What is vitristis
Reading File
Searching the Web
vitritis definition ophthalmology
Finding Sources
Searching PubMed
vitritis uveitis inflammation vitreous
Finding Sources
Reading File
Finding Sources
Reading File
Vitritis is the term used in ophthalmology for inflammation of the vitreous humor — the gel-like substance that fills the eye between the lens and the retina.
What it is
Vitritis refers to the presence of inflammatory cells and debris within the vitreous cavity. It is not a disease in itself, but a sign of underlying ocular or systemic inflammation — most commonly a feature of posterior uveitis or endophthalmitis.
How it presents
- Blurred or hazy vision (the vitreous becomes turbid/cloudy)
- Floaters (inflammatory cells seen as floating spots)
- Impaired fundal view on examination — the ophthalmologist cannot clearly see the retina through the inflamed vitreous
- In severe cases: loss of the red reflex and significant visual loss
Causes
Vitritis can result from a wide range of infectious and non-infectious conditions:
| Category | Examples |
|---|---|
| Infectious | Toxoplasma chorioretinitis, fungal endophthalmitis (Candida), bacterial endophthalmitis, CMV retinitis, ARN (Acute Retinal Necrosis), syphilis |
| Non-infectious / Inflammatory | Sarcoidosis, Behçet disease, pars planitis (intermediate uveitis), large cell lymphoma (especially in patients >50 with refractory vitritis) |
| Post-surgical | Following cataract or other intraocular surgery |
Note: In Progressive Outer Retinal Necrosis (PORN), vitritis is notably minimal or absent, which helps distinguish it from ARN (where significant vitritis is expected). In large cell lymphoma, refractory unilateral vitritis with yellow-white subretinal infiltrates and no pain should raise suspicion.
Significance
- Vitritis grading (mild, moderate, severe) helps gauge the extent of intraocular inflammation
- Severe vitritis can preclude adequate fundus examination, necessitating B-scan ultrasound to rule out retinal detachment
- It is a key feature in diagnosing and monitoring endophthalmitis, uveitis, and other sight-threatening conditions
— Kanski's Clinical Ophthalmology, 10th ed.; The Wills Eye Manual
Can you help me study uveitis for my finals 3rd year mbbs
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here are your comprehensive Uveitis notes for 3rd year MBBS finals.
🔵 UVEITIS — Comprehensive Study Notes
Source: Kanski's Clinical Ophthalmology 10th ed. | The Wills Eye Manual
1. DEFINITION
Uveitis = Inflammation of the uveal tract (iris + ciliary body + choroid).
It is the 3rd most common cause of preventable blindness in the developed world.
2. CLASSIFICATION (SUN Working Group — Anatomical)
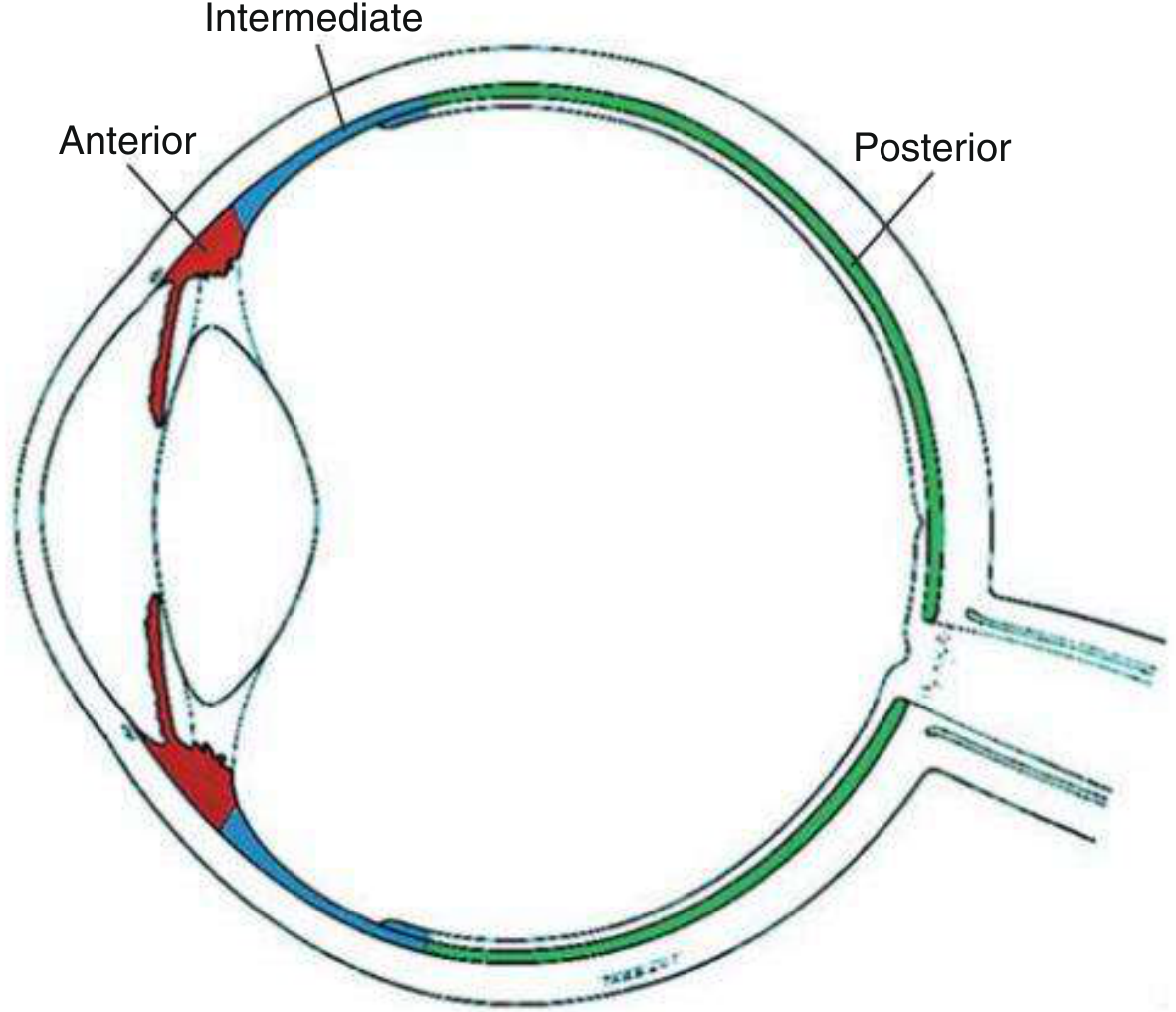
| Type | Primary Site | Also Called |
|---|---|---|
| Anterior | Anterior chamber | Iritis / Iridocyclitis |
| Intermediate | Vitreous / pars plana | Pars planitis |
| Posterior | Retina / choroid | Retinitis, choroiditis |
| Panuveitis | All uveal structures | — |
Most common = Anterior uveitis (AAU)
By Aetiology (IUSG Classification)
- Infectious: bacterial, viral, fungal, parasitic
- Non-infectious: with or without systemic association
- Masquerade: neoplastic (lymphoma) or non-neoplastic (juvenile xanthogranuloma)
By Course (SUN Terminology)
| Term | Definition |
|---|---|
| Acute | Sudden onset, limited duration (≤3 months) |
| Recurrent | Repeated episodes with inactive periods in between |
| Chronic | Persistent >3 months, relapse <3 months after stopping treatment |
| Remission | No visible cells for ≥3 months |
3. ANTERIOR UVEITIS
Symptoms (AAU — Acute Anterior Uveitis)
- Pain (often severe, deep, aching)
- Photophobia
- Redness (perilimbal/ciliary flush)
- Blurred vision
- Watery discharge
- Often unilateral, rapid onset
CAU (Chronic) may be asymptomatic until complications develop!
Signs — Slit Lamp Findings
| Sign | Description |
|---|---|
| Ciliary flush | Circumcorneal redness, violaceous hue (perilimbal injection) |
| Miosis | Pupillary sphincter spasm |
| Aqueous flare | Hazy AC due to protein breakdown of blood–aqueous barrier |
| AC cells | Inflammatory cells in anterior chamber (graded on 1×1 mm slit beam) |
| Hypopyon | White layering of pus at bottom of AC (gravity-dependent) |
| KP (keratic precipitates) | Deposits on corneal endothelium |
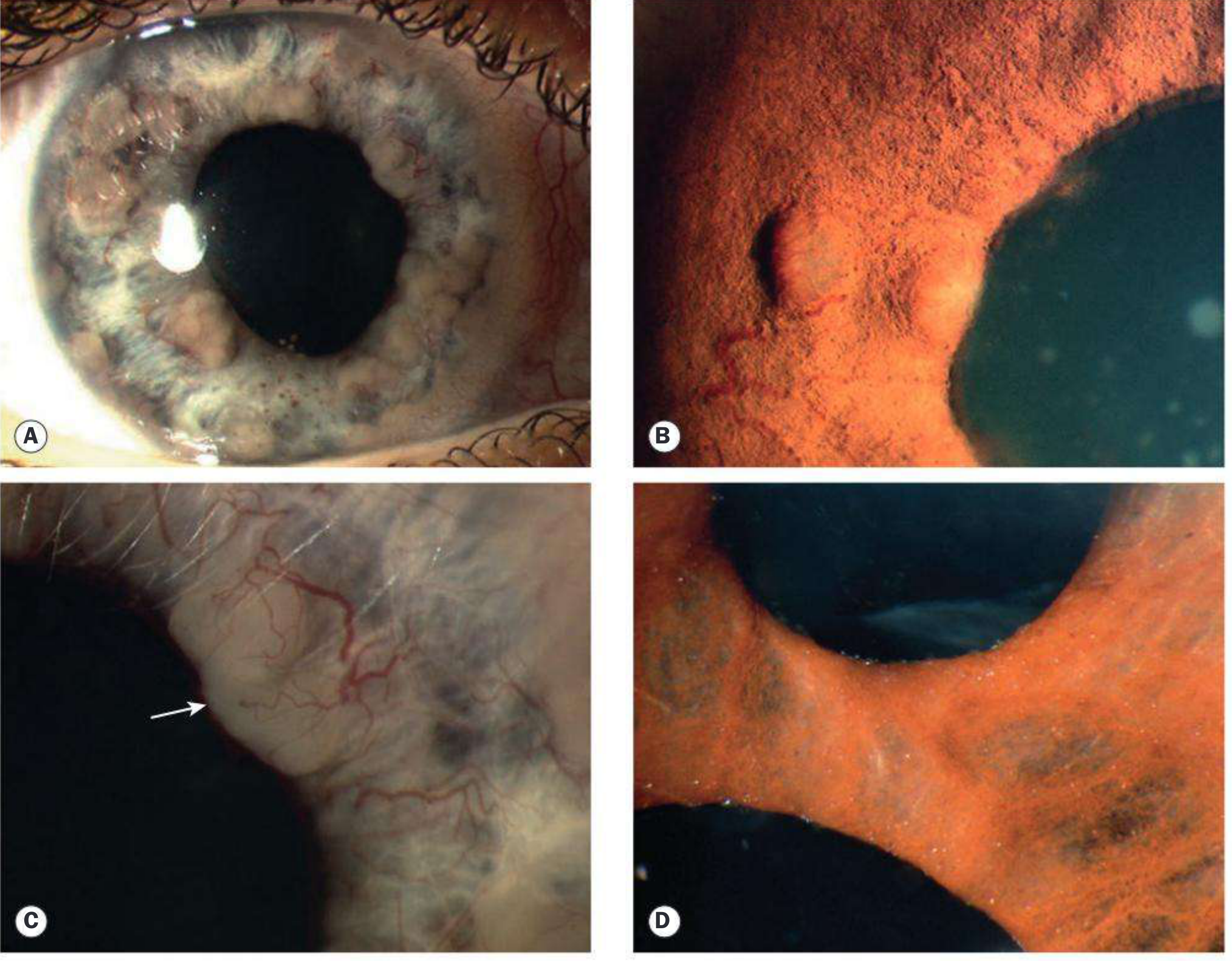
| Posterior synechiae | Adhesions between pupil margin and anterior lens capsule |
| Fibrinous exudate | In severe/HLA-B27 AAU |
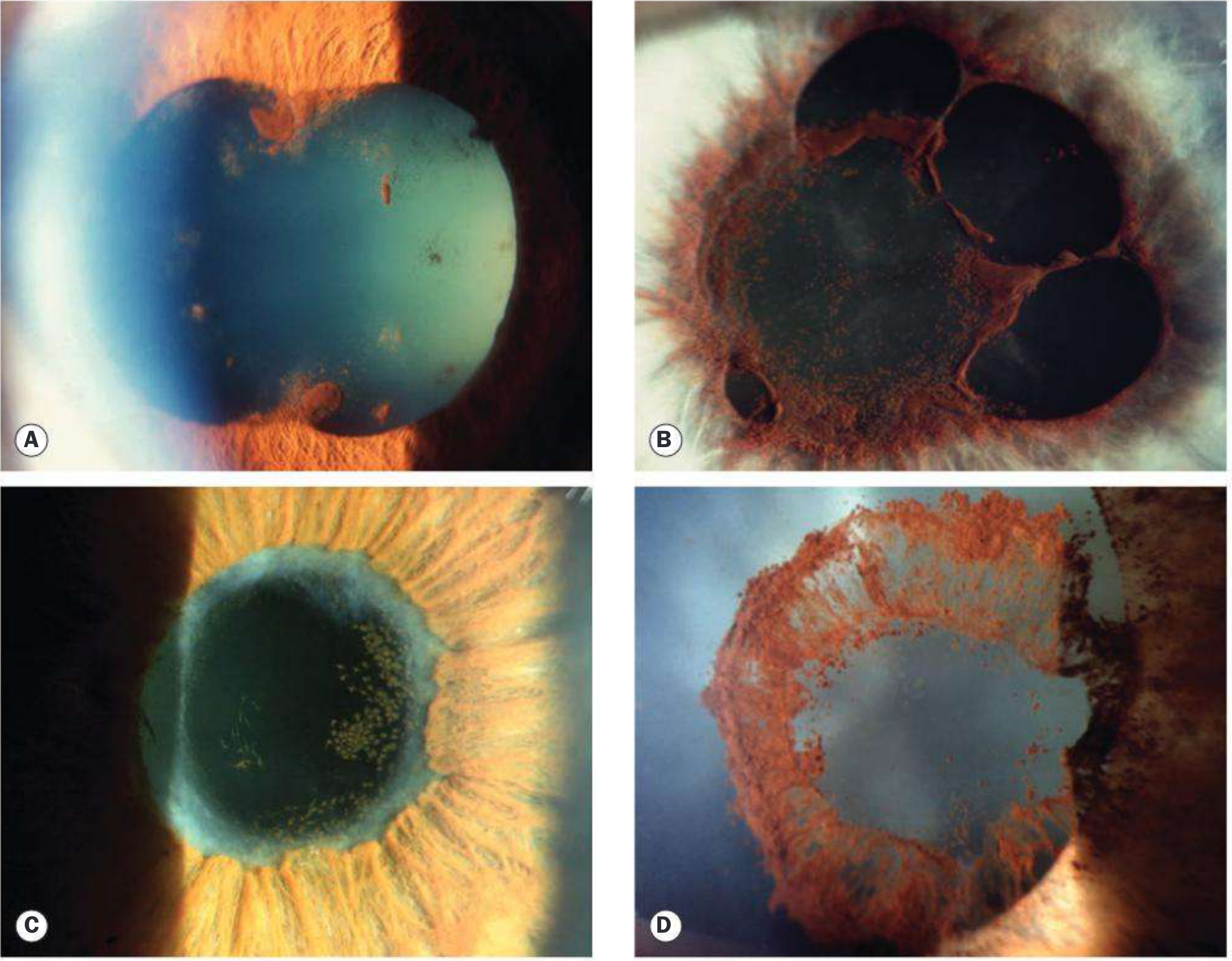
| Iris nodules | Busacca (stromal) — granulomatous; Koeppe (pupillary margin) |
Keratic Precipitates (KP) — HIGH YIELD
| KP Type | Appearance | Associated Condition |
|---|---|---|
| Fine/small | Non-granulomatous | HLA-B27, idiopathic |
| Mutton fat (large, greasy) | Granulomatous | Sarcoidosis, TB, VKH |
| Stellate / filamentous | Star-shaped | Fuchs uveitis syndrome |
| Pigmented | Old/healed | Resolved granulomatous |
Posterior Synechiae (PS)
- Adhesions between pupil margin and anterior lens capsule
- Can lead to seclusio pupillae (360° PS) → iris bombé → angle closure glaucoma
- Prevented by: mydriatics (cyclopentolate, atropine)
Iris nodules in anterior uveitis
4. SYSTEMIC ASSOCIATIONS — HIGH YIELD TABLE
| Category | Disease |
|---|---|
| Idiopathic | ~50% of AAU |
| HLA-B27 (~20% of AAU) | Ankylosing spondylitis, Reactive arthritis (Reiter syndrome), Psoriatic arthritis, IBD (UC/Crohn's) |
| Granulomatous | Sarcoidosis, TB, Leprosy |
| Infections | HSV, VZV (ophthalmic zoster), Syphilis, Lyme disease, TB |
| Autoimmune | JIA (juvenile idiopathic arthritis), SLE, MS, Behçet disease |
| Other | Tubulointerstitial nephritis + uveitis (TINU syndrome) |
| Masquerade | Lymphoma, Melanoma, JXG |
HLA Associations — EXAM FAVOURITE
| HLA | Condition |
|---|---|
| HLA-B27 | Recurrent acute anterior uveitis |
| HLA-A29 | Birdshot retinopathy |
| HLA-B51/B5 | Behçet syndrome |
| HLA-DR4 | Sympathetic ophthalmia, VKH syndrome |
| HLA-B7/DR2 | Presumed ocular histoplasmosis |
Behçet disease classically causes mobile hypopyon (low fibrin content — shifts with head position). In HLA-B27, hypopyon is immobile (high fibrin).
5. POSTERIOR UVEITIS
- Encompasses retinitis, choroiditis, retinal vasculitis
- Presents with floaters, visual loss (painless or mild pain)
- Vitritis is common
- Causes include: Toxoplasma (most common in immunocompetent), CMV (immunocompromised), syphilis, TB, sarcoidosis, Behçet
6. INTERMEDIATE UVEITIS
- Primary site: vitreous + pars plana
- "Pars planitis" — idiopathic type in young adults
- Signs: snowball opacities in vitreous, snowbanking at pars plana
- Associations: MS, sarcoidosis
7. COMPLICATIONS OF UVEITIS
| Complication | Mechanism |
|---|---|
| Cataract | Inflammation + steroid use |
| Glaucoma | PS → pupil block / trabeculitis / steroid-induced |
| Macular oedema | Most common cause of vision loss |
| Band keratopathy | Calcium deposition in Bowman's layer (esp. JIA) |
| Retinal detachment | In severe posterior/panuveitis |
| Phthisis bulbi | End-stage, shrunken eye |
8. INVESTIGATIONS
| Test | Purpose |
|---|---|
| Slit lamp exam | Cells, flare, KP, PS grading |
| HLA-B27 | AAU, spondyloarthropathies |
| Serum ACE + Lysozyme | Sarcoidosis (ACE elevated in ~80% acute sarcoid) |
| CXR / HRCT chest | Sarcoidosis, TB |
| VDRL + FTA-ABS | Syphilis (do both) |
| QuantiFERON-TB Gold / Mantoux | TB |
| ANA | JIA-associated CAU (children) |
| ANCA (c-ANCA) | Wegener's granulomatosis (with scleritis) |
| ESR, CRP | Non-specific inflammation |
| HIV serology | Opportunistic infections |
| B-scan ultrasound | Retinal detachment when vitritis obscures view |
| Aqueous/vitreous PCR | Viral/parasitic identification |
9. TREATMENT
General Principle
Identify and treat any underlying/infectious cause first. For non-infectious uveitis, the goal is steroid-free remission.
Step 1 — Topical Steroids
- Prednisolone 1% or dexamethasone 0.1% (most commonly used)
- Start hourly in moderate-severe AAU, then taper over ~5–6 weeks
- Typical taper: hourly → every 2h → QID → TID → BD → OD → stop
Step 2 — Cycloplegics (MANDATORY in AAU)
- Prevent PS formation, break recent synechiae, relieve ciliary spasm
- Cyclopentolate (12–24h), Homatropine (3 days), Atropine (7–10 days)
- Use more potent agents in severe or recurrent disease
Step 3 — Periocular / Systemic Steroids
- For intermediate/posterior/panuveitis
- Periocular injection (posterior sub-Tenon): triamcinolone
- Oral prednisolone: 1 mg/kg/day, taper over weeks
- CAU: aim for complete suppression (no cells, no flare)
Step 4 — Immunomodulatory Therapy (steroid-sparing)
Used when: inadequate response, steroid side effects, chronic disease needing long-term control
| Drug | Notes |
|---|---|
| Methotrexate | Common first-line, also for JIA uveitis |
| Azathioprine | Second-line; small lymphoma risk |
| Mycophenolate mofetil | Good for posterior uveitis |
| Cyclosporin A | Especially Behçet, VKH |
| Anti-TNF agents (adalimumab, infliximab) | Refractory/non-infectious uveitis |
Important: Exclude active TB before starting immunosuppressants!
10. HIGH-YIELD EXAM PEARLS
| Scenario | Think of |
|---|---|
| Young man, recurrent unilateral AAU + back pain | HLA-B27 / Ankylosing spondylitis |
| Bilateral granulomatous uveitis + lung hilar adenopathy | Sarcoidosis |
| Bilateral uveitis + vitiligo + poliosis + meningism | VKH syndrome |
| Uveitis after penetrating eye injury to other eye | Sympathetic ophthalmia |
| Mobile hypopyon | Behçet disease |
| Heterochromia + stellate KP + no synechiae | Fuchs uveitis syndrome |
| Posterior uveitis + immunosuppression (HIV) | CMV retinitis or toxoplasma |
| Unilateral posterior uveitis + "headlight in fog" lesion | Toxoplasmosis |
| Child + CAU + positive ANA + oligoarthritis | JIA (pauciarticular) |
| Refractory vitritis + >50 yrs + no pain | Intraocular lymphoma |
Sources: Kanski's Clinical Ophthalmology 10th ed., The Wills Eye Manual
Would you like me to go deeper on any specific section — e.g., Behçet/VKH/sympathetic ophthalmia in detail, specific infections (toxoplasma, CMV), or a set of practice SAQs for your finals?
This is a shared conversation. Sign in to Orris to start your own chat.