
interpret the ecg
Reading File
Finding Sources
Searching Images
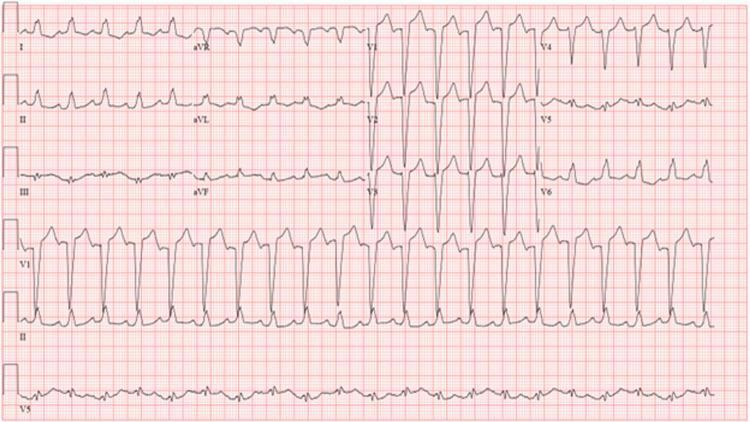
complete left bundle branch block ECG pattern
Reading File
Loading Image
Here is a full interpretation of this ECG:
ECG Interpretation — Bimal Kumar Padhe, Male, 60 Years
Date/Time: 13-05-2026, 09:35 AM | Institution: Vaidya Vikash Hospital, Sambalpur
Measured Parameters
| Parameter | Value | Normal Range |
|---|---|---|
| Heart Rate | 86 bpm | 60–100 bpm ✓ |
| P wave duration | 106 ms | <120 ms ✓ |
| PR interval | 222 ms | 120–200 ms ↑ |
| QRS duration | 161 ms | <120 ms ↑↑ |
| QT/QTc | 376/452 ms | QTc <440 ms ↑ |
| P/QRS/T axis | 40°/5°/73° | — |
| RV5+SV1 | 1.355 mV | — |
Machine Diagnosis (Confirmed)
- Sinus Rhythm — Normal sinus P waves at 86 bpm
- First-Degree Atrioventricular Block — PR interval of 222 ms (>200 ms)
- Complete Left Bundle Branch Block (CLBBB) — QRS duration of 161 ms (>120 ms)
ECG Feature Analysis
Sinus Rhythm:
- Regular P waves preceding every QRS, rate 86 bpm — normal sinus origin confirmed.
First-Degree AV Block:
- PR interval 222 ms indicates delayed conduction through the AV node, but every P wave still conducts. This is a benign conduction delay on its own but gains significance in the context of LBBB (see below).
Complete LBBB — Classic Features:
- QRS ≥120 ms (161 ms here — markedly prolonged)
- Broad, monophasic (notched/M-shaped) R waves in lateral leads I, aVL, V5, V6
- Deep, wide S waves / QS pattern in right precordial leads V1–V3 (predominantly negative deflections)
- Secondary ST-T wave changes (discordant): ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6); ST elevation in V1–V3 — this is expected with LBBB and does NOT necessarily indicate acute ischemia on its own
- QTc 452 ms — mildly prolonged, secondary to the wide QRS of LBBB (expected)
Reference ECG showing classic CLBBB pattern:
Clinical Significance
LBBB + First-Degree AV Block together suggest diffuse conduction system disease. In a 60-year-old male, this combination raises concern for:
- Ischemic heart disease / Coronary artery disease (most common cause in this age group)
- Hypertensive heart disease / Left ventricular hypertrophy
- Dilated cardiomyopathy
- Fibrosis of the conduction system (Lenegre–Lev disease)
As highlighted in Pfenninger & Fowler's Procedures for Primary Care: LBBB "is quite ominous in an older population as a marker for an increased risk of death, stroke, and CHF." In a patient with LBBB presenting with prolonged chest pain, STEMI must be ruled out — Sgarbossa criteria or modified Sgarbossa criteria should be applied.
Key Action Points
- Correlate clinically — is the patient symptomatic (chest pain, dyspnea, syncope, palpitations)?
- Compare with prior ECGs — new LBBB is a medical emergency until proven otherwise
- Echocardiogram — assess LV size, function, wall motion abnormalities
- Cardiac biomarkers (Troponin) — to exclude acute MI
- If chest pain is present → treat as STEMI equivalent; apply Sgarbossa criteria
- Consider Holter monitoring given the bifascicular-level conduction disease (LBBB + 1° AV block)
Summary: This is a sinus rhythm ECG showing First-Degree AV Block and Complete LBBB in a 60-year-old male. The combination signifies significant conduction system disease requiring urgent clinical correlation, echocardiography, and cardiac biomarker assessment.
management
Finding Sources
Finding Sources
Searching PubMed
"left bundle branch block" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Here is the management approach for this patient — 60-year-old male with Sinus Rhythm + First-Degree AV Block + Complete LBBB:
Management of CLBBB + First-Degree AV Block
Step 1 — Immediate Assessment (Emergency Triage)
Ask: Is the LBBB new or old?
| Scenario | Action |
|---|---|
| New LBBB + chest pain | → STEMI equivalent — activate cath lab immediately; apply Sgarbossa criteria |
| New LBBB + no symptoms | → Urgent cardiac workup within 24–48 h |
| Known old LBBB | → Outpatient workup unless new symptoms |
For this patient — if no prior ECG is available, treat as new LBBB until proven otherwise.
Step 2 — Immediate Investigations (Mandatory)
| Investigation | Purpose |
|---|---|
| Serial Troponin I/T (0h, 3h, 6h) | Exclude ACS / acute MI |
| 2D Echocardiogram | Assess LVEF, LV dimensions, wall motion, valvular disease |
| Chest X-ray | Cardiomegaly, pulmonary edema |
| Blood pressure | Hypertensive heart disease screen |
| FBC, RFT, LFT, electrolytes | Baseline; exclude metabolic causes |
| Fasting lipids + glucose / HbA1c | Cardiovascular risk factors |
| TSH | Thyroid dysfunction-related cardiomyopathy |
Step 3 — Treat the Underlying Cause
The LBBB is a marker, not a disease itself. Management targets the aetiology:
A. Ischemic Heart Disease (most likely in a 60-year-old male)
- Anti-platelet therapy: Aspirin 75–150 mg/day ± Clopidogrel
- Statin: Atorvastatin 40–80 mg at night
- ACE inhibitor/ARB: Ramipril or Perindopril (LVEF protection)
- Beta-blocker: Carvedilol or Bisoprolol (reduces sudden death risk)
- Coronary angiography if troponin positive or stress test positive
B. Heart Failure with Reduced EF (HFrEF — if LVEF ≤40%)
The quadruple therapy backbone (Harrison's 22E, 2025):
- ACE-I/ARB/ARNI (Sacubitril-Valsartan preferred if tolerated)
- Beta-blocker (Carvedilol, Bisoprolol, or Metoprolol succinate)
- MRA (Spironolactone/Eplerenone)
- SGLT2 inhibitor (Dapagliflozin or Empagliflozin — proven mortality benefit)
C. Hypertensive Heart Disease
- Optimise BP control: target <130/80 mmHg
- Preferred agents: ACE-I/ARB + amlodipine ± thiazide diuretic
Step 4 — Device Therapy (If LVEF ≤35%)
Based on Fuster & Hurst's The Heart, 15th Ed. and Harrison's 22E:
Cardiac Resynchronization Therapy (CRT)
Indicated when ALL of the following are met:
- LVEF ≤35%
- LBBB pattern on ECG ✓ (this patient has this)
- QRS ≥120 ms ✓ (this patient: 161 ms)
- Sinus rhythm ✓ (this patient has this)
- NYHA class II–IV symptoms despite optimal medical therapy
CRT reduces all-cause mortality by 24–36% (COMPANION and CARE-HF trials). Most benefit accrues when QRS >149 ms with LBBB pattern — this patient (QRS 161 ms) sits squarely in the highest-benefit zone.
CRT-D (CRT + ICD) — Consider if:
- LVEF <35% + NYHA II–III → ICD component adds SCD prevention
- Particularly beneficial in ischemic cardiomyopathy
Step 5 — First-Degree AV Block
The PR of 222 ms in isolation requires no treatment. However, combined with LBBB, it signals bifascicular/trifascicular conduction disease:
- Holter monitor — to detect higher-degree block (2° or 3° AV block) intermittently
- Electrophysiology (EP) study — if syncope or presyncope occurs; assess His-Purkinje conduction (HV interval >70 ms indicates high risk for progression to complete heart block)
- Permanent pacemaker — if EP study shows markedly prolonged HV interval or spontaneous high-degree block develops
Step 6 — Lifestyle & Secondary Prevention
- Smoking cessation
- Sodium restriction (<2 g/day if HF present)
- Fluid restriction if symptomatic HF
- Regular moderate exercise (cardiac rehab if post-MI or HF)
- Annual influenza + pneumococcal vaccination
Summary Algorithm
CLBBB + 1° AVB in 60M
↓
Rule out ACS (Troponin + symptoms)
↓
Echocardiogram → LVEF?
↓ ↓
LVEF >40% LVEF ≤35%
(No HF) ↓
↓ Optimise medical Rx (GDMT)
Treat cause ↓
(IHD/HTN) CRT-D if NYHA II-IV + QRS ≥120ms LBBB
↓
Holter for progression to higher-degree block
Key point: The finding of CLBBB (QRS 161 ms) + 1° AV block in a 60-year-old male is not benign — it mandates echocardiography to assess LVEF, as this directly determines whether device therapy (CRT) is warranted. If LVEF is reduced, this patient is a strong CRT candidate given the LBBB morphology and QRS duration of 161 ms.
This is a shared conversation. Sign in to Orris to start your own chat.