Infective endocarditis
Reading File
Finding Sources
Searching PubMed
"infective endocarditis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
I have enough comprehensive information. Let me compile a thorough response on infective endocarditis:
Infective Endocarditis
Definition
Infective endocarditis (IE) is a microbial infection of the heart valves or endocardium that leads to the formation of vegetations composed of thrombotic debris and microorganisms, often associated with destruction of the underlying cardiac tissue. The aorta, aneurysmal sacs, other blood vessels, and prosthetic devices may also be involved. The vast majority of cases are bacterial, though fungi, rickettsiae (Q fever), and chlamydial species can also cause IE.
- Robbins & Kumar Basic Pathology
Classification: Acute vs. Subacute
| Feature | Acute IE | Subacute IE |
|---|---|---|
| Tempo | Days to weeks | Weeks to months |
| Common organisms | S. aureus | Viridans streptococci |
| Valve involvement | Normal or abnormal valves | Usually abnormal valves |
| Course | Highly destructive, high mortality | Indolent, better prognosis |
| Manifestations | Fever, chills, rapid hemodynamic compromise | Fatigue, weight loss, flu-like, low-grade fever |
- Robbins & Kumar Basic Pathology
Epidemiology
-
Global incidence in developed countries: estimated 3-10 cases per 100,000 person-years, rising due to healthcare-associated infections and the opioid epidemic.
-
S. aureus has become the most common causative organism in high-income countries, largely due to healthcare exposure (indwelling catheters, hemodialysis, cardiac devices) and IV drug use.
-
Rheumatic heart disease remains the dominant predisposing condition in developing countries, causing subacute streptococcal IE in younger adults.
-
Aging populations in developed countries have increased rates of degenerative valvular disease (mitral valve prolapse, calcific aortic stenosis) as predisposing substrates.
-
Braunwald's Heart Disease
Microbiology
The three most common groups worldwide are staphylococci, streptococci, and enterococci:
| Organism | Typical Setting | Notes |
|---|---|---|
| Streptococcus viridans | Community-acquired, damaged/deformed valves | Subacute IE; normal oral flora |
| S. aureus | Healthcare-associated, IV drug users, healthy valves | Most common in high-income countries; acute IE |
| Enterococci | Elderly, healthcare-associated | Requires combination therapy |
| HACEK group | Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella | Slow-growing oral flora |
| Fungi | Immunocompromised, prosthetic valves | Rare; poor prognosis |
| Culture-negative | ~10% of cases | Prior antibiotics or fastidious organisms (e.g., Coxiella burnetii, Bartonella) |
- Robbins & Kumar Basic Pathology; Braunwald's Heart Disease
Pathogenesis
- Endothelial disruption - turbulent blood flow from underlying valvular or congenital disease damages the endothelium, creating a nidus for platelet-fibrin deposition (non-bacterial thrombotic endocarditis/NBTE).
- Bacteremia - organisms enter the bloodstream via dental procedures, skin/mucous membrane breaches, IV drug use, indwelling catheters, or trivial daily activities.
- Colonization - organisms adhere to NBTE via surface adhesins (fibronectin-binding proteins in S. aureus, dextran in streptococci).
- Vegetation formation - organisms proliferate within the platelet-fibrin matrix, recruiting more thrombus and evading host defenses (organisms deep within the vegetation are metabolically inactive and hard to kill).
Key predisposing cardiac conditions: rheumatic heart disease, mitral valve prolapse (now the leading preexistent risk factor in developed countries), bicuspid aortic valve, calcific valvular stenosis, prosthetic valves (10-20% of all IE cases), pacemaker leads and cardiac implantable electronic devices (CIEDs).
- Braunwald's Heart Disease; Robbins & Kumar Basic Pathology
Morphology / Pathology
Vegetations in IE are friable, bulky, and destructive, found on the valve leaflets (typically the atrial surface of AV valves and ventricular surface of semilunar valves). They contain:
- Fibrin, platelets, inflammatory cells
- Large numbers of organisms
Sites of involvement:
- Aortic and mitral valves most common (left-sided IE)
- Tricuspid valve - frequent in IV drug users (right-sided IE)
- Vegetations may be single or multiple, and may erode into myocardium to form a ring abscess
Consequences of friable vegetations:
- Embolization - septic emboli lodge distally causing abscesses, septic infarcts
- Mycotic aneurysms - from bacterial seeding of arterial walls at embolic sites
- Valve perforation, chordal rupture - causing acute regurgitation
Clinical Features
Symptoms
- Fever - the most consistent sign (present in >90%); may be absent in elderly or those with subacute disease
- Constitutional symptoms: fatigue, malaise, anorexia, weight loss, night sweats
- Arthralgias, myalgias
- Symptoms of embolic events: stroke, flank pain, abdominal pain
Signs
Peripheral stigmata (immune complex or embolic):
| Sign | Description | Mechanism |
|---|---|---|
| Osler nodes | Painful, tender subcutaneous nodules in fingertip pulp | Immune complex deposition |
| Janeway lesions | Painless, erythematous/hemorrhagic macules on palms/soles | Septic emboli |
| Roth spots | Boat-shaped retinal hemorrhages with pale center | Immune complex vasculitis |
| Splinter hemorrhages | Linear dark lines under nails | Microemboli |
| Petechiae | Conjunctival, mucous membranes, skin | Microemboli |
-
Heart murmur: present in ~90% of left-sided IE; new or changing murmur is particularly significant
-
Splenomegaly: common in subacute disease
-
Clubbing: in long-standing subacute IE
-
Robbins & Kumar Basic Pathology; Harriet Lane Handbook; Goldman-Cecil Medicine
Diagnosis: Modified Duke Criteria
The modified Duke criteria (published 2000, updated 2015) are the standard diagnostic framework. A definite diagnosis requires:
- 2 major criteria, OR
- 1 major + 3 minor criteria, OR
- 5 minor criteria
"Possible" IE: 1 major + 1 minor, or 3 minor criteria.
Major Criteria
1. Blood culture positive for IE
- Typical organisms (viridans streptococci, S. gallolyticus, S. aureus, HACEK, community-acquired enterococci) from ≥2 separate blood cultures, OR
- Persistently positive blood cultures: ≥2 positive from samples drawn >12 hours apart, or 3-4 of ≥4 cultures with first and last ≥1 hour apart
- Single positive culture for Coxiella burnetii (Q fever), or anti-phase I IgG titer ≥1:800
2. Evidence of endocardial involvement (echocardiography)
- Oscillating intracardiac mass on valve/supporting structures (vegetation)
- Abscess
- New partial dehiscence of prosthetic valve
- New valvular regurgitation (worsening of pre-existing murmur is NOT sufficient)
Minor Criteria
- Predisposing heart condition or IV drug use
- Fever >38°C
- Vascular phenomena: major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhage, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Microbiologic evidence: positive blood culture not meeting major criteria (excludes single positive for coagulase-negative staphylococci)
- Braunwald's Heart Disease; Washington Manual of Medical Therapeutics
Echocardiography
Transthoracic echo (TTE): First-line study; good for native valves in patients with good acoustic windows.
Transesophageal echo (TEE): Recommended when:
- TTE is of poor quality or negative despite high clinical suspicion
- Prosthetic valve is involved
- S. aureus bacteremia
- Suspected perivalvular abscess or fistula
- TEE has higher sensitivity for small vegetations, perforations, and abscesses
Cardiac CT (MDCTA): Sensitivity of 100% for perivalvular extension vs. 89% for TEE in some series; best for surgical planning and coronary artery assessment prior to surgery.
18F-FDG PET/CT: Increases sensitivity from ~60-70% to 87-97% for prosthetic valve IE and cardiac implantable device IE; proposed as additional major Duke criterion for prosthetic device IE.
Below is a TTE image of native aortic valve IE (Braunwald's):
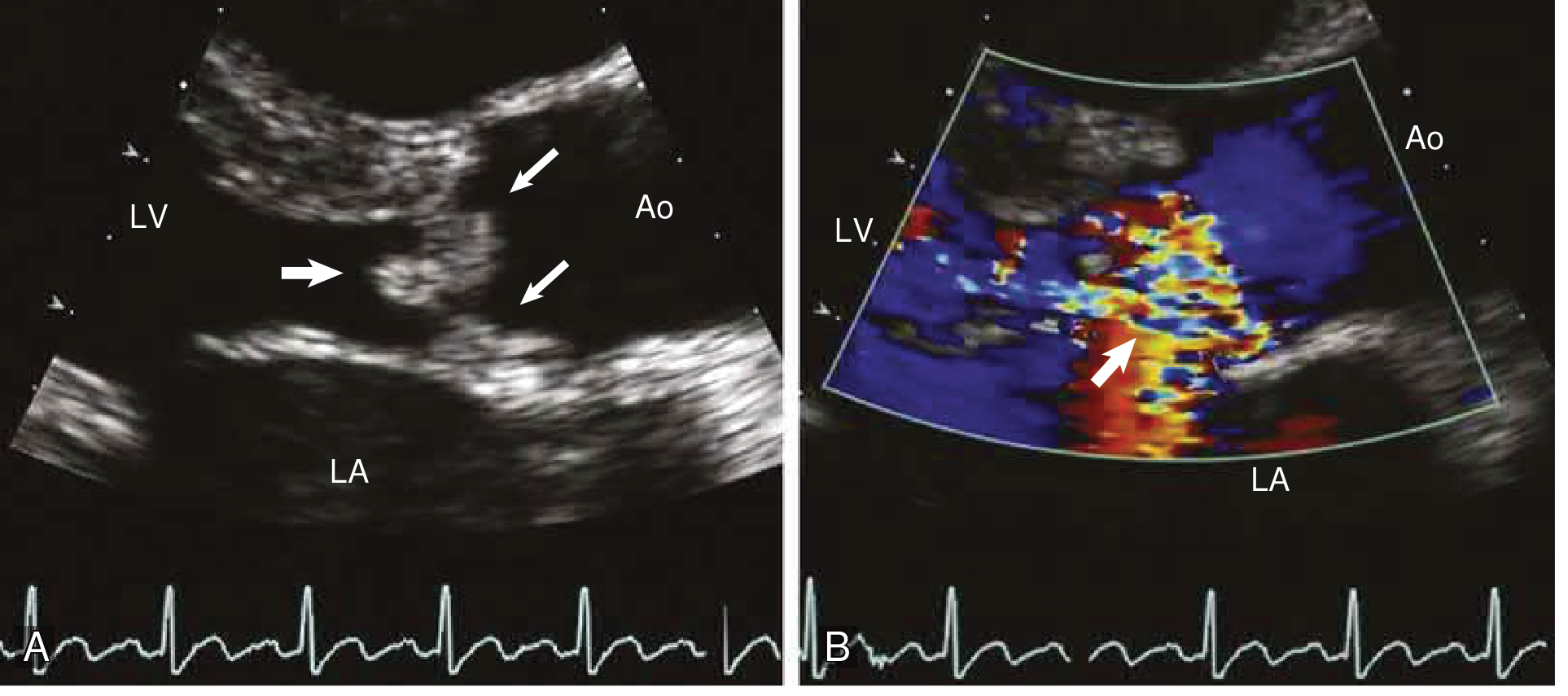
TTE (A) showing vegetations (arrows) attached to aortic valve cusps prolapsing into the LVOT during diastole. Color Doppler (B) showing severe aortic regurgitation. Ao = ascending aorta; LA = left atrium; LV = left ventricle.
- Braunwald's Heart Disease
Complications
| Complication | Notes |
|---|---|
| Valvular destruction | Regurgitation → acute hemodynamic compromise → heart failure |
| Perivalvular abscess | Extension into annulus/myocardium; seen in 20-40% of surgically treated IE; common with aortic IE and S. aureus |
| Embolic events | Incidence 20-50%; most common in first 2 weeks; CNS (38%) > spleen > renal > lung |
| Stroke | Ischemic (most common), hemorrhagic (mycotic aneurysm rupture) |
| Mycotic aneurysms | Intracranial most dangerous; risk of rupture |
| Glomerulonephritis | Immune complex deposition; microscopic hematuria, proteinuria |
| Arrhythmias/conduction defects | Extension to AV node/conduction system; new PR prolongation = perivalvular abscess |
| Metastatic abscesses | Spleen, kidneys, brain, vertebrae |
Treatment
General Principles
- All IE patients require inpatient management at a center with multidisciplinary IE team (infectious disease, cardiology, cardiac surgery).
- Blood cultures must be drawn before starting antibiotics.
- Duration of IV antibiotics: typically 4-6 weeks (longer for prosthetic valve IE or complicated disease).
- The bactericidal nature of the regimen is essential - organisms within vegetations are poorly accessible to antibiotics.
Antibiotic Regimens (Key Examples from Braunwald's)
Viridans streptococci / S. gallolyticus (native valve, penicillin-susceptible MIC ≤0.12 μg/mL):
- Aqueous crystalline penicillin G 12-18 million U/day IV continuously or q4h × 4 weeks, OR
- Ceftriaxone 2 g/day IV/IM × 4 weeks
- Alternatively: 2-week regimen with penicillin/ceftriaxone + gentamicin 3 mg/kg/day (in uncomplicated cases, non-elderly)
- Vancomycin 30 mg/kg/day IV in 2 divided doses × 4 weeks (penicillin-allergic patients only)
Penicillin-resistant viridans streptococci (MIC >0.12 μg/mL):
- Penicillin G or ceftriaxone + gentamicin × 6 weeks (prosthetic valve) or 4 weeks (native valve)
Staphylococci (native valve, MSSA):
- Nafcillin or oxacillin (anti-staphylococcal penicillin) × 6 weeks
- Cefazolin 6 g/day IV in 3 divided doses can be substituted (less CNS penetration)
Staphylococci (MRSA or prosthetic valve):
- Vancomycin 30 mg/kg/day IV in 2 divided doses × 6 weeks
- For prosthetic valve: vancomycin + rifampin × ≥6 weeks, plus gentamicin × 2 weeks
Enterococci:
- Penicillin or ampicillin + gentamicin (synergistic) × 4-6 weeks
- For high-level aminoglycoside resistance: ampicillin + ceftriaxone (double beta-lactam) × 6 weeks
Source: Braunwald's Heart Disease
Surgical Indications
Surgery is indicated (generally emergent/urgent) for:
- Heart failure due to valvular dysfunction (most common indication; surgery associated with improved survival)
- Uncontrolled infection - perivalvular abscess/fistula, prosthetic valve dehiscence, failure to sterilize blood cultures after 5-7 days of appropriate antibiotics, fungal/resistant organisms
- Prevention of emboli - large (>10 mm) mobile vegetations, particularly with prior embolic event or involving the anterior mitral leaflet
- Prosthetic valve endocarditis - early PVE (within 60 days of surgery) caused by staphylococci, fungi, or complicated infection
Timing matters: emergent surgery (same day/within 24 hours) for pulmonary edema or cardiogenic shock; urgent surgery (within days) for perivalvular extension or persistently positive cultures.
Prevention / Prophylaxis
The 2021 AHA Scientific Statement updated prophylaxis guidelines. Antibiotic prophylaxis before invasive dental procedures is indicated for high-risk conditions:
| High-Risk Conditions Requiring Prophylaxis |
|---|
| Prosthetic cardiac valves (including transcatheter-implanted) |
| Previous IE |
| Congenital heart disease - unrepaired cyanotic CHD, or repaired CHD with residual defects |
| Cardiac transplant recipients with valvulopathy |
| Left ventricular assist devices (LVADs) and implantable hearts |
Preferred regimen: Amoxicillin 2 g orally 30-60 min before the procedure.
Alternatives (penicillin-allergic): Azithromycin/clarithromycin 500 mg, or cephalexin 2 g (if not anaphylaxis-type allergy), or doxycycline (replaces clindamycin, which was removed due to risk of C. difficile infection).
Note: Clindamycin was eliminated from the 2021 guidelines.
- Braunwald's Heart Disease
Prognosis
- In-hospital mortality: 15-20% overall; up to 40-50% with severe complications (abscess, stroke, refractory heart failure).
- Adverse predictors: S. aureus infection, prosthetic valve, diabetes, age >65, renal failure, embolic events, perivalvular abscess, heart failure.
- Without treatment, IE is virtually always fatal.
- With appropriate antibiotics +/- surgery, most patients with native valve streptococcal IE can be cured.
Sources:
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine (Baddour, Anavekar, Crestanello, Wilson, Bonow)
- Robbins & Kumar Basic Pathology (Chapter 9)
- Goldman-Cecil Medicine (modified Duke criteria, minor criteria)
- The Washington Manual of Medical Therapeutics (diagnosis and Duke criteria)
- Fuster and Hurst's The Heart, 15th Edition (pathogenesis, management)
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
This is a shared conversation. Sign in to Orris to start your own chat.