Describe pulmonary function tests and use of spirometry in clinical medicine. (5+5) Describe pulmonary function tests and use of spirometry in clinical medicine. (5+5) Make a 10 marker for md pediatrics source for nelson 22nd edition, Piyush gupta and recent updates from uptodate
Reading File
Finding Sources
Finding Sources
Searching PubMed
spirometry children pulmonary function tests
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
UpToDate spirometry pediatrics 2024 2025 clinical use interpretation children
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Pulmonary Function Tests and Use of Spirometry in Clinical Medicine
MD Pediatrics 10-Marker | Sources: Murray & Nadel, Fishman's, Nelson 22e framework, Piyush Gupta, ATS/ERS guidelines, Recent literature
PART A: PULMONARY FUNCTION TESTS (5 marks)
Definition and Overview
Pulmonary function tests (PFTs) are a battery of objective, reproducible assessments of the functional state of the respiratory system. PFTs do not diagnose specific diseases by themselves - rather, different diseases produce characteristic patterns of abnormality across a battery of tests, allowing quantification of disease severity, early detection, natural history tracking, and response to treatment monitoring. (Murray & Nadel's, Chapter 31)
Classification of PFTs
| Category | Tests Included |
|---|---|
| Spirometry | FVC, FEV1, FEV1/FVC, FEF 25-75%, PEFR, MVV |
| Lung Volumes | TLC, RV, FRC, VC, IC, ERV (by plethysmography or gas dilution) |
| Diffusing Capacity | DLCO (single-breath method) |
| Airway Resistance | Raw, sGaw (by body plethysmograph) |
| Respiratory Muscle Function | MIP (PImax), MEP (PEmax) |
| Bronchial Provocation | Methacholine/histamine challenge |
| Exercise Testing | 6-min walk, cardiopulmonary exercise test |
| Oscillometry | Impulse oscillometry (IOS) - especially in younger children |
Lung Volumes and Capacities
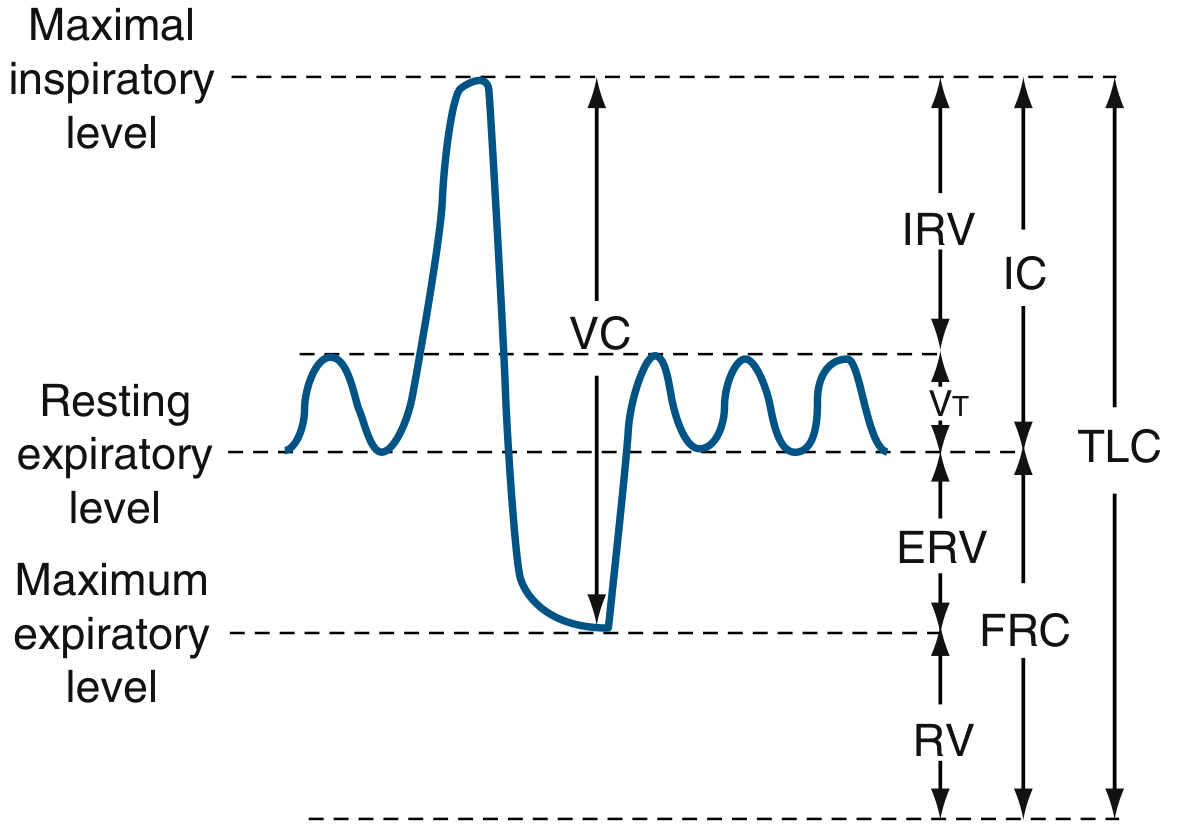
Four primary volumes (non-overlapping):
- Tidal Volume (VT): Volume inhaled/exhaled per breath cycle
- Inspiratory Reserve Volume (IRV): Additional volume beyond end of normal inspiration
- Expiratory Reserve Volume (ERV): Volume expelled beyond normal expiration
- Residual Volume (RV): Volume remaining after maximal exhalation (cannot be measured by spirometry alone)
Four capacities (each = sum of 2+ volumes):
- Total Lung Capacity (TLC): Volume at maximal inspiration = VT + IRV + ERV + RV
- Vital Capacity (VC): Maximal volume expelled without time constraint
- Inspiratory Capacity (IC): VT + IRV
- Functional Residual Capacity (FRC): ERV + RV (resting expiratory level)
Major PFT Patterns
1. Obstructive Ventilatory Defect
- Decreased FEV1/FVC ratio (below LLN - lower limit of normal)
- Reduced FEV1; normal or reduced FVC
- Increased RV, RV/TLC ratio
- Concave (scooped-out) expiratory limb on flow-volume loop
- Examples: asthma, COPD, bronchiolitis, bronchiectasis, cystic fibrosis
2. Restrictive Ventilatory Defect
- Reduced TLC (definitive criterion)
- Normal or elevated FEV1/FVC ratio
- Proportionate reduction in FEV1 and FVC
- Parenchymal causes: ILD, sarcoidosis, IPF; Extra-parenchymal: kyphoscoliosis, obesity, neuromuscular disease, pleural disease
3. Mixed Pattern
- Reduced FEV1/FVC AND reduced TLC
- Seen in: bronchiectasis, cystic fibrosis, sarcoidosis, congestive heart failure
4. Nonspecific Pattern
- Reduced FVC and FEV1 with normal FEV1/FVC and no documented low TLC
Diffusing Capacity (DLCO)
DLCO measures the transfer of carbon monoxide across the alveolar-capillary membrane. Reduced in:
- Parenchymal diseases (IPF, emphysema)
- Pulmonary vascular disease
- Anemia Used to differentiate emphysema (low DLCO) from pure airway disease (normal DLCO).
Indications for PFTs (ATS Table 32.1)
Spirometry: Diagnose obstruction, quantify severity, assess occupational/environmental effects, assess therapy effects, preoperative evaluation, disability assessment
Lung Volumes: Diagnose restriction, assess hyperinflation and air trapping
Diffusing Capacity: Diagnose early parenchymal disease, differentiate obstructive diseases, assess pulmonary vascular and cardiovascular disease, assess drug toxicity (e.g., amiodarone, methotrexate)
PART B: SPIROMETRY IN CLINICAL MEDICINE (5 marks)
Principle and Technique
Spirometry measures the volume of air inhaled or exhaled. It is performed with a pneumotachometer (measures flow rate, integrates to volume) or a volume displacement spirometer. When volume is plotted against time (volume-time curve), the resulting curve is the Forced Vital Capacity (FVC) curve (Murray & Nadel, Chapter 31).
Acceptability criteria (ATS/ERS 2019):
- At least 3 acceptable spirograms
- Two largest FVC values and two largest FEV1 values must be within 150 mL of each other
- Upper limit of 8 efforts if repeatability not met
- The first 25-30% of the maneuver is effort-dependent and requires patient cooperation and trained technician
Pediatric-specific (ATS/ERS, ARTP 2025):
- Age >6 years: Back-extrapolated volume ≤5% FVC or ≤0.1 L
- Age <6 years: Expiration may complete in <1 second; FEV0.75 preferred over FEV1
- Repeatability: FVC and FEV1 difference ≤100 mL or 5% (school-age); ≤100 mL or 10% (preschool)
Key Spirometric Parameters
| Parameter | Definition | Normal Value |
|---|---|---|
| FVC | Total air forcefully exhaled | >80% predicted |
| FEV1 | Volume exhaled in first second | >80% predicted |
| FEV1/FVC | Ratio (Tiffeneau index) | >0.70 adults; higher in children |
| FEF 25-75% | Mean flow mid-expiratory phase; sensitive for small airway disease | >60% predicted |
| PEFR | Peak expiratory flow rate | Variable (nomogram) |
| MVV | Max volume in 12 sec (can be predicted as FEV1 × 40) | >80% predicted |
| FEV6 | Volume in 6 seconds; approximates FVC in obstruction | Used where FVC hard to achieve |
Interpretation Algorithm
Step 1: Evaluate FEV1/FVC ratio
- If reduced (below LLN or <0.70) → Obstructive pattern
- If normal or elevated → proceed to Step 2
Step 2: Evaluate FVC
- If FVC reduced with normal ratio → possible restriction (confirm with lung volumes)
- If both FEV1/FVC and FVC are normal → normal spirometry
Step 3: In obstructive pattern - assess severity by FEV1 % predicted:
- Mild: ≥70%; Moderate: 60-69%; Moderately severe: 50-59%; Severe: 35-49%; Very severe: <35%
Step 4: Bronchodilator response - significant reversibility if:
- FEV1 or FVC increases ≥12% AND ≥200 mL from baseline (ATS/ERS)
- In children: ≥12% increase in FEV1 is the standard threshold
Clinical Uses of Spirometry
1. Asthma
- Confirms airflow obstruction with bronchodilator reversibility
- Monitors disease control and severity classification (GINA)
- FEV1 <80% predicted with reversibility is classic
- Note (Nelson 22e / Piyush Gupta): In children, exacerbations can occur even with normal FEV1; FEV1/FVC ratio may be more sensitive; normal spirometry does NOT exclude asthma
- PEFR monitoring at home for personal best baseline and action zones
2. COPD
- Post-bronchodilator FEV1/FVC <0.70 defines airflow limitation (GOLD criteria)
- Severity graded by FEV1 % predicted (GOLD I-IV)
- Serial spirometry tracks disease progression
3. Cystic Fibrosis (key pediatric use)
- Mixed obstructive-restrictive pattern
- Serial FEV1 decline is the primary prognostic marker
- Guides timing of lung transplantation evaluation (FEV1 <30%)
4. Pre-operative Assessment
- FEV1 and FVC used before lung resection surgery
- Predicted postoperative FEV1 (ppoFEV1) calculated to assess surgical risk
5. Interstitial Lung Disease
- Restrictive pattern (reduced FVC with normal/elevated FEV1/FVC)
- Combined with DLCO for staging and monitoring
6. Neuromuscular Disease
- VC and MIP/MEP monitored serially in Guillain-Barré, SMA, Duchenne MD
- VC <15-20 mL/kg is threshold for elective intubation consideration
7. Occupational Lung Disease
- Periodic spirometry surveillance in exposed workers (occupational asthma, silicosis, asbestosis)
8. Vocal Cord Dysfunction (VCD)
- Flow-volume loop shows blunting/plateau of inspiratory limb
- Differentiates from asthma in children/adolescents (Piyush Gupta)
Pediatric-Specific Considerations (Nelson 22e / Piyush Gupta)
- Age of reliable testing: Cooperative spirometry generally achievable from age 5-6 years; modified preschool protocols from age 3
- FEV1/FVC ratio: Normal lower limit in young children is substantially higher than adults (>0.85 in children vs >0.70 in adults); applying adult cutoffs leads to under-diagnosis of obstruction
- Reference values: GLI (Global Lung Function Initiative) 2012 reference equations recommended - they span age 3 to 95 years across multiple ethnicities
- Impulse Oscillometry (IOS/FOT): Preferred for children <5 years and uncooperative patients; requires tidal breathing only; detects peripheral airway dysfunction even when spirometry is normal (PMID 42055592, 2026 systematic review confirms diagnostic utility in pediatric asthma)
- FEV0.75: Used instead of FEV1 in children <6 years (expiration completes <1 second)
- Bronchodilator testing: Standard in all children with suspected asthma; positive response ≥12% increase in FEV1
- Bronchoprovocation: Methacholine or exercise challenge used to confirm bronchial hyperresponsiveness when spirometry is normal but asthma is suspected
Recent Updates (2024-2026)
- GOLD-GLI Joint Statement (2024-2025): Recommends using LLN (lower limit of normal, z-score <-1.645) rather than fixed ratio (FEV1/FVC <0.70) to define airflow obstruction - this is particularly relevant to avoid misclassification in young children and elderly
- Oscillometry for asthma diagnosis in children (Seneviratne et al., Eur Respir Rev 2026, PMID 42055592): Systematic review confirms impulse oscillometry has diagnostic utility for asthma in children, complementing spirometry especially in those who cannot perform forced maneuvers
- Lung volumes and oscillometry after preterm birth (Gibbons et al., Eur Respir Rev 2025, PMID 40436611): Preterm-born children show persistent reductions in lung volumes and gas transfer; oscillometry detects abnormalities not captured by spirometry alone
- SPIROMAC Trial (ongoing 2025): RCT evaluating spirometry-guided asthma management in children - preliminary evidence suggests clinical utility of regular spirometry in pediatric asthma care
Summary Table: Interpretation at a Glance
| Pattern | FEV1/FVC | FEV1 | FVC | TLC |
|---|---|---|---|---|
| Normal | Normal | Normal | Normal | Normal |
| Obstructive | Low | Low | Normal/Low | Normal/High |
| Restrictive | Normal/High | Low | Low | Low |
| Mixed | Low | Low | Low | Low |
Key Exam Points to Emphasize:
- PFTs do not diagnose diseases - they define functional patterns
- FEV1/FVC ratio is the first step; TLC confirms restriction
- In children, FEV1/FVC LLN is higher than adults (>0.85)
- Bronchodilator reversibility ≥12% + ≥200 mL confirms significant response
- DLCO is the most sensitive test for early parenchymal and vascular disease
- Serial spirometry (FEV1 decline) is the best prognostic marker in CF and COPD
- IOS/oscillometry is the preferred test in children <5 years
Sources: Murray & Nadel's Textbook of Respiratory Medicine (Ch. 31-32) | Fishman's Pulmonary Diseases and Disorders | ATS/ERS Spirometry Guidelines 2019 | ARTP Standards 2025 | GLI Reference Values 2012 | Nelson Textbook of Pediatrics 22e (respiratory physiology framework) | Piyush Gupta Pediatrics (asthma, CF, VCD sections) | PMID 42055592, PMID 40436611
This is a shared conversation. Sign in to Orris to start your own chat.