Low cortisol and low acth what's the next step
Reading File
Finding Sources
Searching PubMed
secondary adrenal insufficiency diagnosis workup
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a complete breakdown of the workup when you find low cortisol + low (or low-normal) ACTH:
Low Cortisol + Low ACTH: Diagnostic Approach
This combination localizes the problem to the pituitary (secondary) or hypothalamus (tertiary) - NOT the adrenal gland itself. The adrenal gland is intact but under-stimulated.
Step 1 - Confirm the Pattern is Real
First, rule out the most common cause before expensive imaging:
- Exogenous glucocorticoid use (any steroid in the past 4+ weeks) suppresses CRH - ACTH - cortisol axis. This is the #1 cause of low ACTH + low cortisol.
- Review all medications, including inhaled, topical, and intra-articular steroids.
Step 2 - Cosyntropin (ACTH) Stimulation Test (CST)
This confirms adrenal insufficiency and helps characterize it:
- Administer 250 mcg cosyntropin (synthetic ACTH) IV or IM
- Measure cortisol at 60 minutes
- Abnormal = cortisol < 18 mcg/dL - confirms secondary adrenal insufficiency
Important caveat: In recent-onset secondary AI (e.g., after acute pituitary event), the adrenal glands have not yet atrophied. Exogenous ACTH can still stimulate them, giving a false-normal CST. If recent pituitary surgery or infarction is suspected, go straight to endocrine consultation.
Step 3 - Pituitary MRI (Most Important Next Step)
Once secondary/tertiary AI is confirmed:
"Low ACTH (<5 pg/mL) and cortisol levels suggest secondary or tertiary adrenal insufficiency, and pituitary CT or MRI is indicated."
- Textbook of Family Medicine 9e
Look for:
| Cause | Notes |
|---|---|
| Pituitary adenoma | Most common structural cause |
| Craniopharyngioma | Especially in younger patients |
| Metastatic tumor | Lung, breast most common |
| Sheehan syndrome | Postpartum pituitary necrosis |
| Lymphocytic hypophysitis | Autoimmune; can be postpartum |
| Infiltrative disease | Sarcoidosis, TB, histoplasmosis |
| Head trauma | History of TBI |
Step 4 - CRH Stimulation Test (to distinguish Secondary vs. Tertiary)
If needed to differentiate pituitary from hypothalamic cause:
- Secondary AI (pituitary failure): little or no rise in ACTH or cortisol after CRH
- Tertiary AI (hypothalamic failure): ACTH rises in an exaggerated, prolonged fashion (the pituitary is intact but un-stimulated)
Step 5 - Insulin Tolerance Test (ITT) - if CST is falsely normal
For recent-onset secondary AI where CST may be normal:
- Challenges the entire HPA axis by inducing hypoglycemia
- Requires endocrine specialist supervision (risk of severe hypoglycemia)
- Alternative: metyrapone test (inhibits cortisol synthesis, assesses ACTH response)
Step 6 - Evaluate for Panhypopituitarism
Because secondary AI often comes with other pituitary hormone deficiencies, check:
- TSH, free T4 (secondary hypothyroidism)
- LH, FSH, testosterone/estrogen (secondary hypogonadism)
- GH/IGF-1
- Prolactin
- ADH axis (diabetes insipidus)
Key Clinical Features That Distinguish Secondary from Primary AI
| Feature | Secondary/Tertiary (low ACTH) | Primary (high ACTH) |
|---|---|---|
| Skin hyperpigmentation | Absent | Present |
| Hyperkalemia | Absent | Present |
| Hyponatremia | May occur (from free-water retention) | Present |
| Mineralocorticoid need | Not required | Required (fludrocortisone) |
| Aldosterone | Normal (RAS intact) | Low |
Diagnostic Flowchart
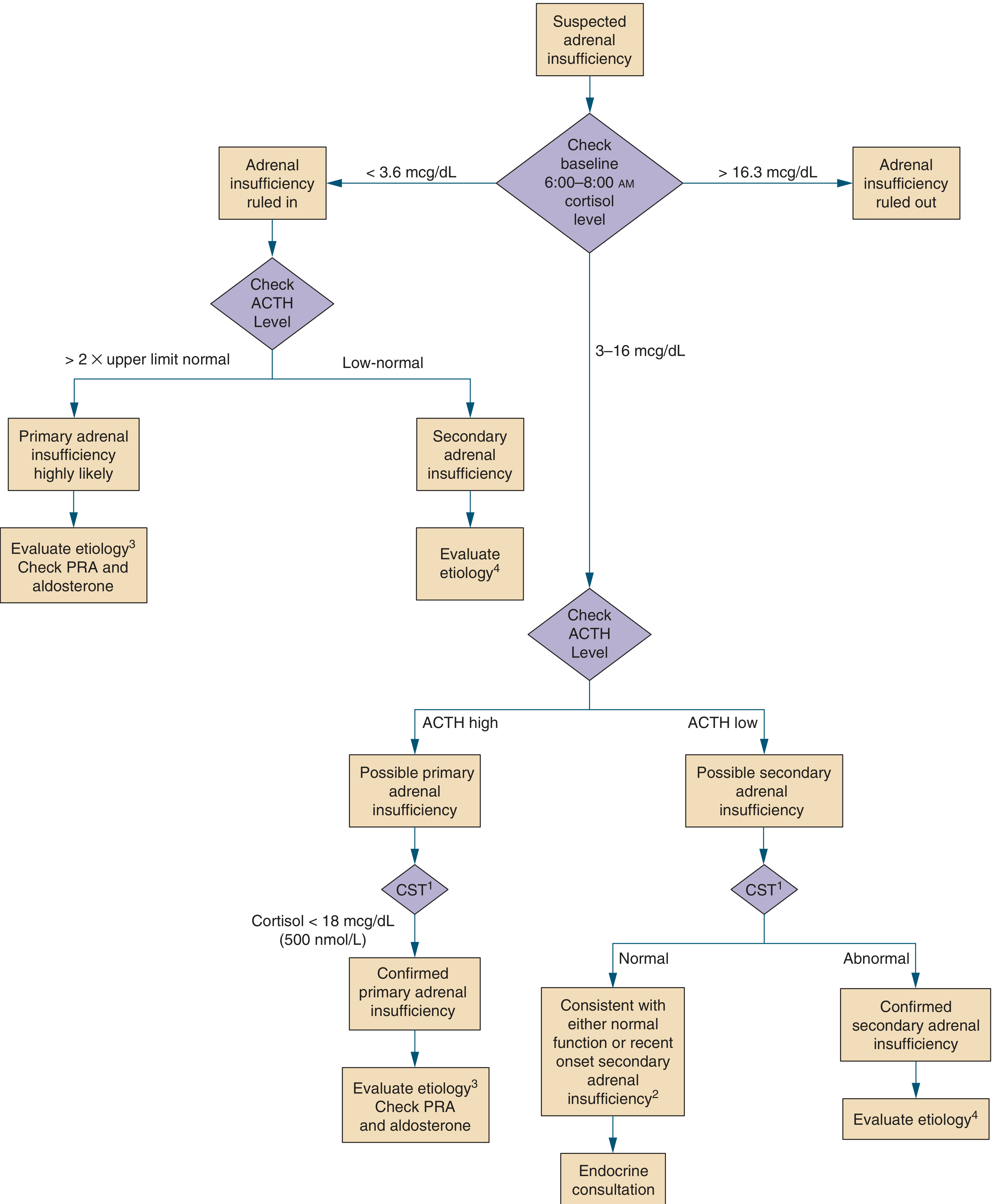
Bottom Line: Next Steps in Order
- Exclude exogenous steroid use (most common cause)
- Cosyntropin stimulation test - confirm AI (may be false-negative if recent onset)
- Pituitary MRI - identify structural cause
- Assess all pituitary axes - look for panhypopituitarism
- CRH test or ITT if needed to distinguish pituitary vs. hypothalamic level
- Treat: glucocorticoid replacement (hydrocortisone); mineralocorticoid replacement is NOT needed
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed., p. 433-434
- Textbook of Family Medicine, 9th ed.
- Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.