Bone formation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bone formation" AND "osteoblast" AND "ossification"
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks and excellent images. Let me compile the full response.
Bone Formation (Osteogenesis)
Bone is a specialized connective tissue whose distinguishing feature is a mineralized extracellular matrix - calcium phosphate in the form of hydroxyapatite crystals [Ca₁₀(PO₄)₆(OH)₂] deposited on a type I collagen scaffold.
Bone Structure - Overview
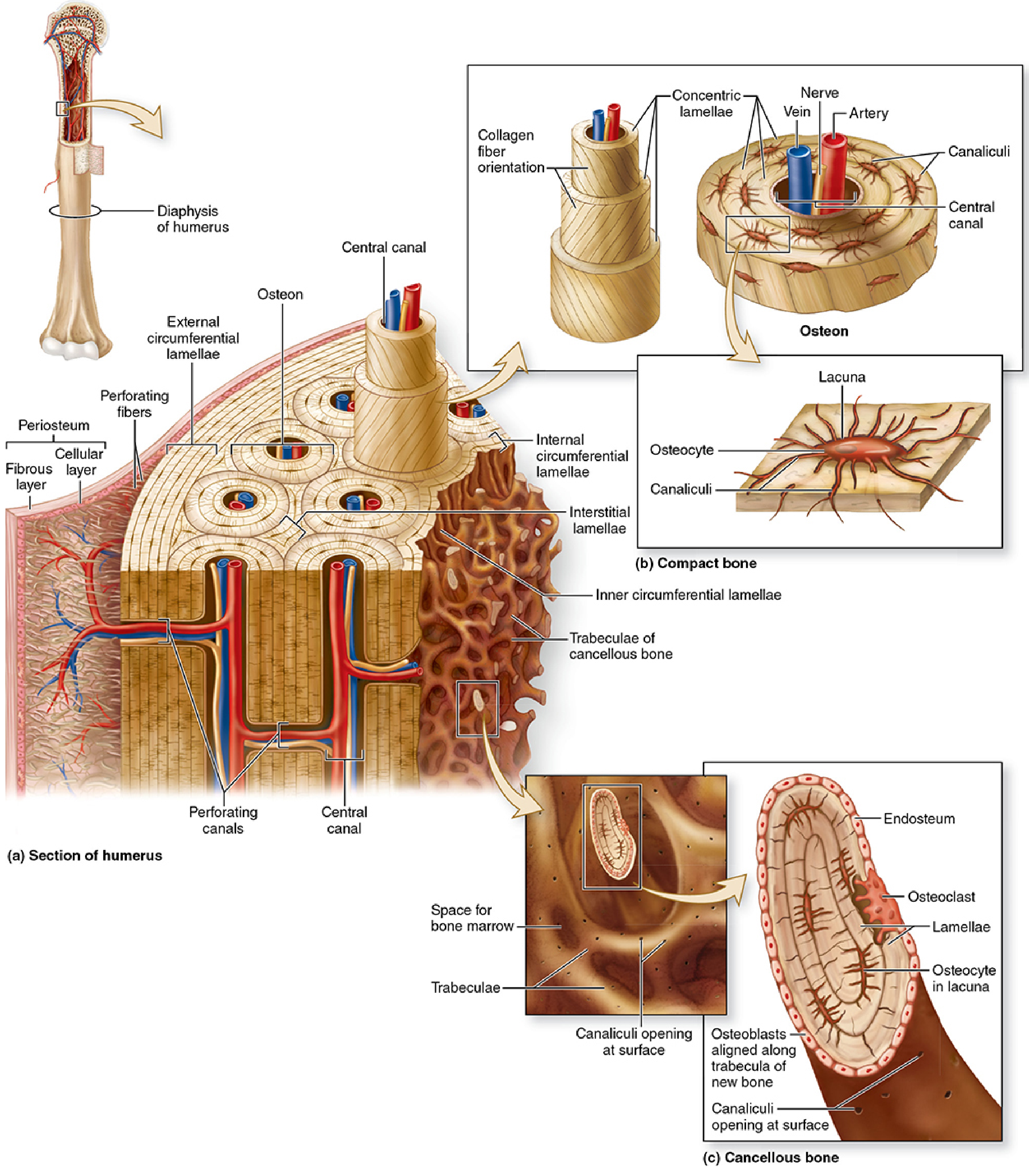
Figure: Bone structure showing compact bone (osteons, concentric lamellae, canaliculi) and cancellous bone (trabeculae). - Junqueira's Basic Histology, 17e
Three key cell types:
| Cell | Origin | Function |
|---|---|---|
| Osteoblast | Mesenchymal stem cells / osteoprogenitor cells | Synthesize and secrete osteoid (unmineralized matrix); driven by RUNX2/CBFA1 transcription factor |
| Osteocyte | Trapped osteoblasts | Maintain calcified matrix; sense mechanical load via canalicular network |
| Osteoclast | Monocyte/macrophage lineage | Resorb bone; activated via RANK-RANKL signaling |
Bone matrix composition:
- ~90% type I collagen (minor amounts of type III, V, XI, XIII)
- ~10% noncollagenous proteins: proteoglycans (chondroitin sulfate, keratan sulfate), glycoproteins (osteocalcin, osteonectin, bone sialoprotein), growth factors, and lipids
Two Types of Bone Formation
1. Intramembranous Ossification
Bone forms directly from mesenchyme, without a cartilage intermediate.
Bones formed this way: Flat bones of the skull, mandible, clavicle.
Steps:
- Mesenchymal cells migrate and aggregate at an ossification center (~8th week of embryonic development)
- These cells express the CBFA1/RUNX2 transcription factor and differentiate into osteoprogenitor cells, then osteoblasts
- Osteoblasts secrete osteoid (type I collagen, bone sialoproteins, osteocalcin)
- Osteoid undergoes mineralization; trapped osteoblasts become osteocytes
- Spicules and trabeculae form first as woven (primary) bone
- Vascular connective tissue invades spaces between trabeculae → becomes bone marrow
- Woven bone is remodeled by osteoclasts and replaced by lamellar (secondary) bone
- Outer surfaces condense to form compact bone plates; inner spongy bone persists
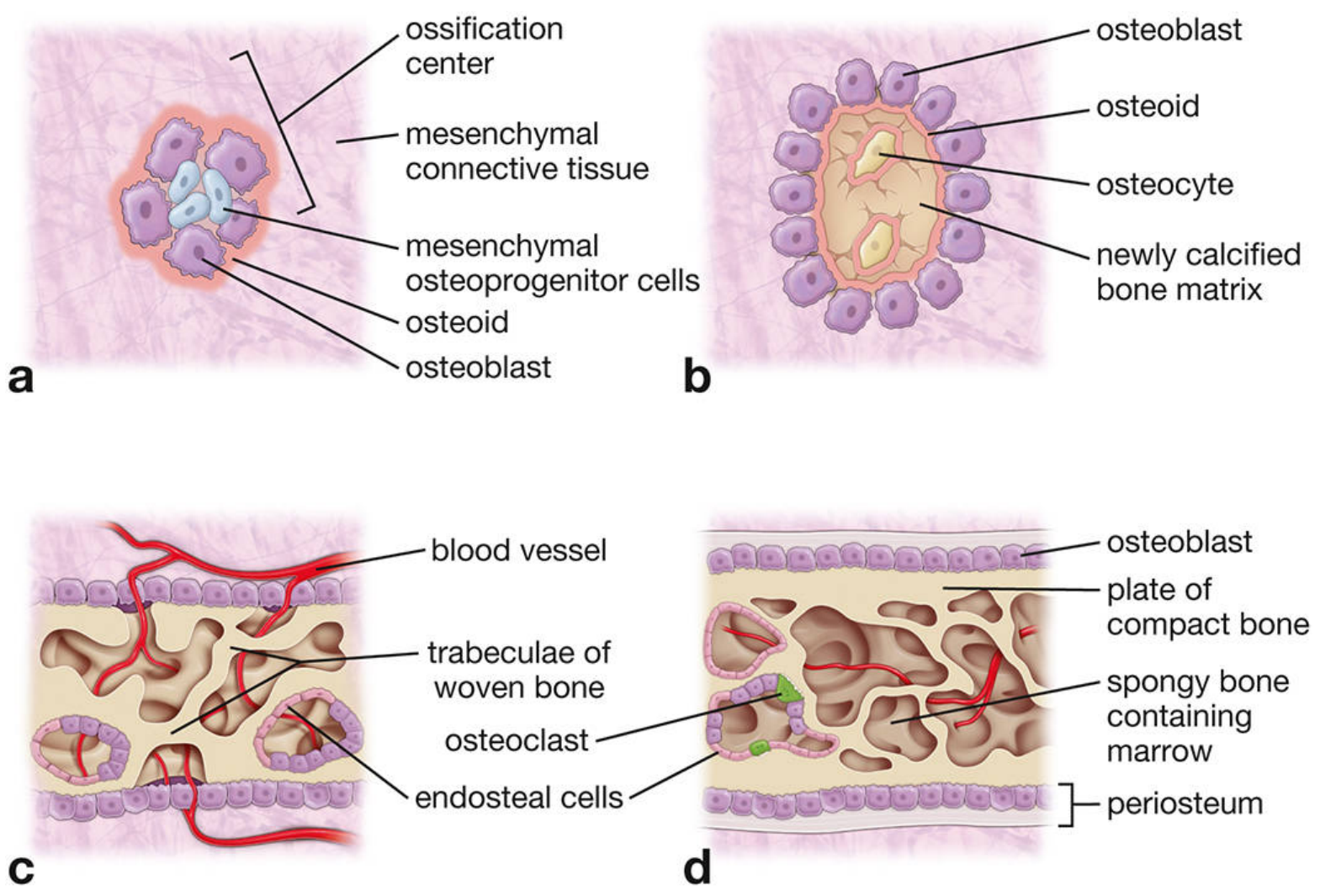
Figure 8.18: Intramembranous ossification. (a) Mesenchymal osteoprogenitor cells aggregate at the ossification center. (b) Osteoblasts at periphery secrete osteoid; osteocytes form at center. (c) Woven bone trabeculae with invading blood vessels. (d) Mature bone with compact outer plates, spongy center, and periosteum. - Histology: A Text and Atlas, 9e
2. Endochondral Ossification
Bone forms by replacing a hyaline cartilage template (anlage). This is the mechanism for all long bones, vertebrae, ribs, and the base of the skull.
Steps:
- Mesenchymal cells form a hyaline cartilage model of the future bone
- Chondrocytes in the center of the diaphysis hypertrophy; the matrix mineralizes
- A periosteal bony collar (intramembranous) forms around the mid-diaphysis
- Blood vessels and osteoprogenitor cells invade the calcified cartilage → primary ossification center at the diaphysis (~8 weeks gestation)
- The medullary canal is created as cartilage is resorbed
- Ossification progresses toward the epiphyses
- After birth, secondary ossification centers form in the epiphyses
- A plate of cartilage is entrapped between the two expanding centers → epiphyseal growth plate (physis)
Epiphyseal Growth Plate Zones (diaphysis → epiphysis):
| Zone | Description |
|---|---|
| Reserve (resting) zone | Small, inactive chondrocytes in hyaline cartilage; source of new cells |
| Proliferating zone | Chondrocytes divide rapidly, forming stacks/columns |
| Hypertrophic zone | Cells enlarge; matrix calcifies |
| Zone of calcification / apoptosis | Chondrocytes undergo apoptosis; matrix mineralizes |
| Zone of ossification (primary spongiosa) | Capillaries and osteoblasts invade; osteoid deposited on calcified cartilage spicules → trabecular bone |
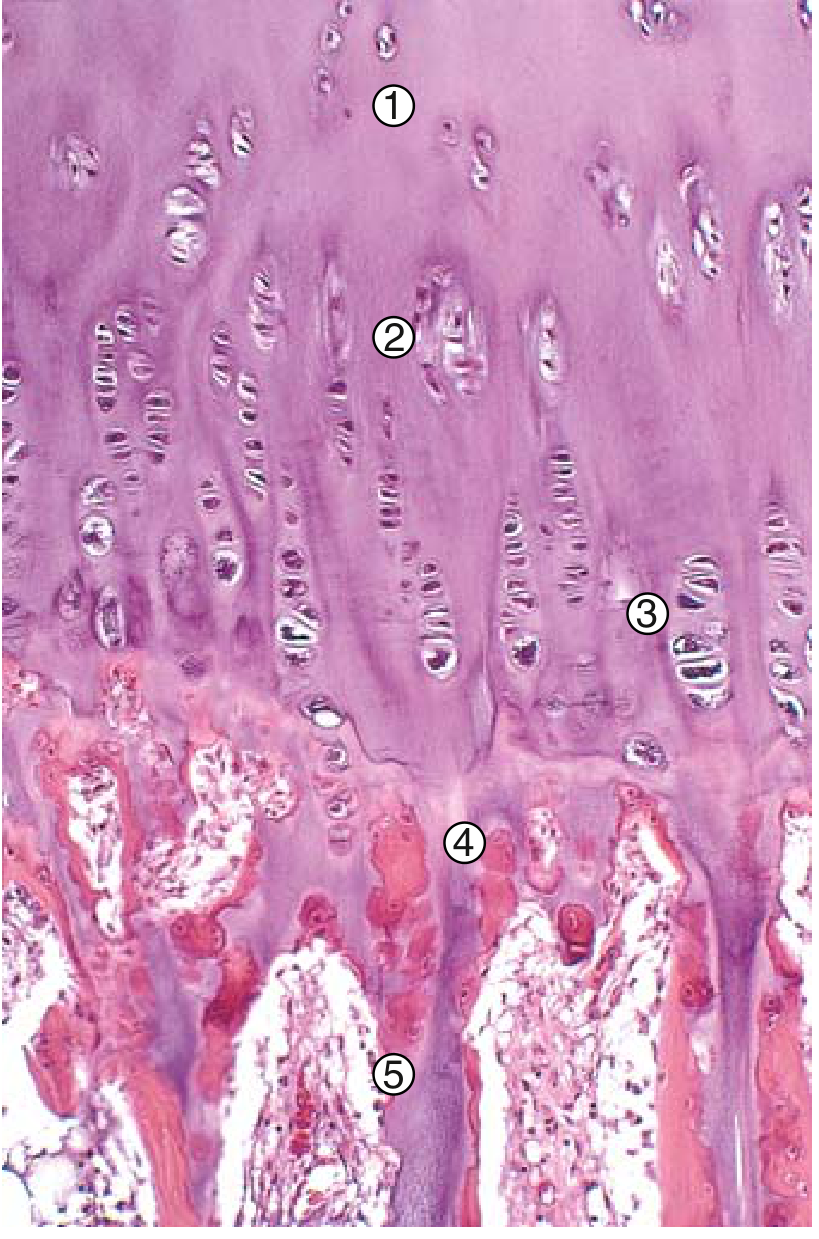
Figure 19.3: Active growth plate. 1 = Reserve zone. 2 = Proliferation. 3 = Hypertrophy. 4 = Apoptosis/mineralization. 5 = Primary spongiosa. - Robbins & Kumar Basic Pathology
Longitudinal bone growth depends on interstitial proliferation of chondrocytes in the growth plate. Radial (width) growth occurs by appositional bone deposition from the periosteum.
Bone Remodeling (Throughout Life)
After formation, bone undergoes continuous remodeling by Bone Multicellular Units (BMUs) - small clusters of osteoclasts followed by osteoblasts.
RANK-RANKL-OPG axis (key regulatory pathway):
- Osteoblasts, stromal cells, and T lymphocytes express RANKL on their surface
- RANKL binds RANK on monocyte precursors → monocytes differentiate into osteoclasts
- Osteoprotegerin (OPG) acts as a decoy receptor, competes with RANK for RANKL binding → inhibits osteoclastogenesis
Osteoclast resorption mechanism:
- Osteoclast attaches to bone via integrins in the sealing zone
- H⁺-ATPase proton pumps acidify the compartment to ~pH 4.0 → hydroxyapatite dissolves
- Lysosomal proteases (cathepsins) degrade collagen
- Products are transcytosed and released; collagen pyridinoline breakdown products appear in urine as markers of bone resorption
Remodeling rates:
- Infants: calcium turnover ~100%/year
- Adults: ~18%/year
Hormonal Regulation of Bone
| Hormone | Effect on Bone |
|---|---|
| PTH | Stimulates osteoclast-mediated resorption (indirect, via RANK-RANKL on osteoblasts; osteoclasts lack PTH receptors) → raises blood Ca²⁺ |
| Calcitonin | Inhibits osteoclast activity → lowers blood Ca²⁺ |
| 1,25-(OH)₂ Vitamin D | Promotes Ca²⁺ absorption; supports matrix mineralization |
| Estrogen/Testosterone | Inhibit osteoclastogenesis; loss at menopause → increased resorption → osteoporosis |
| Growth hormone / IGF-1 | Stimulate chondrocyte proliferation in growth plate |
| Glucocorticoids (excess) | Suppress osteoblast function; increase osteoclast activity → bone loss |
Key Transcription Factors in Bone Formation
- RUNX2 (CBFA1): Master regulator of osteoblast differentiation. Knockout mice are born with an entirely cartilaginous skeleton - no ossification occurs.
- Osterix (SP7): Downstream of RUNX2; required for osteoblast maturation and matrix secretion.
- Hedgehog signaling (Ihh): Required for both endochondral and intramembranous ossification; mediates osteoblastogenesis in response to mechanical load.
- FGF receptor-3 (FGFR3): Regulates endochondral ossification in long bones. Activating mutations cause achondroplasia (premature growth plate closure, shortening of long bones).
Woven vs. Lamellar Bone
| Feature | Woven (Primary) Bone | Lamellar (Secondary) Bone |
|---|---|---|
| Collagen arrangement | Random, irregular | Parallel, organized layers |
| Mineral content | Lower | Higher |
| When present | Fetal bone, fracture repair, Paget disease, osteosarcoma | Normal adult bone |
| Strength | Weaker | Stronger |
Clinical Correlations
- Achondroplasia: Gain-of-function mutation in FGFR3 → inhibits endochondral ossification → dwarfism
- Osteoporosis: Imbalance between osteoclast resorption and osteoblast formation (resorption > formation); trabecular thinning
- Scurvy: Vitamin C deficiency → impaired collagen synthesis → defective osteoid
- Rickets/Osteomalacia: Vitamin D deficiency → failure of osteoid mineralization; widened growth plate zones
- Paget disease: Dysregulated remodeling; initial osteoclastic resorption followed by disorganized woven bone formation
- Fracture healing: Periosteal cells form a fibrocartilage soft callus → replaced by woven bone (hard callus) → remodeled to lamellar bone
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, 9e, Chapter 8
- Junqueira's Basic Histology: Text and Atlas, 17e, Chapter 8
- Ganong's Review of Medical Physiology, 26e, Chapter 21
- Robbins & Kumar Basic Pathology, Chapter 19
This is a shared conversation. Sign in to Orris to start your own chat.