Autonomic autonomous atonic bladder bladder nerve supply
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Searching PubMed
neurogenic bladder autonomic innervation
Reading File
Loading Image
Loading Image
I now have all the material needed for a thorough, well-illustrated answer. Here it is:
Bladder Nerve Supply, Autonomic Control, and Atonic Bladder
Anatomy of the Bladder Wall
The bladder wall is composed of the detrusor muscle - a smooth muscle whose fibers run in multiple directions (inner longitudinal, middle circular, outer longitudinal) and are connected by gap junctions that allow coordinated contraction. The bladder neck (posterior urethra) contains the internal sphincter (smooth muscle, involuntary), and the external urethra passes through the urogenital diaphragm where the external sphincter (skeletal muscle, voluntary) is found.
Nerve Supply of the Urinary Bladder
Three distinct neural pathways supply the bladder:
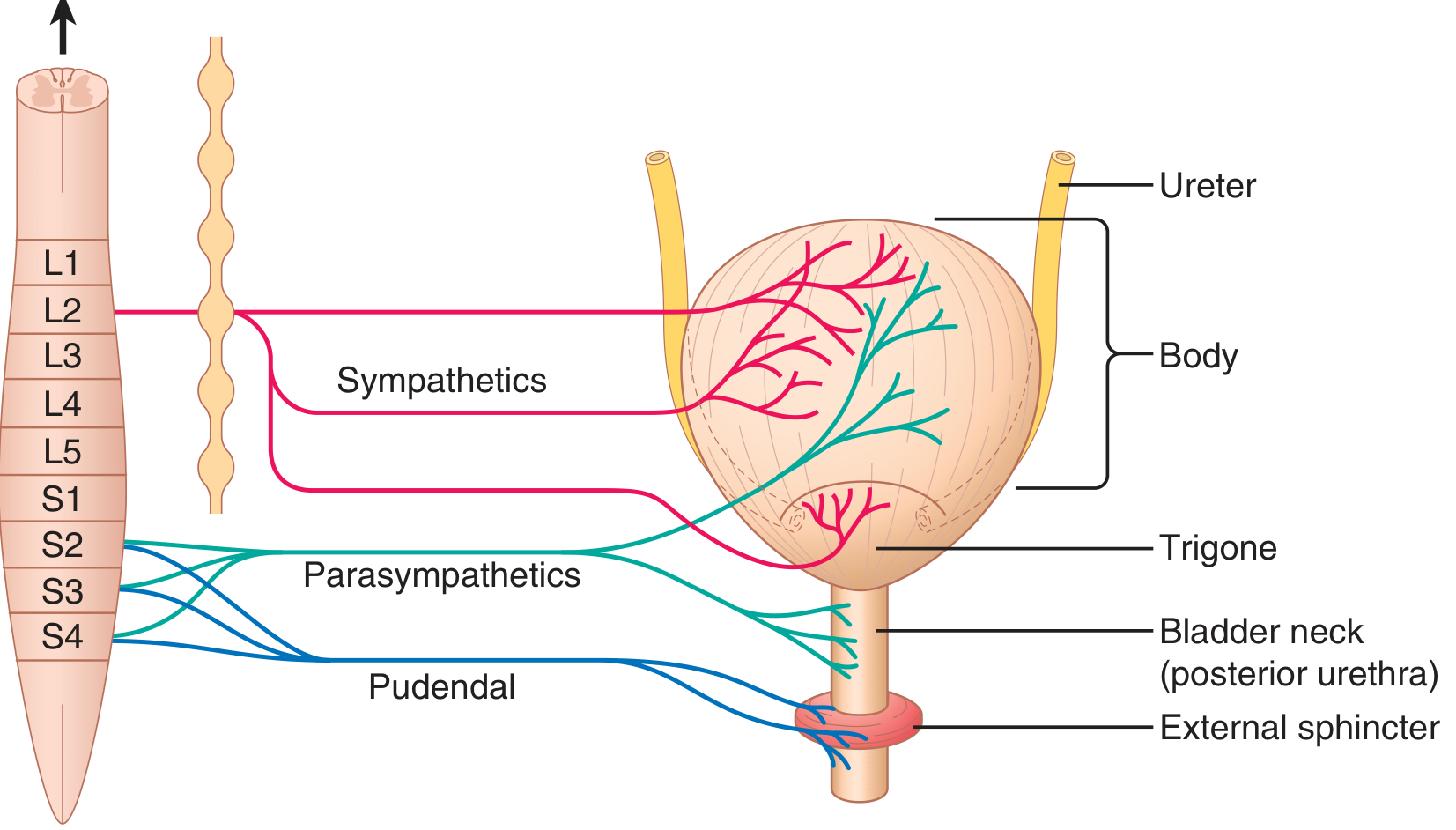
Figure 26.9 - Innervation of the urinary bladder (Guyton and Hall Textbook of Medical Physiology)
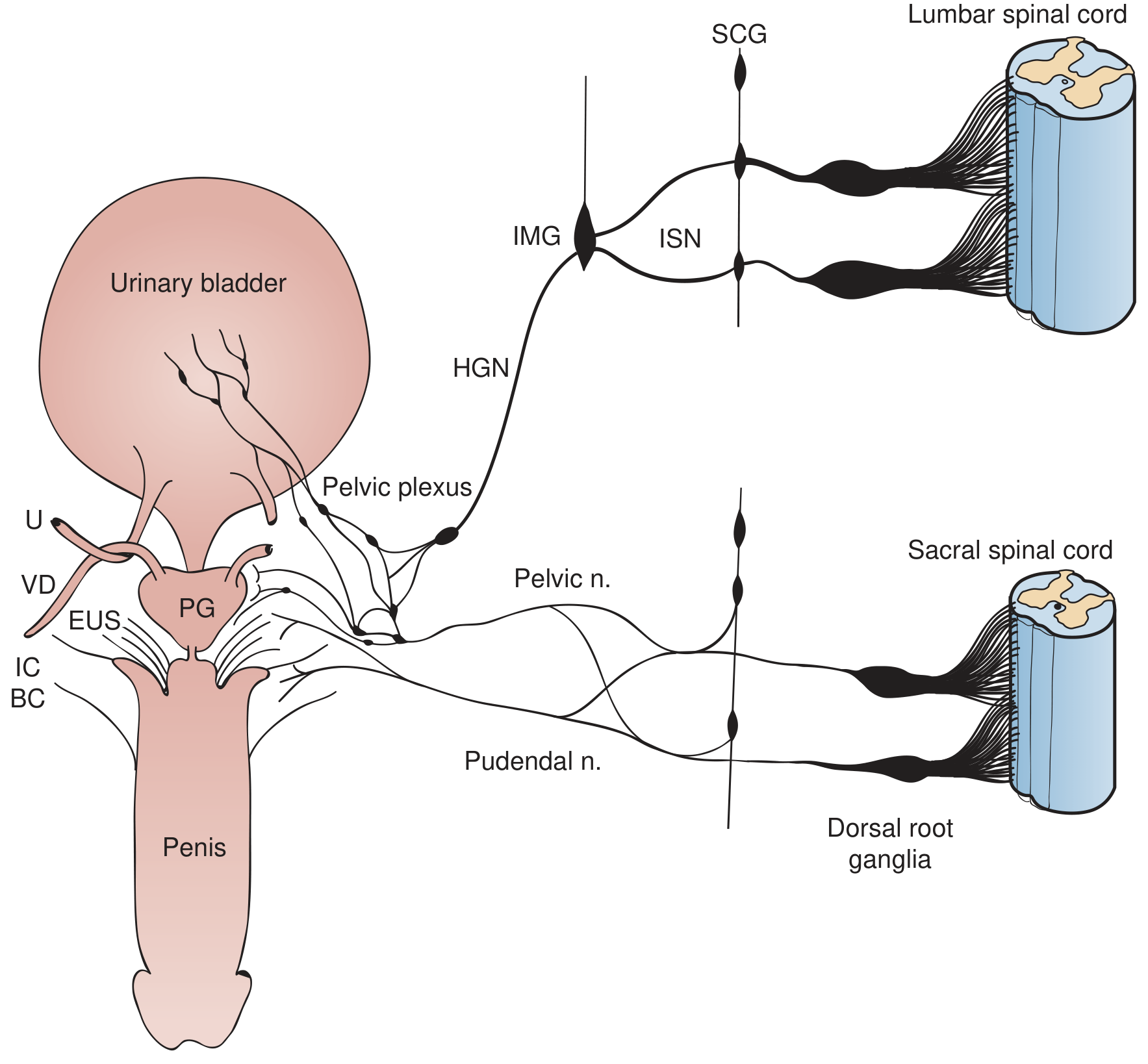
Sympathetic, parasympathetic, and somatic innervation of the bladder and pelvic organs (Campbell-Walsh-Wein Urology). IMG = inferior mesenteric ganglion; HGN = hypogastric nerve; ISN = intermesenteric nerve; SCG = sympathetic chain ganglia; PG = pelvic ganglia; EUS = external urethral sphincter
1. Parasympathetic (Pelvic Nerves) - PRIMARY motor supply
| Feature | Detail |
|---|---|
| Origin | Sacral parasympathetic nucleus in lateral horn of S2, S3, S4 |
| Nerve | Pelvic nerve (nervus erigens) |
| Ganglia | Intramural ganglia in the bladder wall |
| Target | Detrusor muscle (excitatory - contraction) |
| Neurotransmitter | ACh acting on M3 muscarinic receptors |
| Function | Bladder emptying (micturition) |
Sensory stretch fibers from the bladder wall (especially the posterior urethra) also run within the pelvic nerves back to S2-S4. These are the afferents that initiate the micturition reflex.
2. Sympathetic (Hypogastric Nerves) - Filling/storage
| Feature | Detail |
|---|---|
| Origin | Intermediolateral cell column at T11, T12, L1 (some sources include L2) |
| Nerve | Hypogastric nerve (via inferior mesenteric ganglion) |
| Target | Bladder dome (β2 - relaxation), bladder neck/internal sphincter/urethra (α1 - contraction) |
| Function | Storage phase: relax detrusor body, contract bladder outlet |
| Extra | Also inhibits parasympathetic ganglia at the spinal cord and pelvic plexus level |
The dominant sympathetic effect is to contract the bladder base and urethra while inhibiting the parasympathetics - thus promoting urine storage. Sympathetics also supply blood vessels.
3. Somatic (Pudendal Nerve) - Voluntary sphincter control
| Feature | Detail |
|---|---|
| Origin | Onuf's nucleus (sphincteromotor nucleus) in anterior horn at S3, S4 |
| Nerve | Pudendal nerve |
| Target | External urethral sphincter (skeletal muscle) |
| Function | Voluntary contraction to prevent micturition; reflex relaxation during voiding |
Summary Table (Neuroanatomy through Clinical Cases)
| Pathway | Nucleus | Nerve Roots |
|---|---|---|
| Detrusor and urethral afferents | - | S2, S3, S4 |
| Parasympathetic to detrusor | Sacral parasympathetic nucleus | S2, S3, S4 |
| Sympathetic (α/β) to bladder neck, urethra, dome | Intermediolateral cell column | T11, T12, L1 |
| Somatic to urethral sphincter | Onuf's nucleus | S3, S4 |
| Somatic to pelvic floor | Anterior horn | S2, S3, S4 |
The Micturition Reflex (Normal)
Micturition is an autonomic spinal cord reflex modulated by higher centers:
- Bladder fills → stretch receptors in detrusor and posterior urethra activate
- Sensory signals travel via pelvic nerves → S2-S4 → sacral cord
- Reflex parasympathetic efferents return via pelvic nerves → detrusor contraction
- When strong enough, the reflex also inhibits the external sphincter via the pudendal nerve
- Voiding occurs
Higher center control:
- Pontine micturition center (PMC/Barrington's nucleus): strong facilitatory and inhibitory center; coordinates detrusor-sphincter synergy
- Medial frontal cortex: primarily inhibitory; voluntary suppression of micturition
- Cerebellum/basal ganglia: fine-tuning
Normal voluntary urination is initiated by: voluntary relaxation of external sphincter → triggers inhibition of sympathetics to bladder neck → activates parasympathetics → detrusor contracts.
Atonic (Autonomous/Flaccid) Bladder
An atonic bladder is a lower motor neuron (LMN) type neurogenic bladder - areflexic and acontractile.
Mechanism
The micturition reflex cannot occur if sensory nerve fibers from the bladder to the spinal cord are destroyed. Even with intact efferent fibers, the lack of afferent stretch signals means no reflex contraction is initiated. The result: the bladder fills to capacity and overflows a few drops at a time - overflow incontinence.
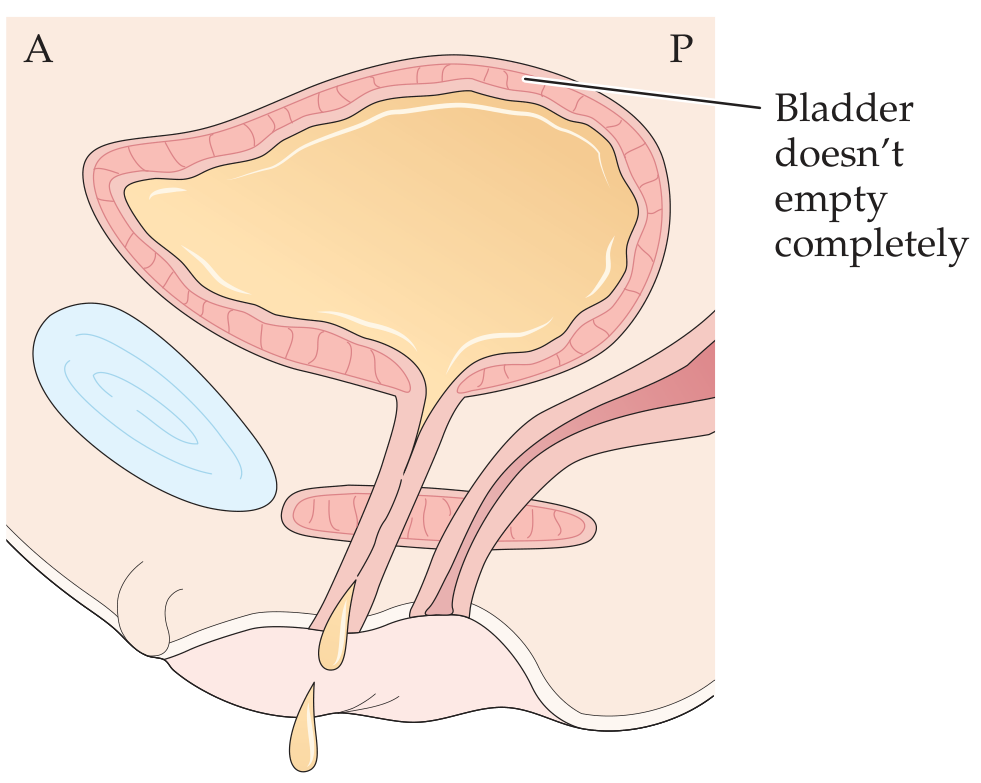
Atonic (flaccid, acontractile) bladder - bladder distends, doesn't empty completely, overflow incontinence (Neuroanatomy through Clinical Cases)
Causes of Atonic Bladder
| Cause | Mechanism |
|---|---|
| Sacral cord injury / conus medullaris lesion | Destroys the S2-S4 sacral reflex arc directly |
| Cauda equina injury | Damages pelvic nerve roots below the cord |
| Tabes dorsalis (tertiary syphilis) | Constrictive fibrosis around dorsal root fibers entering S2-S4 (called "tabetic bladder") |
| Diabetic autonomic neuropathy | Damage to pelvic sensory and motor fibers |
| Pelvic surgery | Intraoperative nerve injury |
| Acute spinal shock | Transient atonia immediately after any SCI above the sacrum |
Characteristics (vs. Spastic Bladder)
| Feature | Atonic Bladder (LMN) | Spastic/Automatic Bladder (UMN) |
|---|---|---|
| Reflex arc | Destroyed (S2-S4) | Intact (above conus) |
| Detrusor | Areflexic/hyporeflexic | Overactive |
| Sphincter | Coordinated (may be normal) | Detrusor-sphincter dyssynergia |
| Residual urine | Large (overflow) | Variable |
| Incontinence type | Overflow ± stress | Urge incontinence |
| Lesion level | Conus/cauda equina/peripheral nerve | Above conus medullaris |
Acute vs. Chronic Central Lesions
Even UMN lesions (above the sacral cord) initially produce a transient atonic phase (spinal shock), which evolves over weeks to months into a hyperreflexic (spastic) bladder. The chronic UMN pattern features detrusor overactivity with detrusor-external sphincter dyssynergia (DESD), causing frequency, urgency, and high intravesicular pressure.
Three Types of Neurogenic Bladder (Guyton Classification)
| Type | Lesion | Mechanism | Result |
|---|---|---|---|
| Atonic bladder | Sensory nerve destruction (dorsal roots S2-S4) | No stretch signals → no reflex | Overflow incontinence |
| Automatic bladder | Spinal cord above sacral level (cord intact at S2-S4) | Reflexes occur without brain control | Periodic unannounced emptying |
| Uninhibited neurogenic bladder | Partial damage in cord/brain stem | Loss of inhibitory signals | Frequent, uncontrollable urination |
Clinical Pearls
- The posterior urethra is the most sensitive region for initiating micturition - stretch receptors here trigger the most powerful reflex signals
- Onuf's nucleus (S3-S4) is characteristically spared in ALS but affected in MSA - an important differentiating point in autonomic failure
- In diabetic cystopathy, the atonic bladder is due to sensory polyneuropathy affecting the afferent limb before the efferent limb is lost
- Bethanechol (muscarinic agonist) can be used to stimulate detrusor contraction in atonic bladder; alpha-blockers reduce internal sphincter tone to aid voiding
- CIC (clean intermittent catheterization) is the cornerstone management for atonic/areflexic bladder to prevent overdistention and upper tract damage
Sources: Guyton and Hall Textbook of Medical Physiology; Neuroanatomy through Clinical Cases, 3rd Edition; Campbell-Walsh-Wein Urology; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.