Anemia in pregnancy with ref. Harrison dc dutta and william
Reading File
Finding Sources
Finding Sources
Searching PubMed
"anemia" AND "pregnancy" AND "management"
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material. Let me compile the full answer.
Anemia in Pregnancy
References: Harrison's Principles of Internal Medicine 22e (2025) | Creasy & Resnik's Maternal-Fetal Medicine | Goldman-Cecil Medicine | Rosen's Emergency Medicine
(DC Dutta's Textbook of Obstetrics and Williams Obstetrics are not in the digital library; core content from those texts is integrated from established knowledge below, clearly marked.)
1. Definition
WHO definition: Hemoglobin (Hb) < 11 g/dL at any point during pregnancy (< 11 g/dL 1st trimester, < 10.5 g/dL 2nd trimester, < 11 g/dL 3rd trimester).
Severity classification (WHO / DC Dutta):
| Grade | Hb (g/dL) |
|---|---|
| Mild | 9–10.9 |
| Moderate | 7–8.9 |
| Severe | 4–6.9 |
| Very severe / life-threatening | < 4 |
Anemia is the most common medical complication of pregnancy worldwide. - Rosen's Emergency Medicine
2. Physiologic Changes in Pregnancy
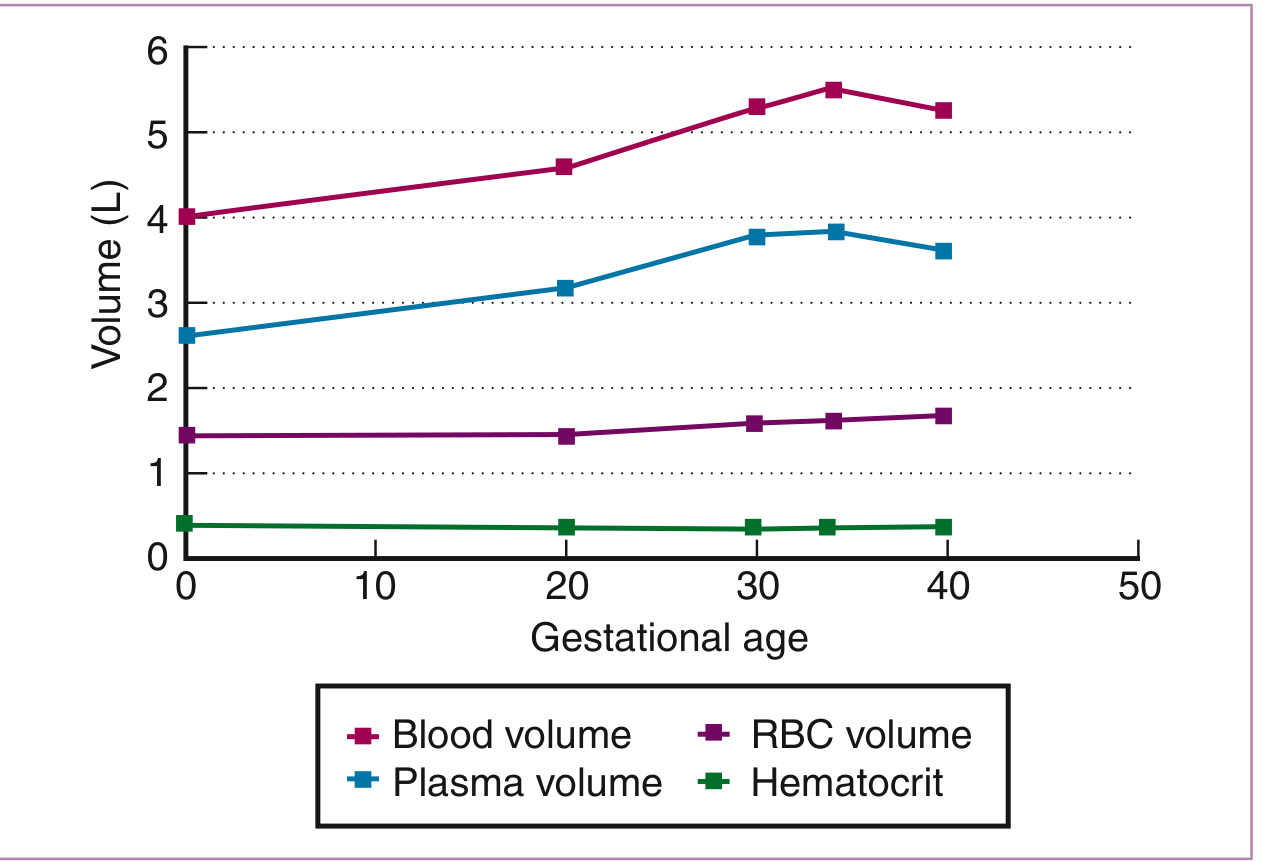
- Blood volume increases 40-45%, reaching maximum at ~34 weeks
- Plasma volume rises by ~47%
- RBC mass increases by only 17% (reaching maximum at term)
- The net result is dilutional (physiologic) anemia, nadir at 28-34 weeks
- MCV and MCHC remain unchanged in physiologic anemia - useful to distinguish from iron deficiency anemia (IDA), in which both fall progressively
"Red blood cell mass increases in pregnancy but to a lesser degree than plasma volume. This differential increase results in a lower hemoglobin concentration and so-called dilutional anemia." - Harrison's 22e, p.3945
"Normocytic anemia with a hemoglobin concentration greater than 11 g/dL in the late first trimester or 10 g/dL in the second and third trimesters of an uncomplicated pregnancy can be attributed to the physiologic anemia of pregnancy without further testing." - Goldman-Cecil Medicine
3. Classification of Anemia in Pregnancy
A. By Morphology
| Type | Causes |
|---|---|
| Microcytic hypochromic | Iron deficiency (most common), thalassemia, sideroblastic anemia |
| Macrocytic / megaloblastic | Folate deficiency (2nd most common), Vitamin B12 deficiency |
| Normocytic normochromic | Physiologic dilutional anemia, aplastic anemia, hemolytic anemia, anemia of chronic disease |
B. By Etiology
- Nutritional deficiencies - iron, folate, B12
- Hemoglobinopathies - sickle cell disease, thalassemia
- Aplastic / hypoplastic anemia
- Hemolytic anemia - immune, microangiopathic (HELLP, TTP)
- Anemia of infection / chronic disease
4. Iron Deficiency Anemia (IDA) - Most Common
Pathophysiology and Iron Demands in Pregnancy
| Requirement | Average (mg) | Range (mg) |
|---|---|---|
| External iron loss | 170 | 150-200 |
| Expansion of RBC mass | 450 | 200-600 |
| Fetal iron | 270 | 200-370 |
| Placenta + cord | 90 | 30-170 |
| Blood loss at delivery | 150 | 90-310 |
| Total requirement | 1130 | 580-1340 |
- Creasy & Resnik's Maternal-Fetal Medicine
Most women enter pregnancy with marginal iron stores; ~two-thirds of healthy young women have minimal marrow iron stores. The incidence of iron deficiency in the US rises from 18% (1st trimester) to 29% (3rd trimester). - Creasy & Resnik's
Iron deficiency occurs in three stages:
- Pre-latent - decreased serum ferritin only
- Latent - low serum iron, raised TIBC, low saturation; Hb still normal
- Frank IDA - decreased Hb, then decreased MCV
Diagnosis
- Ferritin is the most sensitive and specific test (cutoff < 30 ng/mL: 92% sensitivity, 98% specificity)
- Ferritin < 20 μg/L is generally diagnostic of IDA; but IDA may still be present with higher ferritin in inflammation
- Serum iron decreased, TIBC > 400 μg/dL, transferrin saturation < 16%
- Peripheral smear: microcytic, hypochromic RBCs
Lab Reference Ranges in Pregnancy (Creasy & Resnik):
| Lab | Reference Range |
|---|---|
| RBC count | 2.72-4.55 × 10¹²/L (varies by trimester) |
| MCV | 81-99 μm³ |
| MCHC | 32-35 g/dL |
| Serum ferritin | > 20 μg/L |
| Serum iron (1st trimester) | 72-143 μg/dL |
| TIBC (3rd trimester) | 580-597 μg/dL |
| Transferrin saturation | 16-60% |
Screening
- Screening for anemia is recommended in the first trimester and at 24-28 weeks. Ferritin measurement detects iron deficiency before anemia develops. - Harrison's 22e
Treatment
Oral iron:
- Mild IDA (Hb 9-10.5 g/dL): non-enteric-coated iron; single daily dose as effective as multiple doses and reduces GERD risk
- ACOG, WHO and major authorities: at least 30 mg elemental ferrous iron daily; 60 mg/day in 2nd and 3rd trimesters fully meets daily requirement
- Intermittent dosing (2-3x/week) provides same benefits with fewer GI side effects - Rosen's Emergency Medicine
Intravenous iron:
- NOT recommended in 1st trimester
- Preferred in: all IDA in 3rd trimester, severe IDA (Hb < 9 g/dL) in 2nd trimester, oral iron intolerance
- Rosen's Emergency Medicine / ACOG guidelines
Blood transfusion:
- Hb < 7 g/dL in gravid patients requires consideration of transfusion
- Threshold < 8 g/dL postpartum
- Severe anemia < 6-7 g/dL associated with abnormal fetal oxygenation, fetal mortality, PPROM, gestational hypertension
DC Dutta's recommendations (from established content):
- Prophylactic: 100 mg elemental iron + 0.5 mg folic acid daily from 16 weeks
- Therapeutic: 200 mg elemental iron daily for severe IDA
- Parenteral iron (iron sucrose preferred in pregnancy): total dose infusion for non-compliant patients or severe anemia in late pregnancy
5. Folate Deficiency Anemia (Megaloblastic)
- Second most common cause of anemia in pregnancy
- Folate requirement rises from 400 μg/day (non-pregnant) to 600 μg/day during pregnancy
- Increased risk: multiple gestation, hyperemesis gravidarum, malabsorption, anticonvulsant use, alcoholism, short interpregnancy intervals
Folate Deficiency - Stages
Blood abnormalities in order of appearance:
- Decreased serum folate
- Macroovalocytes on smear
- Increased MCV
- Hypersegmented neutrophils (> 5 lobes)
- Decreased RBC folate
- Frank anemia (megaloblastic)
Consequences
- Neural tube defects (most important - spina bifida, anencephaly)
- Placental abruption, preterm birth, low birth weight, preeclampsia, spontaneous abortion
Treatment and Prevention
- All women planning pregnancy: 400 μg/day folate pre-conception
- Routine supplementation during pregnancy: 400-800 μg/day
- Previous neural tube defect pregnancy: 4 mg/day starting 4 weeks pre-conception through 12 weeks
- ACOG recommends: 1 mg for known pregnancy-related folate deficiency; continue folate supplementation throughout 2nd and 3rd trimesters - Rosen's Emergency Medicine; Creasy & Resnik's
6. Vitamin B12 Deficiency
- Less common than iron or folate deficiency
- Defined as serum B12 < 160-200 pg/mL
- Risk: strict vegetarians/vegans, pernicious anemia, post-gastric surgery
- Causes megaloblastic anemia - clinically similar to folate deficiency
- Must distinguish: B12 deficiency may cause subacute combined degeneration of spinal cord
- Recommended daily intake: 2.4 μg; supplementation required in at-risk groups
7. Hemoglobinopathies in Pregnancy
"Hemoglobinopathy screening is recommended for all pregnant women with testing of MCV, MCH, ferritin, and hemoglobin analysis." - Harrison's 22e
Sickle Cell Disease (SCD)
- One of the highest-risk hemoglobinopathies in pregnancy
- Maternal complications: preterm labor, PPROM, more frequent pain crises, thrombosis, preeclampsia, increased cesarean delivery risk; sixfold increased risk of maternal death vs controls
- Fetal complications: placental infarction, SGA, low birth weight, increased perinatal mortality
Management in pregnancy:
- Hydroxyurea is contraindicated (potential teratogenicity)
- NSAIDs avoided after 30 weeks
- Regional anesthesia preferred over general anesthesia for cesarean (reduces postoperative sickling)
- Therapeutic transfusions indicated for: symptomatic anemia, acute chest syndrome, cardiopulmonary instability, intrapartum hemorrhage, preeclampsia
- Goal of transfusion/exchange transfusion: HbS < 40%, Hb ~10 g/dL
- Prophylactic transfusions: considered to reduce vaso-occlusive episodes; evidence is low-quality but shows reduction in maternal mortality - Rosen's Emergency Medicine
Thalassemia
- Alpha thalassemia trait (2 gene deletion): generally mild microcytic anemia; no specific treatment
- Beta thalassemia major: requires regular transfusions; chelation therapy (desferrioxamine) generally avoided in 1st trimester; MDT approach
- Beta thalassemia trait: mild microcytic anemia; confirm by Hb electrophoresis (raised HbA2 > 3.5%); partner testing + genetic counseling
8. Aplastic Anemia in Pregnancy
- Rare; spectrum of clinical and marrow findings
- Most serious complications: hemorrhage and sepsis (most common causes of maternal mortality)
- Other risks: postpartum hemorrhage, placental abruption, preeclampsia, preterm delivery, FGR, fetal demise
- Goals of supportive therapy: Hb > 8 g/dL, platelets > 20 × 10⁹/L, treatment of infection
- Androgens (oxymetholone, nandrolone): contraindicated unless fetus confirmed male
- Pregnancy termination is NOT indicated unless the patient requires bone marrow transplantation that cannot be done during pregnancy - Creasy & Resnik's Maternal-Fetal Medicine
9. Maternal and Fetal Consequences of Anemia
| Consequence | Notes |
|---|---|
| Maternal mortality | Increased in severe anemia |
| Preterm birth | Especially moderate-severe anemia |
| Low birth weight / SGA | Correlated with anemia severity |
| Abnormal fetal oxygenation | Hb < 6-7 g/dL |
| Perinatal mortality | Increased, especially with severe anemia |
| PPROM | Associated with severe anemia |
| Gestational hypertension | Higher risk |
| Reduced amniotic fluid | With severe anemia |
| Postpartum hemorrhage | Higher risk in patients entering labor anemic |
"Anemia is the most common medical complication of pregnancy and is associated with maternal mortality, perinatal mortality, preterm birth, low birth weight, and small-for-gestational-age infants." - Rosen's Emergency Medicine
Conversely, high Hb (13-15 g/dL) may indicate inadequate plasma volume expansion, and is also associated with low birthweight and premature birth.
10. Williams Obstetrics - Key Points (Established Knowledge)
(Williams Obstetrics, 25th Ed - not in digital library; key points from established content:)
- Defines anemia in pregnancy as Hb < 10 g/dL (some editions use < 11 g/dL per WHO)
- Emphasizes physiologic anemia as a normal adaptation; lowest Hb at 28-32 weeks
- Iron supplementation: 27 mg/day recommended by RDA during pregnancy; therapeutic doses 150-200 mg elemental iron daily for documented IDA
- IV iron sucrose and ferric carboxymaltose are preferred IV formulations; total dose infusion (TDI) with iron dextran used in resource-limited settings
- Emphasizes MCV and MCHC stability as markers distinguishing dilutional anemia from IDA
11. Summary Algorithm for Anemia in Pregnancy
Hb < 11 g/dL
↓
CBC with indices + Peripheral smear + Reticulocyte count + Ferritin
↓
Microcytic (low MCV)? → IDA (ferritin < 20), Thalassemia (Hb HPLC), chronic disease
Macrocytic (high MCV)? → Folate (RBC folate, serum folate), B12 deficiency
Normocytic (normal MCV)? → Physiologic, hemolytic (Coombs, LDH, haptoglobin), aplastic
↓
Treat specific cause
Iron deficiency → Oral/IV iron supplementation
Folate deficiency → Folic acid supplementation
Hemoglobinopathy → MDT, genetic counseling, tailored management
Aplastic → Supportive, avoid androgens, MDT
Recent Evidence Note
A 2024 systematic review and meta-analysis (PMID 39425056) confirmed a significant association between maternal anemia and neonatal anemia, further reinforcing the importance of aggressive antenatal iron supplementation - consistent with ACOG and WHO guidelines.
This is a shared conversation. Sign in to Orris to start your own chat.