloride iodide transport. PENDRIN transports iodide into the colloid, results in organification. Some patients only have deafness, normal thyroid dysfunction. Defects of lodide Organification: Most common type of thyroid hormone defect. TPO requires locally generated H₂O; & hematin (co factor) for organification. Marked discharge of radioactivity 2 hours after administration (40-90% as opposed to <10% in normal). Enzyme DUOX2 produces H₂O; DUOX 2 mutations cause permanent/transient hypothyroidism. 4.Defects of Thyroglobulin Synthesis: Goiter+. [TSH raponsible for Thyroglobulin synthers in the cal They also present & gaster] 5. Defects in deiodination: ⚫lodotyrosine deiodinase enzyme defect. Causes halt in peripheral conversion of Ty to Ty 6.Defects in thyroid hormone transport: Transport of thyroid hormone into cell facilitated by: MCTS. Thyrotropin Receptor Blocking Antibodies: 2% of cases of congenital hypothyroidism. Transplacentally acquired. PEDIATRIC PULSE-EXAM NOTES MY NOTES h/o maternal auto immune thyroiditis, similar h/o in siblings. USG: small thyroid. Radio iodine uptake: nil. Serum thyroglobulin level: LOW. Rx: levothyroxine. Spontaneous remission in 3-6 months. Radio Iodine Administration: Radio iodine mistakenly administered during pregnancy to mother. Fetal thyroid actively traps lodine by 70-75 days of gestation. Hence, iodine administration in women of child bearing age should be done after ruling out pregnancy. Iodine Exposure: Mothers taking excessive iodine (>12mg/day) as nutritional supplements or seaweed. Drugs Containing Iodine- amiodarone. It's a TRANSIENT phenomenon-resolves after discontinuation. Goiter+ Iodine Deficiency (Endemic Goiter): Most common cause of congenital hypothyroidism worldwide. RDA of lodine: 150micg/day. RDA during Pregnancy: 220 micg/day. Iodine deficiency in mothers cause: congenital hypothyroidism. Figure 4: Endemic Goitre Central (Secondary) Hypothryoidism: Developmental defects of pituitary or hypothalamus. 1 in 30000 LB. 75% of cases have multiple endocrine deficiencies. Either TSH deficiency or TRH receptor mutation. Various genes involved. Genes Involved: POUIFI mutation: deficiency of TSH + GH + Prolactin. PROPI mutation: deficiency of TSH + GH + Prolactin + FSH + LH. 348 ENDOCRINOLOGY HESXI mutation deficiency of TSH OH Prolactin + ACTH MY NOTES Inst) mutation: isolated TSH deficiency. Thyroid function in preterm & LBW: Postnatal TSH surge is less & Total serum T4 levels become normal by weeks of life: but FT4 is normal. Reasons: Immaturity of Hypothalamic-pituitary-thyroid axis. Maternal contribution of thyroid hormone is less. Illnesses needing steroids, dopamine. Clinical Features: of congenital Hypogeitum Asymptomatic at birth even in severe cases. Due to the transplacental transfer of maternal T4. Only identified through newborn screening program (TSH & T4 levels). Birth weight & length: Normal. Head size: mild increase (myxedema of brain). Posterior Fontanelle: >5mm. Prolonged jaundice (indirect). Sluggish cry. protruded tongu ↑ Feeding difficulties- macroglossia, choking spells. Respiratory difficulties- noisy respiration, nasal obstruction, apneic spells. Figure Sa: Newborn Screening for TSH & T4 Umbilical hernia is allo cean Constipation not responding to treatment. Sub normal temperature <35degree C. (Hypo-thermia) Systone teaturi CVS: cardiomegaly, heart murmurs, asymptomatic pericardial. effusion. Genital edema & edema of extremities. Slow Pulse. cold peripheries all thypothermin Macrocytic anemia. Hearing loss. Figure 5c: Features of Congenital Hypothyroidism If not treated at once, physical & mental development decreases. Short stature, short extremities, broad nasal bridge, swollen eyelids. Open mouth, delayed dentition, macroglossia. Newborn thyasd screening I establluted for all newborns world ande at 48 to 72 hor (DOL) Both TSt and Ty levels are coded to check Why on IDOL Tote am advised? dit gransplacental Tronifer of maremal Tu Figure 5b: Prolonged Jaundice If not diagnond and Reed Systemic symptoms stads Showing like cus INON PEDIATRIC PULSE-EXAM NOTES ENDOCRINOLOGY Short & thick neck. MY NOTES Fat deposits between neck & shoulders, Buffale homp Dry & scaly skin with little perspiration. General pallor with sallow complexion. Myxedema of eyelids, back of hands & external genitalia. Coarse, brittle & scanty hair. Hairline reaches far down on forehead. Development: Delay in both gross & fine motor. Lethargic infants. Hoarse voice. Speech delay. Sexual maturation is delayed. Thu seen in Chronically untreated congenital hypothymic Kocher-Debre-Semelaigne Syndrome: Usually muscles are hypotonic. Affected older children can have an athletic appearance. Generalized pseudo-hypertrophy. Particularly calf muscles. Males more common. Figure 6: Kocher-Debre-Semelaigne Syndrome Ectopic Thyroid: Produce normal thyroid levels for a variable period of time. So, remain euthyroid. Surgical removal results in hypothyroidism. Lab Findings: Newborn Screening. Day 2-5, heel prick method. Mostly, TSH measurement is done. Figure 7: Ectopic Thyroid Jdcally TSH and Ty levels should be accused Disadvantages: central hypothyroidism & some cases of primary congenital hypothyroidism. Some centers: measure T4 first, if its low then TSH is measured. 350 Normal Age Specific Values: MY NOTES Table 2 Age TSH (alU/mL) T4 (pg/dL) T3 (ng/dL) Free T4 1.0-17.4 7.4-13.0 15-75 (ng/dL) Cord blood 4 days 1.0-39.0 14.0-28.4 100-740 2.2-5.3 0.9-22 220 weeks 1.7-9.1 7.2-15.7 105-245 4.24 months 0.8-8.2 7.2-15.7 0923 105-269 0.8-1.8 2.7 years 0.7-5.7 6.0-14.2 94-241 1.0-2.1 9.20 years 0.7-5.7 4.7-12.4 80-210 0.8-1.9 21-45 years 0.4-4.2 5.3-10.5 70-204 0.9-2.5 TRH TSH secretion by activethadone Thyroid Gland Thyroid Specific Antibodies ↑ ↑ ↓ + ↓ - Thyroid Hormones ↓ ↓ Free T4 and T3 Figure 8: Primary & Secondary Hypothyroidism At Risk Groups: LBW. Prematurity. Trisomy