In detail about all surgical approach to hip
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Campbell's Operative Orthopaedics 15th Ed and Miller's Review. Here is the detailed, organized answer:
Surgical Approaches to the Hip
The hip can be accessed from four main directions: anterior, anterolateral, lateral, posterior, and medial. Each exploits specific intermuscular/internervous planes and carries distinct neurovascular risks. Below is a systematic account of all major approaches.
1. ANTERIOR APPROACHES
1a. Smith-Petersen (Anterior Iliofemoral) Approach
Position: Supine, with a sandbag under the affected hip.
Interval:
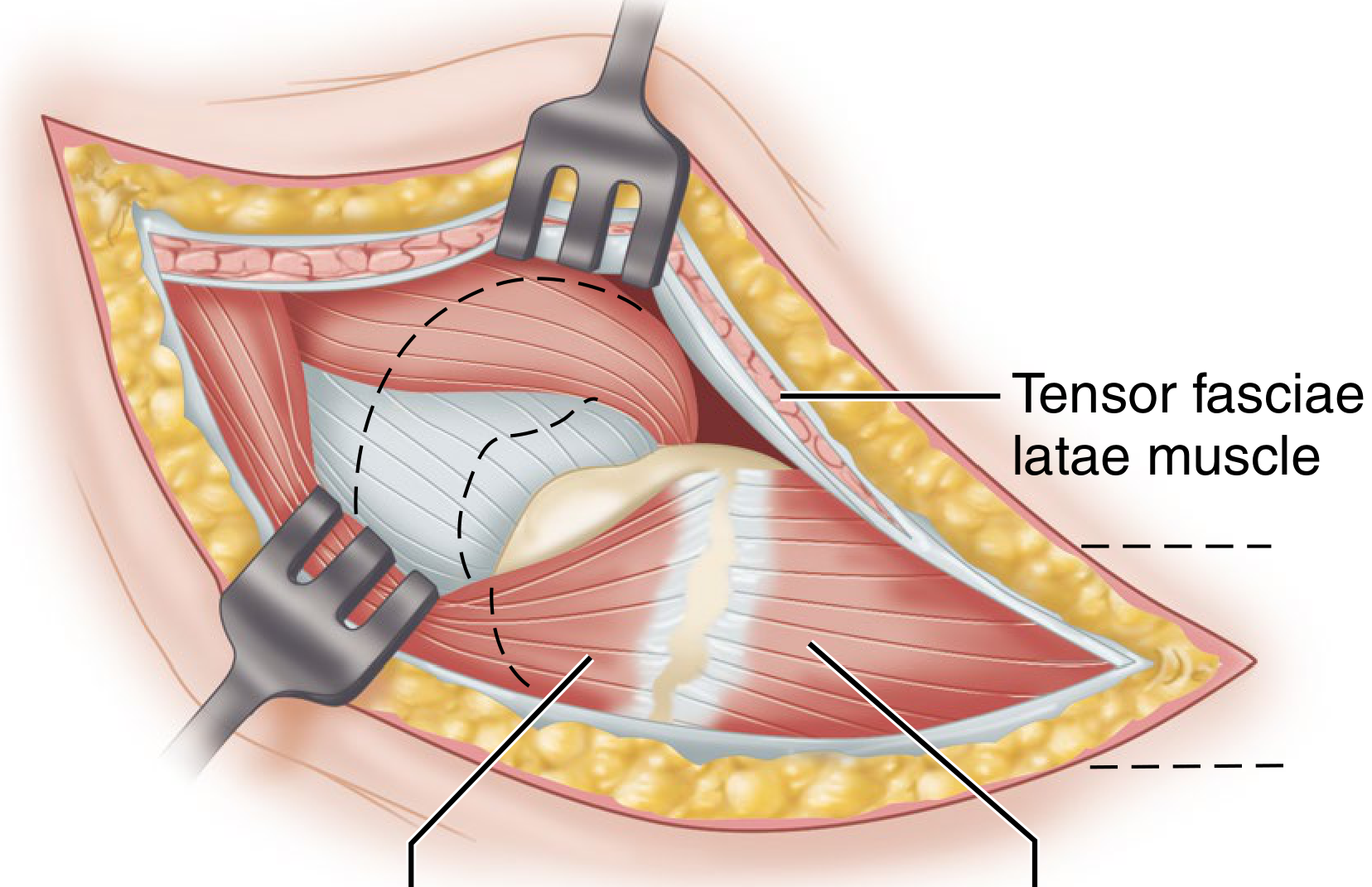
- Superficial: between sartorius (femoral nerve) and tensor fasciae latae / TFL (superior gluteal nerve)
- Deep: between rectus femoris (femoral nerve) and gluteus medius (superior gluteal nerve)
- This is a true internervous plane
Incision: Begins at the iliac crest and curves distally and anteriorly toward the anterior superior iliac spine (ASIS) and then distally to the lateral border of the patella.
Steps:
- Incise fascia along the anterior border of the TFL
- Locate and protect the lateral femoral cutaneous nerve (LFCN), which lies medial to the TFL border, close to the sartorius
- Reflect abductors (gluteus medius, minimus, TFL) subperiosteally from the iliac wing to the capsule
- Divide attachments of rectus femoris (straight and reflected heads)
- Perform capsulotomy to expose the femoral head and neck
Structures at risk:
- LFCN (injury causes meralgia paresthetica) - most common complication
- Ascending branch of the lateral femoral circumflex artery (LFCA) - ligated during approach; descending branch may be injured with excessive distal reflection
- Femoral nerve and artery - avoid aggressive medial retraction of sartorius
- Superficial iliac circumflex artery penetrates TFL just anterior to LFCN
Uses: Open reduction of CDH, femoral neck fractures, hip arthroplasty, labral repair, osteotomies.
1b. Anterior Approach Using a Transverse Incision (Somerville)
Designed specifically for irreducible congenital dislocation of the hip (CDH) in young children.
Incision: Transverse "bikini" incision - inferior and medial to the ASIS, coursing obliquely superiorly and posteriorly to the iliac crest midpoint.
Sequential steps required:
- Psoas tenotomy
- Complete medial capsulotomy including the transverse acetabular ligament
- Excision of hypertrophied ligamentum teres
- Reduction of femoral head into the true acetabulum
1c. Direct Anterior Approach (DAA) / Smith-Petersen Distal Half (Light and Keggi, 1980)
The DAA uses the distal half of the traditional Smith-Petersen approach and has grown substantially in popularity for total hip arthroplasty (THA).
Position: Supine on a radiolucent table or specialized fracture table. Allows intraoperative fluoroscopy for implant positioning.
Interval: Both intermuscular and internervous - requires minimal muscle dissection.
Advantages:
- True internervous plane (no muscle detachment)
- Supine position gives more reliable pelvic orientation
- Intraoperative fluoroscopy feasible
- Faster recovery in some studies
Limitations:
- Cannot be safely extended distally - a separate exposure needed for osteotomy, implant removal, or cerclage
- More difficult femoral canal access, especially in wide iliac crest, short varus neck, or obese patients
- Significant learning curve; cadaver lab training recommended
1d. Modified Anterolateral Iliofemoral Approach (Smith-Petersen Modification)
Retains advantages of the anterior iliofemoral approach while also exposing the trochanteric region laterally - useful for open reduction and internal fixation of femoral neck fractures.
Capsular incision: Begins on the inferior capsule just lateral to the labrum, extends parallel to the labrum to the superior capsule, then curves laterally past the capsule to the base of the greater trochanter, dividing the reflected head of the rectus femoris.
2. LATERAL APPROACHES
2a. Watson-Jones Lateral Approach (Anterolateral Approach)
Position: Lateral decubitus.
Interval: Between TFL and gluteus medius - no true internervous plane, but an intermuscular one.
Incision: Slightly curved, centered over the greater trochanter.
Steps:
- Split the fascia lata to expose the vastus lateralis
- Separate TFL from gluteus medius (coarse fiber direction of gluteus medius helps distinguish the two)
- Detach the anterior third of the gluteus medius tendon from the trochanter and the entire gluteus minimus
- Dissect the reflected head of the rectus femoris medially to gain capsule access
Structures at risk:
- Superior gluteal nerve - passes ~5 cm above acetabular rim; injury denervates TFL; split must stay <5 cm proximal to trochanter
- Femoral nerve and artery with excessive medial retraction
- LFCA descending branch with anterior and inferior dissection
Uses: Femoral neck fractures, arthroplasty, hip arthrotomy.
Campbell's tip: Begin the gluteus medius/TFL separation midway between the ASIS and the greater trochanter before TFL blends with its fascial insertion. For wider field, detach the anterior gluteus medius tendon fibers or reflect the anterosuperior trochanter with an osteotome.
2b. Hardinge (Lateral / Direct Lateral) Approach
Interval: Splits the gluteus medius and vastus lateralis in tandem through the greater trochanter.
Steps:
- Incise skin and fascia lata to expose gluteus medius and vastus lateralis
- Incise gluteus medius from the greater trochanter, leaving a cuff and the posterior half to two-thirds attached
- Extend the incision to split the gluteus medius proximally
- Split the vastus lateralis distally along its anterior fourth to the femoral shaft
- Detach the gluteus minimus from its insertion to expose the capsule
Structures at risk:
- Superior gluteal nerve if gluteus medius split goes >5 cm proximal to the greater trochanter
- LFCA (transverse branch)
Uses: Total hip arthroplasty, revision hip surgery. Low dislocation rate compared to posterior approach.
2c. Lateral Approach for Extensive Exposure (Harris Trochanteric Approach)
Provides the most extensive lateral exposure, allowing dislocation of the femoral head both anteriorly and posteriorly.
Position: Unaffected hip down, affected hip elevated 60 degrees, supported by sandbags.
Key feature: Requires osteotomy of the greater trochanter.
Steps (simplified):
- U-shaped skin incision with base at the posterior trochanter border
- Divide iliotibial band proximal to the greater trochanter
- Incise fascia lata one fingerbreadth anterior to the gluteus maximus insertion
- Osteotomize the greater trochanter and retract superiorly with gluteus medius and minimus
- Divide piriformis, obturator externus, obturator internus at their trochanteric insertions
- Full circumference of femoral head exposed by placing trochanter/muscle pedicle in the acetabulum and externally rotating the femur
- Entire acetabulum exposed by retracting the trochanter superiorly
Risks: Higher risk of heterotopic ossification after THA vs direct lateral. Risk of trochanteric nonunion or bursitis.
2d. McFarland and Osborne Approach (Lateral Preserving Gluteus Medius)
Treats the gluteus medius and vastus lateralis as functionally continuous through the trochanteric periosteum.
Key steps:
- Midlateral incision centered over the greater trochanter
- Divide gluteal fascia and iliotibial band in a straight midlateral line
- Retract gluteus maximus posteriorly, TFL anteriorly
- Separate gluteus medius from piriformis and gluteus minimus by blunt dissection
- Oblique incision through periosteum from the posterior border of gluteus medius across the trochanter and distally in the vastus lateralis
Advantage: Preserves integrity of the gluteus medius muscle while giving good lateral access.
2e. Transtrochanteric Approach (for Revision THA)
Used when standard approaches are inadequate for revision surgery.
Key feature: Osteotomy of the greater trochanter allows retraction of the abductor mechanism and complete exposure of the femoral canal and acetabulum.
Uses: Revision THA where implant removal requires extended access, trochanteric advancement for abductor insufficiency.
Risk: Trochanteric nonunion (historically 5-20%), bursitis, heterotopic ossification.
3. POSTERIOR APPROACHES
These are the most widely used approaches for hip arthroplasty worldwide.
Key anatomical note (Campbell's): If femoral head viability matters (resurfacing, fracture repair), the medial femoral circumflex artery (MFCA) and its ascending branches must be protected. The attachments of the obturator externus and quadriceps femoris must be preserved.
3a. Osborne Posterior Approach (TECHNIQUE 1.72)
Position: Lateral decubitus, unaffected side down.
Incision: Begins 4.5 cm distal and lateral to the posterior superior iliac spine (PSIS), runs laterally and distally parallel to gluteus maximus fibers, to the posterosuperior angle of the greater trochanter, then distally 5 cm along its posterior border.
Steps:
- Separate gluteus maximus fibers parallel to the incision - no more than 7 cm to protect branches of the inferior gluteal artery and nerve
- Divide insertion of gluteus maximus into fascia lata for 5 cm
- Internally rotate the thigh; detach piriformis and gemellus tendons near their trochanteric insertions; retract medially (gemelli protect the sciatic nerve)
- Incise capsule longitudinally to expose the posterior femoral neck and posterior acetabular border
3b. Moore Posterior Approach ("Southern Exposure") (TECHNIQUE 1.73)
The most popular posterior approach for hip arthroplasty and trauma.
Position: Unaffected side down.
Incision: Approximately 10 cm distal to the PSIS, extends distally and laterally parallel to gluteus maximus fibers to the posterior margin of the greater trochanter, then distally 10-13 cm parallel to the femoral shaft.
Steps:
- Open deep fascia in line with skin incision
- Blunt separation of gluteus maximus fibers - no more than 7 cm from the trochanter tip (protects inferior gluteal artery/nerve)
- Expose sciatic nerve and retract carefully
- Divide the gemelli, obturator internus, and piriformis at their femoral insertions; retract medially (tag for later reattachment)
- Posterior capsule well exposed; incise from distal to proximal along the femoral neck to the acetabular rim
- Detach distal capsule from femur; flex the thigh and knee 90°, internally rotate, and dislocate hip posteriorly
Structures at risk:
- Sciatic nerve (neurapraxia, usually peroneal division) - protected by short external rotators; can be stretched with excessive lengthening
- Inferior gluteal artery - injured during gluteus maximus splitting
- MFCA - may be damaged during external rotator takedown
Structures at risk summary (Moore/posterior):
- Sciatic nerve
- Inferior gluteal artery
- MFCA (ascending branches)
3c. Posterolateral Approach for THA (Gibson Modification)
Position: Straight lateral, firmly anchored.
Incision: Slightly curved, centered over the greater trochanter. Begins proximally at a point level with the ASIS along a line parallel to the posterior trochanteric edge, extends distally 10 cm below the greater trochanter.
Steps:
- Divide subcutaneous tissues down to fascia lata and gluteal fascia
- Divide fascia in line with the wound over the center of the trochanter
- Bluntly split the gluteus maximus proximally in direction of its fibers
- Retract anterior and posterior fascia edges; insert self-retaining retractor (do not entrap sciatic nerve posteriorly)
- Divide trochanteric bursa, sweep posteriorly to expose the short external rotators and posterior trochanteric edge
- Divide short external rotators near insertion; reflect posteriorly with the capsule for later repair
Key advantages over pure posterior approach:
- Can be extended proximally with trochanteric osteotomy for anterior dislocation
- Can be extended distally to the posterolateral femoral shaft
Posterior capsule repair with external rotator repair significantly reduces the dislocation rate of the posterolateral approach (from ~5% to ~1%).
4. MEDIAL APPROACHES
4a. Ludloff Medial Approach (Classic)
First described in 1908 for surgery on congenitally dislocated hips with the hip in flexion, abduction, and external rotation (which halves the distance from skin to the medial femoral head/lesser trochanter).
Muscular interval:
- Superficial: between sartorius and adductor longus
- Deep: between iliopsoas and pectineus
4b. Ferguson / Hoppenfeld and deBoer Medial Approach (TECHNIQUE 1.74)
Position: Hip flexed, abducted, externally rotated.
Incision: Longitudinal on the medial thigh, beginning ~2.5 cm distal to the pubic tubercle over the interval between the gracilis and adductor longus.
Steps:
- Develop plane between adductor longus and brevis (anterior) and gracilis and adductor magnus (posterior)
- Protect the posterior branch of the obturator nerve and the gracilis neurovascular bundle
- The lesser trochanter and the inferior hip capsule are on the floor of the wound
Cavaignac modification: Interval between the lateral belly and aponeurosis of adductor longus; lesser trochanter exposed by blunt dissection; inferior capsule accessed by retracting the iliopsoas tendon laterally.
Structures at risk:
- Obturator nerve (anterior division) and MFCA - located between adductor brevis and adductor magnus/pectineus
Uses: Open reduction of CDH, psoas tendon release, biopsy of the lesser trochanter, access to the inferior capsule.
5. SURGICAL HIP DISLOCATION (Ganz Approach) / TRANSTROCHANTERIC APPROACH
Position: Lateral decubitus.
Features: Provides 360° access to the femoral head and acetabulum while preserving the blood supply to the femoral head by protecting the MFCA via the trochanteric flip osteotomy.
Steps:
- Posterior skin incision
- Trochanteric flip osteotomy - the greater trochanter with the anterior TFL/gluteus medius sleeve is flipped anteriorly
- Short external rotators left intact (protecting MFCA)
- Hip capsule opened with Z-shaped capsulotomy
- Full 360° visualization of the femoral head articular surface and acetabulum
Uses: Femoral head osteochondroplasty, labral repair, chondral lesions, femoro-acetabular impingement (FAI), avascular necrosis procedures, acetabular fractures with femoral head pathology.
Advantage: Provides the widest exposure of the joint while maintaining femoral head perfusion - unlike other posterior approaches that risk the MFCA.
Summary Comparison Table
| Approach | Position | Interval (Superficial/Deep) | Key Structures at Risk | Main Uses |
|---|---|---|---|---|
| Smith-Petersen (Anterior) | Supine | Sartorius/TFL → Rectus femoris/Gluteus medius | LFCN, LFCA ascending, femoral nerve | CDH, arthroplasty, femoral neck ORIF |
| DAA | Supine | Intermuscular + internervous | LFCN, LFCA | THA (minimally invasive) |
| Watson-Jones (Anterolateral) | Lateral | TFL/Gluteus medius (no true internervous plane) | Superior gluteal nerve, LFCA | Femoral neck fractures, THA |
| Hardinge (Direct Lateral) | Lateral | Split gluteus medius/vastus lateralis | Superior gluteal nerve | THA, revision |
| Harris Transtrochanteric | Lateral | Greater trochanter osteotomy | Heterotopic ossification, nonunion | Extensive hip exposure |
| Moore/Osborne (Posterior) | Lateral | Gluteus maximus split → Short external rotators | Sciatic nerve, MFCA, inf. gluteal artery | THA, fracture, dislocation |
| Posterolateral (Gibson) | Lateral | Same as posterior + distal extension | Sciatic nerve | THA primary/revision |
| Ganz (Surgical Dislocation) | Lateral | Trochanteric flip osteotomy | Careful MFCA preservation | FAI, labrum, osteochondral |
| Medial (Ludloff/Ferguson) | Supine, hip FR | Adductor longus/Gracilis → Iliopsoas/Pectineus | Obturator nerve, MFCA | CDH reduction, psoas release |
Key Neurovascular Structures Relevant to All Approaches
- LFCN - injured in virtually all anterior approaches; causes meralgia paresthetica
- Superior gluteal nerve - exits sciatic notch, runs ~5 cm above acetabular rim; injury causes TFL/gluteus medius denervation and Trendelenburg gait; at risk in any lateral approach if dissection goes >5 cm proximal to the trochanter
- Sciatic nerve - major risk in all posterior approaches; usually peroneal division affected; protected by the short external rotators in the posterior approach
- MFCA - main blood supply to the femoral head; at risk in posterior approaches when short external rotators are detached; preserving the obturator externus protects it
- Inferior gluteal artery - at risk if gluteus maximus split exceeds 7 cm from the trochanter tip
- Femoral nerve/artery - at risk with medial retractors in anterior approaches
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Edition; Rockwood and Green's Fractures in Adults 10th Ed 2025
This is a shared conversation. Sign in to Orris to start your own chat.