Brachial plexus
Reading File
Finding Sources
Searching the Web
brachial plexus anatomy roots trunks divisions cords branches
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive information to produce a thorough answer. Let me compile it.
Brachial Plexus
Overview
The brachial plexus is a somatic nerve network formed by the anterior rami of C5, C6, C7, C8, and T1. It originates in the neck, passes laterally and inferiorly over rib I between the anterior and middle scalene muscles, and enters the axilla, where its cords surround the axillary artery. It provides all motor and sensory innervation to the upper limb.
- Gray's Anatomy for Students, p. 858
Structure: Roots - Trunks - Divisions - Cords - Branches
The classic mnemonic: "Read That Damn Cadaver Book" (Roots, Trunks, Divisions, Cords, Branches).
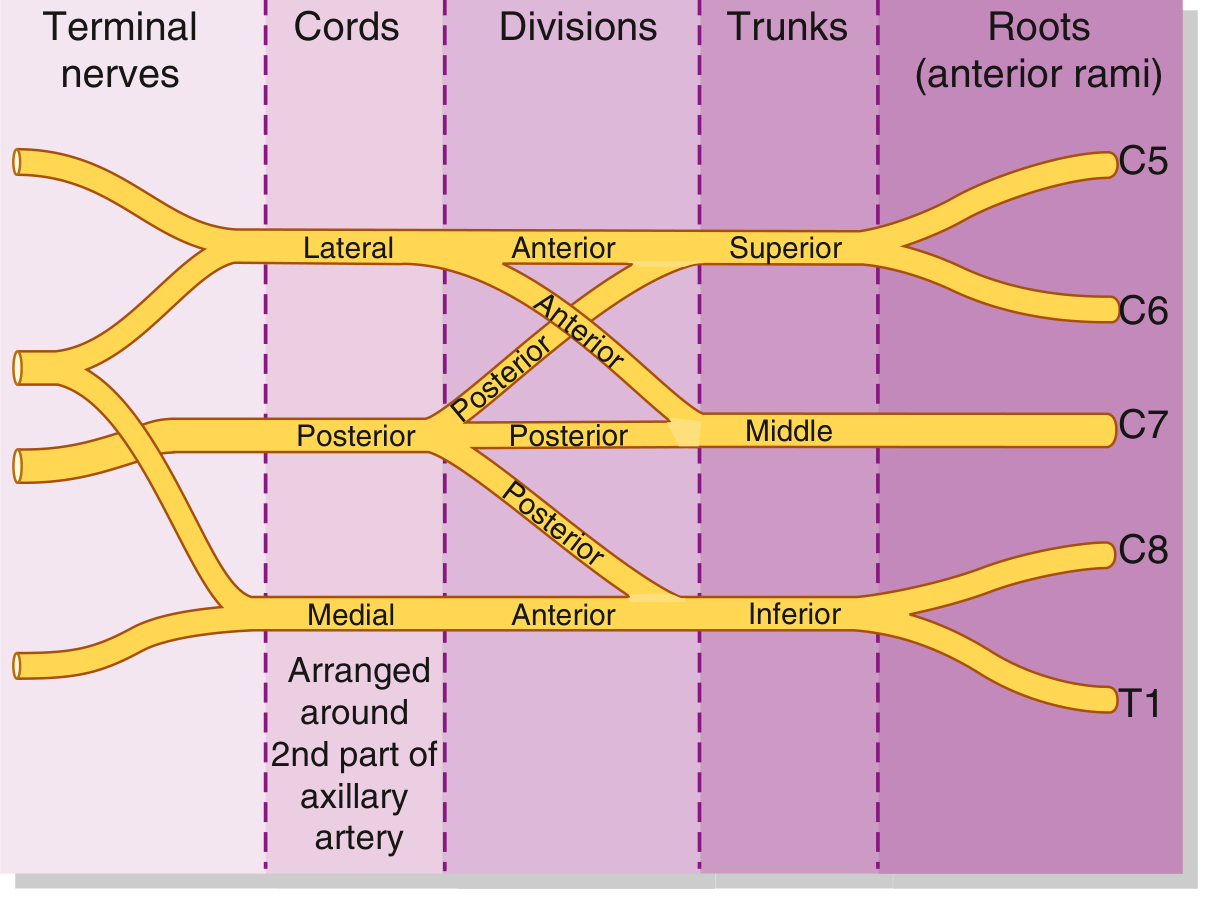
Fig. Schematic of the brachial plexus - Gray's Anatomy for Students
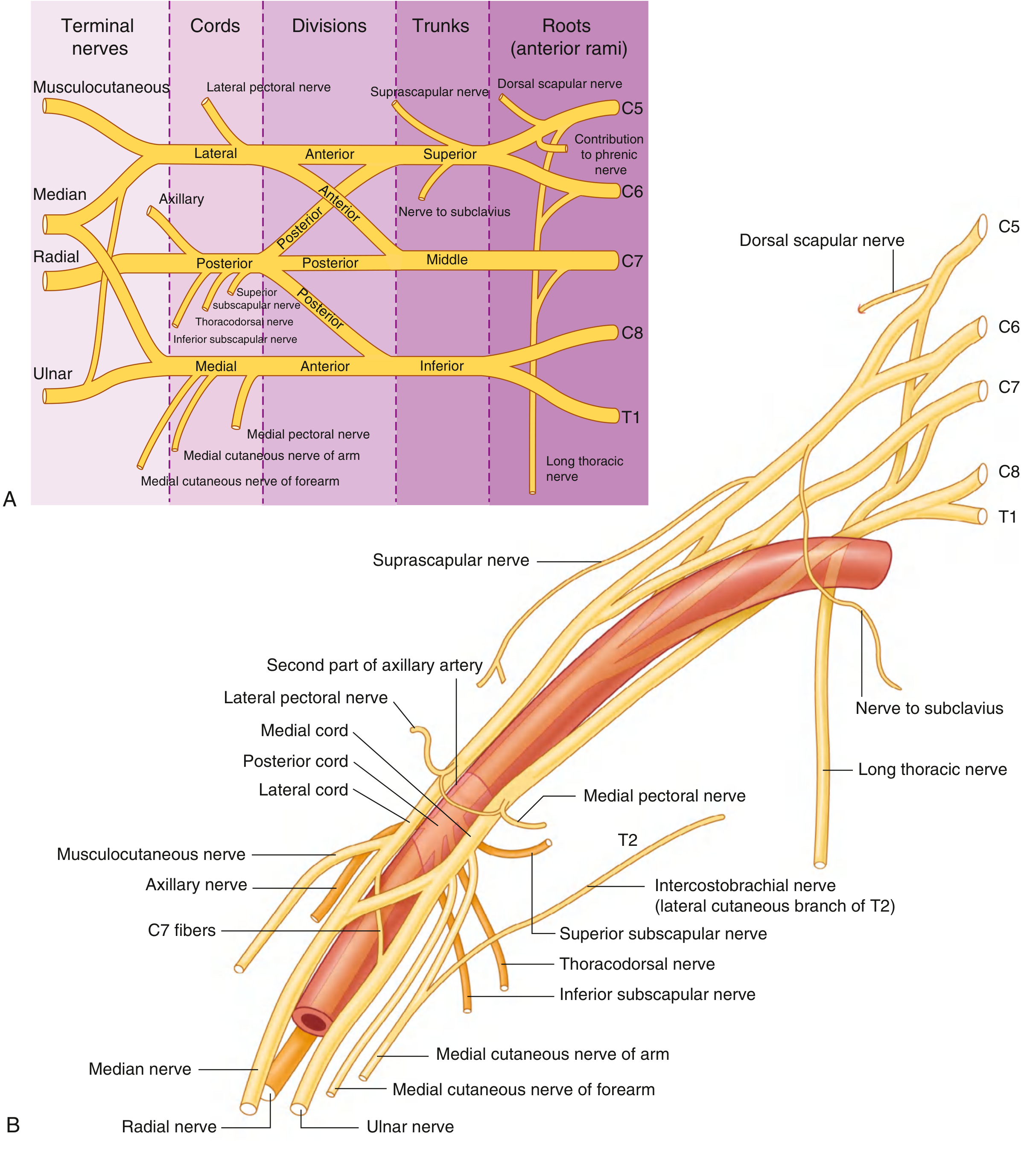
Fig. Brachial plexus branches and their relationships to the axillary artery - Gray's Anatomy for Students
1. Roots (Anterior Rami)
| Root | Notes |
|---|---|
| C5 | Gives dorsal scapular nerve, contributes to phrenic nerve |
| C6 | Joins C5 to form superior trunk |
| C7 | Continues as middle trunk |
| C8 | Joins T1 to form inferior trunk |
| T1 | Gives gray rami communicantes from the sympathetic trunk |
The roots pass between the anterior and middle scalene muscles. They receive gray rami communicantes (postganglionic sympathetic fibers) from the sympathetic trunk.
2. Trunks
| Trunk | Formation | Position |
|---|---|---|
| Superior | C5 + C6 | Above subclavian artery |
| Middle | C7 alone | Above subclavian artery |
| Inferior | C8 + T1 | On rib I, posterior to subclavian artery |
The trunks cross the base of the posterior triangle of the neck.
3. Divisions
Each trunk splits into an anterior and posterior division (6 divisions total). No named peripheral nerves arise directly from the divisions.
- Anterior divisions - supply anterior (flexor) compartments
- Posterior divisions - supply posterior (extensor) compartments
4. Cords
Named by their position relative to the second part of the axillary artery:
| Cord | Formation | Roots | Position |
|---|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5-C7 | Lateral to axillary artery |
| Medial | Anterior division of inferior trunk | C8-T1 | Medial to axillary artery |
| Posterior | All three posterior divisions | C5-T1 | Posterior to axillary artery |
5. Branches
From the Roots
| Nerve | Root | Supplies |
|---|---|---|
| Dorsal scapular nerve | C5 | Rhomboid major, rhomboid minor, levator scapulae |
| Long thoracic nerve | C5, C6, C7 | Serratus anterior (injury = medial winging of scapula) |
| Contribution to phrenic nerve | C5 | Diaphragm (small contribution) |
From the Trunks (Superior trunk only)
| Nerve | Supplies |
|---|---|
| Suprascapular nerve (C5, C6) | Supraspinatus, infraspinatus |
| Nerve to subclavius (C5, C6) | Subclavius |
From the Lateral Cord
| Nerve | Supplies |
|---|---|
| Lateral pectoral nerve (C5-C7) | Pectoralis major (clavicular head) |
| Musculocutaneous nerve (C5-C7) | Coracobrachialis, biceps brachii, brachialis; sensory - lateral forearm |
| Lateral root of median nerve | (contributes to median nerve) |
From the Medial Cord
| Nerve | Supplies |
|---|---|
| Medial pectoral nerve (C8, T1) | Pectoralis major and minor |
| Medial cutaneous nerve of arm (C8, T1) | Skin - medial distal arm |
| Medial cutaneous nerve of forearm (C8, T1) | Skin - medial forearm |
| Ulnar nerve (C8, T1) | Intrinsic hand muscles, medial 1.5 fingers |
| Medial root of median nerve | (contributes to median nerve) |
From the Posterior Cord
| Nerve | Supplies |
|---|---|
| Superior subscapular nerve (C5, C6) | Subscapularis (upper) |
| Thoracodorsal nerve (C6-C8) | Latissimus dorsi |
| Inferior subscapular nerve (C5, C6) | Subscapularis (lower), teres major |
| Axillary nerve (C5, C6) | Deltoid, teres minor; sensory - regimental badge area |
| Radial nerve (C5-T1) | All posterior compartment muscles of arm and forearm |
A useful axilla landmark: the musculocutaneous nerve, lateral root of median nerve, median nerve, medial root of median nerve, and ulnar nerve form an "M" shape over the third part of the axillary artery. - Gray's Anatomy for Students, p. 865
Terminal (5 Major) Nerves Summary
| Nerve | Origin | Key function |
|---|---|---|
| Musculocutaneous | Lateral cord | Elbow flexion; lateral forearm sensation |
| Median | Lateral + medial cord | Forearm pronation/wrist flexion, thumb opposition, lateral palm |
| Ulnar | Medial cord | Intrinsic hand muscles, medial 1.5 fingers |
| Radial | Posterior cord | Elbow/wrist/finger extension, posterior arm + forearm sensation |
| Axillary | Posterior cord | Shoulder abduction (deltoid), shoulder patch sensation |
Clinical: Brachial Plexus Injuries
Erb-Duchenne Palsy (Upper Plexus - C5, C6)
Mechanism: Forceful widening of the angle between neck and shoulder - motorcycle accidents, shoulder dystocia at birth (most common neonatal brachial plexus injury).
Muscles affected: Deltoid, biceps, brachialis, brachioradialis, supinator.
Classic posture: Arm internally rotated, extended at elbow, pronated - "Policeman's tip" or "waiter's tip" position.
Sensory loss: Lateral arm and upper lateral forearm.
Klumpke's Palsy (Lower Plexus - C8, T1)
Mechanism: Forceful hyperabduction of the arm - grabbing a branch while falling, difficult breech delivery (arms above head).
Muscles affected: Intrinsic hand muscles (combined median + ulnar palsy pattern) = claw hand.
Sensory loss: Medial forearm, medial hand, medial 1.5 fingers.
Associated finding: Horner's syndrome (ptosis, miosis, enophthalmos, anhidrosis) - due to interruption of sympathetic fibers from T1, indicating a preganglionic lesion. This is a key indicator of severity.
Complete Brachial Plexus Lesion
Rare - severe trauma only. Results in complete paralysis and anesthesia of the entire upper limb (except the upper medial arm, supplied by intercostobrachial nerve from T2, and the upper lateral arm via axillary contributions from C3-C4).
Preganglionic vs. Postganglionic Injury
| Feature | Preganglionic | Postganglionic |
|---|---|---|
| Site | Root avulsion from spinal cord | Distal to dorsal root ganglion |
| Horner's syndrome | Present (if T1 involved) | Absent |
| Histamine test | Flare present (DRG intact) | No flare |
| Repair potential | Poor - cannot graft | Better - can repair/graft |
| Sensory nerve action potential | Present (axon intact) | Absent |
Clinical: Brachial Plexus Blocks (Anesthesia)
Different approaches target different levels of the plexus:
| Approach | Level blocked | Coverage | Uses |
|---|---|---|---|
| Interscalene | Roots/upper trunks (C5-C7) | Shoulder, proximal arm | Shoulder surgery |
| Supraclavicular | Trunks | Entire arm below shoulder | Arm/forearm surgery |
| Infraclavicular | Cords | Arm, forearm, hand | Elbow/hand surgery |
| Axillary | Terminal branches | Elbow, forearm, hand | Hand/wrist surgery |
"Brachial plexus block at the level of the cords provides excellent anesthesia for procedures at or distal to the elbow. The upper arm and shoulder are not anesthetized." - Morgan & Mikhail's Clinical Anesthesiology, 7e
Axillary block is considered the safest approach (no risk of pneumothorax), while interscalene block reliably blocks C5-C7 but has the highest risk of phrenic nerve palsy (ipsilateral hemidiaphragm paresis in virtually all patients).
Other Notable Conditions
- Thoracic outlet syndrome - Compression of lower trunk (C8-T1) and subclavian vessels between the clavicle and first rib; causes hand weakness and medial arm/forearm paresthesias.
- Pancoast tumor - Apical lung tumor invading lower brachial plexus + sympathetic chain; causes Horner's + C8-T1 distribution weakness.
- Parsonage-Turner syndrome (neuralgic amyotrophy) - Acute inflammatory plexopathy; sudden severe shoulder pain followed by weakness; often post-viral or post-vaccination.
Sources: Gray's Anatomy for Students (9780323934237), S. Das Manual of Clinical Surgery (9788190568104), Bradley & Daroff's Neurology in Clinical Practice (9780323642613), Morgan & Mikhail's Clinical Anesthesiology 7e
This is a shared conversation. Sign in to Orris to start your own chat.